
Case-Report | DOI: https://doi.org/10.31579/2641-0419/051
*Corresponding Author: Jhan Carlos Altamar, MD, Carrera 42h #84-33, Barranquilla, Colombia
Citation: La Ossa MD, Jhan C. Altamar, (2020) Posteroseptal Accessory Pathways Ablation: do not forget the Coronary Sinus Diverticulum. J. Clinical Cardiology and Cardiovascular Interventions, 3(4); Doi:10.31579/2641-0419/051
Copyright: © 2020 Jhan Carlos Altamar, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 26 February 2020 | Accepted: 09 March 2020 | Published: 16 March 2020
Keywords: accessory pathway; atrial fibrillation; radiofrequency ablation; wolff parkinson white syndrome.
The posteroseptal accessory pathways often are associated with coronary sinus abnormalities. We report the case of a 15-year-old female, who had palpitations due to Wolff Parkinson White Syndrome and high risk posteroseptal accessory pathway associated with coronary sinus diverticulum. The accessory pathway was successfully ablated using radiofrequency catheter ablation into the diverticulum. These accessory pathways have a very short refractory period and are associated with a risk of sudden cardiac death during atrial fibrillation. Performing a coronary sinus venography and demonstrate diverticulum before ablation, substantially reduces failed ablation.
Posteroseptal accessory pathway is mostly associated with coronary sinus diverticulum. It opens by way of the neck either directly into the coronary sinus or into a tributary. The accessory atrioventricular connections associated with venosus diverticulum are epicardial musculature remnants of the sinus venosus. [1]These accessory pathways have very fast conduction properties associated with the high risk of sudden cardiac death. [2] We report the case of a 15-year-old female who suffered from palpitation due to Wolff Parkinson White Syndrome with multiple coronary sinus diverticulum and went to catheter ablation of high risk posteroseptal accessory pathway in one of these diverticulum.
A 15-year-old female with palpitations associated with delta wave on the Surface electrocardiogram consistent with a right side posteroseptal accessory pathway localization (Figure.1).

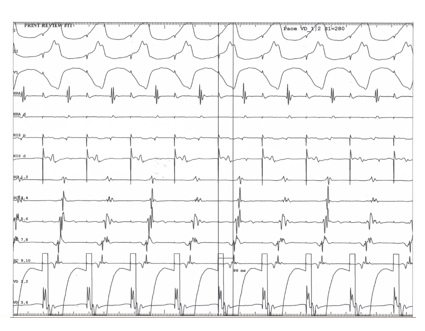
Physical examination and echocardiography disclosed no abnormalities. The treadmill exercise test showed that the maximal heart rate reached 175 bpm, but the delta wave did not disappear. She was referred for an electrophysiological study and radiofrequency catheter ablation under transvenous anesthesia. Three quadripolar catheters were inserted for recording signals from the high right atrium, the right ventricle and the bundle area. Also, a decapolar catether was arranged in the coronary sinus. During ventricular pacing, the earliest atrial activation was at coronary sinus proximal (figure. 2) and decremental property was not shown. Pre-excited atrial fibrillation with high ventricular rate (figure.3) was induced by atrial and ventricular stimulation up to 270 milliseconds unable to reveal the antegrade and retrograde accessory pathway effective refractory period. Mapping was performed on the right side over tricuspid valve and continuous atrioventricular conduction with accessory pathway potential was get into the proximal coronary sinus. Before ablation, a coronary sinus angiography was performed with long steerable sheath (figure. 4) and demonstrated multiple diverticulum coronary sinus into the middle cardiac vein and showed association with atrioventricular fusion and one of these diverticulum (figure. 5). The delta wave disappeared and the accessory pathway conduction was interrupted at 5 seconds after initiation of ablation using an irrigated-tip ablation catheter (therma control, 30 Watts at 42 ˚C up 120 ohm) (figure. 6). After radio frequency application, there was no accessory pathway.




Although most patients with posterior accessory pathway occurs without a coronary sinus diverticulum, the incidence reported in series varying widely. In a series published by Sun et al. 7.5% of patients with posterior accessory pathway retrograde coronary sinus angiography demonstrated a diverticulum. In this largest series, 47% of patients had a previous failed ablation procedure and the accessory pathway was related to the coronary sinus diverticulum in 34/36 patients with diverticulum.3 Also, it has been reported an acute success rate of 75% for ablation procedure into the diverticulum.2 In case of posteroseptal accessory pathway, the abolition of the pathway might be achieve infrequently from the endocardial site of posteroseptal space. In these cases, a coronary sinus contrast angiography which is a safe procedure may be helpful.
Our findings stress the utility for coronary sinus angiography when catheter mapping indicates a localization of posteroseptal accessory pathway. The angiography provides a considerable chance of identifying a coronary sinus diverticulum and increase the success rate of the ablation catheter.
Declare any conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
