
Case Report | DOI: https://doi.org/10.31579/2641-0419/244
1 Central Clinical Hospital of Ministry of Internal and Administration, Warsaw, Poland Woloska 137 Str., 02507 Warsaw, Poland
*Corresponding Author: Katarzyna Byczkowska, Central Clinical Hospital of Ministry of Internal and Administration, Warsaw, Poland Woloska 137 Str., 02507 Warsaw, Poland.
Citation: Katarzyna Byczkowska, Agnieszka Pawlak Robert J. Gil (2022). Post-TAVI Asystole due to Dynamic Gradient in left Ventricular outflow tract - Case Report. J. Clinical Cardiology and Cardiovascular Interventions, 5(3); DOI:10.31579/2641-0419/244
Copyright: © 2022 Katarzyna Byczkowska, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 15 December 2021 | Accepted: 10 January 2022 | Published: 17 January 2022
Keywords: transcatheter aortic valve implantation; intraventricular septal hypertrophy; left ventricular outflow tract obstruction
Left ventricular hypertrophy (LVH) in aortic stenosis (AS) is viewed as a compensatory mechanism aimed at maintaining LV systolic function under chronic pressure overload. In patients with AS, both the presence and the size of the hypertrophy are associated with an increased risk of adverse cardiovascular events, especially when the LV mass is disproportionate to the LV afterload. We presented a case of severe aortic stenosis coexisting with significant intraventricular septal hypertrophy, in which occurred asystole due to dynamic gradient in left ventricular outflow tract immediately after TAVI. Our experience showed that early anticipation of potential LVOTO after TAVI remains a very important issue in clinical cardiology and further research is needed to determine the optimal therapeutic option in such cases.
Transcatheter aortic valve implantation (TAVI) is an effective treatment for severe symptomatic aortic stenosis (AS) in high- and intermediate-risk patients [1,2]. However, in patients with significant ventricular septal hypertrophy, a dynamic increase in the left ventricular outflow tract (LVOT) gradient after TAVI may occur, which may be associated with serious clinical implications [3,4]. The current guidelines do not explain how to proceed in such case. We describe a case of severe aortic stenosis and significant asymmetric left ventricular hypertrophy (LVH), in which appeared asystole during the implantation of the bioprosthesis.
We presented a case of severe aortic stenosis coexisting with significant intraventricular septal hypertrophy, in which occurred asystole due to dynamic gradient in left ventricular outflow tract immediately after TAVI.
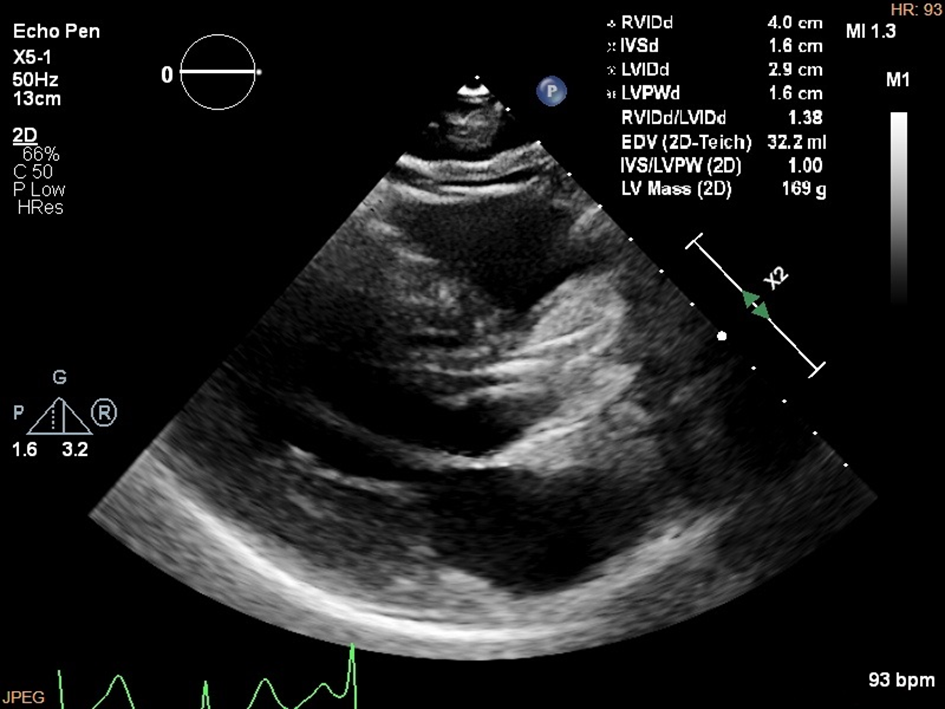
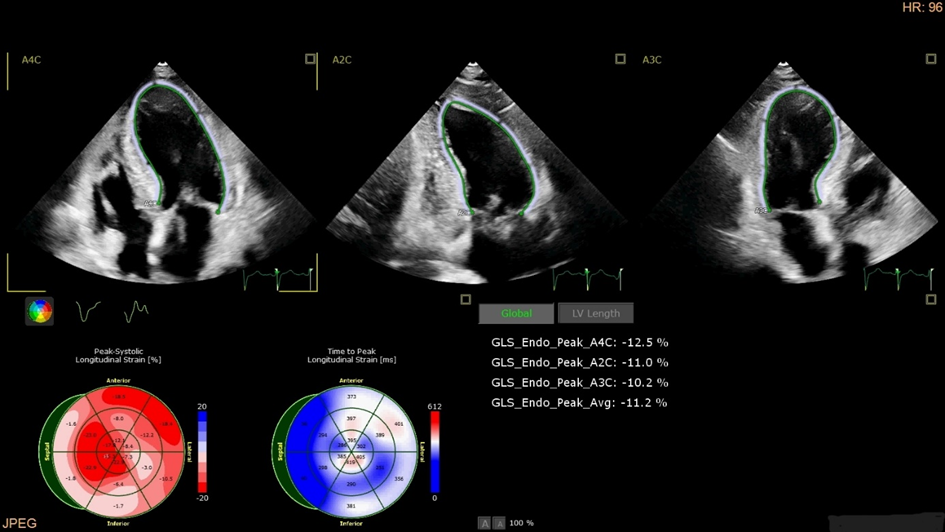
A 79-year-old patient was admitted to the Department of Invasive Cardiology for the diagnosis of chest pain, both stress and rest and occurring at night. Moreover, the patient reported fatigue and exercise dyspnea in NYHA II class. In the clinical history: condition after ischemic stroke, obstruction of the left internal carotid artery, lipid metabolism disorders, hypothyroidism treated with substitution therapy, impaired glucose tolerance, Addison-Biermer anemia. Physical examination didn`t show overt symptoms of heart failure. A regular sinus rhythm of 58 beats was recorded on the ECG, with features of LVH. Echocardiography (TTE) showed severe aortic stenosis, significant hypertrophy of the interventricular septum up to 18 mm in the basal segment with slight acceleration of blood flow along the outflow of the left ventricle, mild systolic motion of the anterior mitral valve leaflet (SAM) and low mitral valve regurgitation. The left ventricular end-diastolic dimension was relatively small at 29 mm (Figure 1). LVEF was estimated to be 60% and LV GLS was decreased to -11,2% (Table 1, Figure 2).
IMPORTANT CHOSEN ECHOCARDIOGRAPHIC PARAMETERS | ||||
Before TAVI | During TAVI | 1-week follow up | 2-months follow-up | |
Ao V max. (m/s) | 4,4 | 2,0 | 2,0 | 1,9 |
Ao grad.max. (mmHg) | 77 | 16 | 16 | 15 |
Ao grad.mean (mmHg) | 42 | 9 | 9 | 9 |
AVA (cm2) | 0.8 | 1.5 | 1.5 | 1.6 |
AVAI (cm2/m2) | 0.44 | 0.82 | 0.82 | 0.88 |
LVOT V max. (m/s) | 2.4 | 7.0 | 3.3 | 2.3 |
LVOT grad.max. (mmHg) | 24 | 195 | 43 | 22 |
LVEDd (mm) | 29 | 35 | 36 | 39 |
LVEF (%) | 60 | 60 | 65 | 65 |
LV GLS (%) | -11,2 | -12 | -13 | -14 |
Mitral regurgitation | Mild | Severe | Mild | Mild |
Ao V max. – maximum aortic velocity, Ao grad.max. – maximum aortic gradient, Ao grad.mean – mean aortic gradient, AVA – aortic valve area, AVAI – aortic valve area index, LVOT V max. – maximum velocity in left venricular outflow tract, LVOT grad.max. – maximum gradient in left venricular outflow tract, LVEDd – left ventricle end-diastolic diameter, LVEF – left venticular ejection fraction, LV GLS – left ventricular global longitudinal strain.
Table 1: Important chosen echocardiographic parameters of the case
There was no significant atherosclerotic changes in the coronary arteries in coronarography. Computed tomography showed aortic stenosis of tricuspid valve (highly calcified leaflets; annulus circumference was 73.7 mm, annulus area was 433 mm 2). Heart-Team decided about TAVI based on patient`s age, intermediate risk of death (STS - 4.24%), and mild Katz frailty syndrome (≥ 5 pts). TAVI was performed via a femoral approach under general anesthesia. After inserting the angiographic guide wire with the system, the St. Jude Portico 27 mm. Asystole developed immediately after implantation, followed by hypotension of 50/30 mmHg. Transesophageal echocardiography (TEE) showed good function of the implanted valve and LVOT obstruction to 5 mm, increased SAM and severe mitral regurgitation. Temporary cardiac stimulation of the right ventricle and continuous intravenous infusion of noradrenaline were used to achieve hemodynamic stabilization (BP 100/60 mmHg, HR 50 / min. in sinus rhythm). The patient was successfully extubated and transferred to the intensive care unit. TTE revealed SAM and LVOTO (v max. 7 m / s, grad. max. 195 mmHg), severe mitral regurgitation, good function of implanted bioprosthesis, LVEF was 60% and LV GLS was decreased -12% (Table 1, Figure 3)

Since a significant gradient in LVOT was still observed, we used IV fluids and bisoprolol at a dose of 2.5 mg. In the control TTE we observed a decrease in the velocity and gradient in LVOT to V max. 3.3 m/s and maximum gradient 43 mmHg and mild mitral regurgitation. Atrioventricular block episodes were not observed in ECG monitoring, therefore the patient was not qualified for pacing system implantation currently. The patient, in good condition, with no cardiovascular complaints, was discharged. During two-months follow-up he remained in good condition and echocardiographic parameters were better. In two months follow-up we took note velocity in LVOT 2.3 m/s, maximum gradient in LVOT 22 mmHg and mild mitral regurgitation (Table 1, Figure 4).

Left ventricular hypertrophy (LVH) in AS is viewed as a compensatory mechanism aimed at maintaining LV systolic function under chronic pressure overload. In patients with AS, both the presence and the size of the hypertrophy are associated with an increased risk of adverse cardiovascular events, especially when the LV mass is disproportionate to the LV afterload [5,6]. Importantly, the negative prognostic effect of excessive concentric LVH in AS was observed regardless of the treatment strategy (pharmacological therapy or interventional treatment) [5].Dynamic intraventricular LV obstruction in severe AS has been reported in approximately 15% of patients undergoing surgical aortic valve replacement (SAVR). Predictive factors were: small LV size, asymmetric IVS hypertrophy, good ejection fraction, and high transvalvular gradients [1,2]. In contrast to hypertrophic cardiomyopathy (HCM), where the greatest gradient is recorded in the LVOT, intraventricular obstruction usually occurs after aortic valve replacement. However, asymmetric IVS hypertrophy, which also occurs in patients with AS, as in our case, may induce significant LVOTO after TAVI. This phenomenon may be due to the interplay of subaortic hypertrophy, the LV ejection fraction, and the alignment of the plane of the mitral valve apparatus [6,7]. The treatment strategy focuses on maintaining the LV filling pressure, slowing the pulse rate to increase diastolic filling time and reduce inotropic activity [8,9].Conservative treatment with beta-blockers often improves haemodynamics, but is not causal. In the event of its ineffectiveness, a ventricular septum may be performed. However, surgical resection may not be feasible for patients undergoing TAVI because of the high risk of death, comorbidities, and the frailty syndrome. Another treatment option is alcohol ablation of the interventricular septum, which is less invasive than surgical resection. However, up to 20% of patients may not have an adequate septal artery, and the procedure requires extensive experience of operators [8]. Dual-chamber stimulation, should also be considered as a therapeutic alternative. And although it is not a causal treatment of LVOTO, cohort studies have shown that right ventricular apex stimulation is effective in reducing the LVOT gradient and reducing symptoms [10,11]. In the presented case, right ventricular stimulation was essential in the treatment of acute haemodynamic instability. And after stabilization of the patient, hydration and treatment with bisoprolol resulted in a reduction of the LVOT gradient. However, it is possible that our patient will soon require the implantation of a dual-chamber pacemaker. Leya et al. reported a case in which severe LVOT obstruction also occurred during TAVI. A second, self-expanding bioprosthesis (valve-in-valve) was then used [12]Clinical vigilance and early anticipation of potential LVOTO after TAVI remains a very important issue. However, further research is needed to determine the optimal therapeutic option in such cases.
We noticed that with significant intraventricular septal hypertrophy a dynamic increase in the left ventricular outflow tract (LVOT) gradient after transcatheter aortic valve implantation (TAVI) may be associated with serious clinical implications, including asystole and cardiogenic shock. The clinical vigilance and early anticipation of potential LVOTO after TAVI remains a very important issue and further research is needed to determine the optimal therapeutic option in such cases.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
