
Research Article | DOI: https://doi.org/10.31579/2641-5194/062
1 Department of Internal medicine, Hepato-gastroenterology, and liver transplantation. Kasr Al-Ainy School of medicine, Cairo University, Cairo, Egypt.
2 Department of general surgery and liver transplantation, Kasr Al-Ainy School of medicine, Cairo University, Cairo, Egypt.
3 Department of Endemic Medicine, Hepato gastroenterology & Liver Transplantation unit, Kasr Al-Ainy School of medicine, Cairo University, Cairo, Egypt.
4 Department of diagnostic and interventional radiology, Kasr Al-Ainy School of medicine, Cairo University, Cairo, Egypt
*Corresponding Author: Abeer Awad Abdellatif. Department of Internal medicine, Hepato-gastroenterology, and liver transplantation. Kasr Al-Ainy School of medicine, Cairo University, Cairo, Egypt.
Citation: Abeer Awad Abdellatif , Doaa A. Mansour, Mohamad Sherif Mogawer, Mostafa El-Shazli, Ayman Salah, et al. (2022). Post living donor liver transplantation recipients in the era of early covid-19. Real-life experience, single-center experience; J. Gastroenterology Pancreatology and Hepatobilary Disorders, 6(3): DOI: 10.31579/2641-5194/062.
Copyright: © 2022 Abeer Awad Abdellatif. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 May 2022 | Accepted: 23 May 2022 | Published: 27 May 2022
Keywords: covid-19; coronavirus; liver transplantation; liver transplant recipient; health care providers; immunosuppression; infection transmission; telemedicine; single center experience; real-life experience.
Background: A novel coronavirus named Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) was first recorded in December 2019 Wuhan, China. Infection rapidly spread worldwide to be declared by the World Health Organization (WHO) as a global Pandemic on March 11, 2020. Owing to the immunosuppressive state of the post-liver transplant recipients, they are considered more susceptible to severe COVID-19. Telemedicine technology is considered low-cost, widely available, and accepted by patients and providers to minimize the risk of spreading the infection to patients or health care providers. The aim of our study is to assess the impact of the recent COVID 19 pandemic on routine practice in the management of liver transplant recipients and the validity of using Telemedicine in the management of post-liver transplant complications. All our post living donor liver transplantation recipients have been screened by phone by the transplant hepatologist team on-call. From March 1st, 2020; we followed our patients through telemedicine and phone calls. Our goal is to reduce clinic visits and provide psychological support to our patients through regular follow up calls.
Results: 36 (6 female, 30 male) out of 159 of our post LDLT was followed by our liver transplant team; with only 12 patients needed hospital service as abdominal ultrasonography, nasopharyngeal swab, computer tomography of the chest, endoscopic retrograde cholangiopancreatography, or percutaneous coronary intervention. Of all our post-transplant patients, three were suspected and four proven to have COVID-19; all of them completely improved. There was no need to modify the dose of immunosuppressive medications. No LDLT surgery was performed during this period. Actually, no case required urgent transplantation.
Conclusion: Telemedicine has been successful in following post-liver transplant patients and minimizing the risk of infection transmission. Improvement in predictive diagnostics and management strategies including the optimal approach to immunosuppression adjustment is still needed.
Background:
In December 2019 Wuhan, China a novel coronavirus named Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) was first recorded and rapidly spread all over the world to be declared by the World Health Organization (WHO) as a global Pandemic on March 11, 2020. [1]
As supposed the disease can be transmitted from human to human through aerosol and droplets resulting in a high probability to acquire the infection [2], it may also be transmitted through feces, and contaminated environmental surfaces. [3] Transmission of infection can also occur from asymptomatic infected persons. [4, 5]
Indeed, immunosuppressive medications have an influence on humoral, cell-mediated immunity, and neutrophil function with the possibility of increasing the risk of severe infections caused by many viral agents, such as adenovirus, rhinovirus, norovirus, influenza, and respiratory syncytial virus. [6]
Because of the long-term immunosuppressive drugs that post-liver transplant recipient is exposed to, they may be more susceptible to severe COVID-19 infection with a worse prognosis when compared with the general population, so post-liver transplant recipients should be managed cautiously. Follow-up and methods of communication with health care providers should be adjusted to limit the risk of infection transmission during the COVID-19 pandemic. [7]
Organ transplant recipients are considered susceptible population to COVID-19 infection so whether to defer transplantation or not during this pandemic is still debatable [8], as many centers suggested that transplantation should be deferred while others recommend performing transplantation under strict infection precautions and after careful risk assessments.Moreover, the decision should rely upon certain considerations as center capability regarding the availability of intensive care beds, ventilators, and available donated blood. [9]
Currently, Egyptian patients have a high prevalence of chronic liver diseases with increasing numbers of patients suffering from end-stage liver disease (ESLD) that necessitating liver transplantation (LT). [10] In Egypt only living donor liver transplantation (LDLT) programs are available now. [10]
COVID-19 infection may present with a wide variety of symptoms ranging from mild to severe symptoms as fever, dry cough, dyspnea, fatigue, anorexia, nausea, nasal congestion, sore throat, myalgia, diarrhea or complications as severe pneumonia or acute respiratory distress syndrome (ARDS). Owing to the long-term use of immunosuppressive drugs in post-liver transplant recipients, COVID-19 infection may progress rapidly to acute ARDS. [4]
Because of the immunosuppressed state of the post-liver transplant recipients; it is advised to test for COVID-19 in any post-liver transplant patient complaining of fever with a consideration that negative results do not exclude the infection and even normal computed tomography (CT) of the chest does not exclude COVID-19 infection. [11]
50% of COVID-19 infected patients developed liver dysfunction; AST and ALT are primarily elevated with normal to moderately elevated total bilirubin levels but it is usually transient and resolves within 2–3 weeks; however, before considering COVID-19 infection as a cause of elevated liver enzymes, other etiologies must be excluded as cytomegalovirus (CMV). [4, 12]
Liver injury may be common in severe COVID-19 rather than mild cases. Elevated liver biochemistries could be explained by a direct virus-induced cytopathic effect and/or immune damage from the provoked inflammatory response (cytokine storm) that occurs with COVID-19 infection. [13, 14]
In this context and especially in post-liver transplant patients, it will be very difficult to differentiate whether increases in liver biochemistries are due to SARS-CoV-2 infection itself; its complications, including myositis (particularly with AST>ALT), cytokine release syndrome, ischemia/hypotension; or due to post-liver transplantation complications as rejection or drug-induced liver injury. [15, 16]
During COVID-19 pandemic; frequency of examination, blood tests, or imaging to the post-liver transplant recipients should be minimized as much as possible to diminish exposure of patients and health care workers. Telemedicine through using online clinics and phone calls are the preferred methods of communication between the patient and health care providers to avoid cross-infection during hospital visits. [17] Together with restriction of hospital admission of liver transplant recipients to those suffering from major complications such as rejection, decompensation, vascular or biliary complications. [18] Also, with limiting the transport of patients for ultrasound or other advanced imaging (e.g., MRI/MRCP) unless it is highly indicated e.g., clinical suspicion for biliary obstruction or venous thrombosis. We think it is mandatory to develop an internet-based educational, dietitian, and financial consultation sessions for patients and family members.
The exact effects of immunosuppression on COVID-19 are not well established; Immunosuppression may prolong viral shedding in post-transplant patients with COVID-19 [19, 20]; Therefore, the immunosuppressed patients are considered to be at higher risk for severe illness from COVID-19 infection, but it is not well documented if post-transplant patients are at greater risk for more severe COVID-19 infection than the general population. [21]
As it is reported for SARS (2002-2003) and MERS (2012-present); the post-transplant immunosuppression was not found to be a risk factor for mortality, meanwhile it is not well known till now if COVID-19 infection in post-transplant patients is associated with a higher risk of mortality. [22]
The telephone is the most valuable method of communication with the patients both inside and outside the hospital during any pandemics. Collection of functional signs, interrogation of the patient, and questions and explanations of the clinical situation, as well as the provision of information for the patient, are all undertaken by phone. This aims to limit the virus spreading and to decrease the contact between the patients and the medical staff in order to limit the risk of the infection spreading. [23]
A method of using a tele-triage service is found to be a good way to triage the patient before contact visit to the hospital of the outpatient clinic, this practice should verify as best it can that the patient does not have symptoms of COVID-19. Visits that may be conducted via telemedicine should be encouraged. For visits that must take place in person, administrative staff should contact the patient via phone within 24 hours prior to the office visit to select the best way to offer the medical service without any hazards that could be conducted to other patients or health care providers. [24]
There is still limited data about dealing with post-liver transplant recipient during COVID-19 pandemic regarding modification of immunosuppressive therapy, the efficiency of new methods of communication with health care providers to limit hospital visits for decreasing the risk of exposure, and so here we will demonstrate our experience as a single center in dealing and managing our post-liver transplant recipient as regarding immunosuppressive therapy, problems facing our patients, drug-drug interactions and value of using telemedicine to prevent rejection and effectively treat the underlying health-related problems during the COVID-19 pandemic.
To assess the impact of recent COVID 19 pandemics on routine practice in the management of liver transplant recipients in the transplantation unit of El-Manial Specialized Hospital, Cairo University and the validity of using Telemedicine in the management of post-liver transplant complications.
Methods:
Patients:
In our transplantation unit of El-Manial Specialized Hospital, Cairo University; all our post LDLT recipients have been screened by phone by the transplant hepatologist on-call team about travel history with fever or respiratory symptoms, but we have not tested for COVID-19 PCR except in those who gave history or symptoms suggestive of COVID-19 infection.
From March 1st, 2020 till 31th May; we closed our post-transplant clinic and we followed our patients through telemedicine and phone calls at a frequency of once every two weeks, actually, the frequency of care differ from one patient to the other according to the clinical status, comorbidities, and presence of post-transplant complications. Our goal was to reduce clinic visits to the maximum and provide psychological support to our patients through regular follow up calls.
We emphasize our post-transplant patients about preventive measures that should be followed such as frequent hand washing, cleaning frequently touched surfaces, staying away from large crowds, staying away from individuals who are ill and not to travel during this pandemic.
Transplant coordinators will call patients at home and document their clinical status, BP, heart rate, and weight; this will be followed by the transplant team via telephone to review the laboratory tests to assess overall management, medications, and any newly reported complaints.
Our routine postoperative follow-up schedule labs included liver profile (ALT, AST, serum bilirubin, serum albumin), coagulation profile and trough level of the immunosuppressive drug; also any added labs according to the patient’s complaint.
Statistical analysis:
Data management and analysis were performed using Statistical Package for Social Sciences (SPSS) vs. 25. Numerical data were summarized using means and standard deviations or medians and/or ranges, as appropriate. Categorical data were summarized as numbers and percentages. Estimates of the frequency were done using the numbers and percentages.
During March, April, and May; 36 (6 female, 30 male) out of 159 of our post LDLT were followed by our liver transplant team; others were missed follow up either due to technical difficulty or traveling history. All our patients were having liver transplanted from their related donors. The demographic data of the patient involved demonstrated in table 1
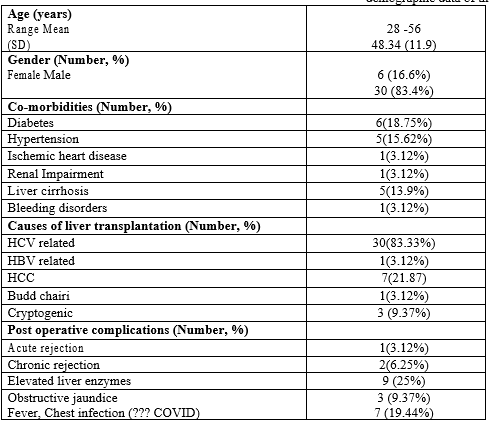
Table (1): Demographic data of the patients and presentation (total=36)
16 patients showed normal follow up parameters, 2 patients asked about the possibility of fasting during Ramadan (Ramadan is a Holly month during which Moslems fast for a period of about 15 hours/day), one patient complained from uncontrolled DM and elevated tacrolimus trough level, one of our patients developed ischemic chest pain necessitating percutaneous coronary intervention (PCI), one case of Budd Chiari needed to communicate for adjusting his anticoagulation dose, one patient was followed for intraabdominal collection and 9 patients had elevated liver function tests.
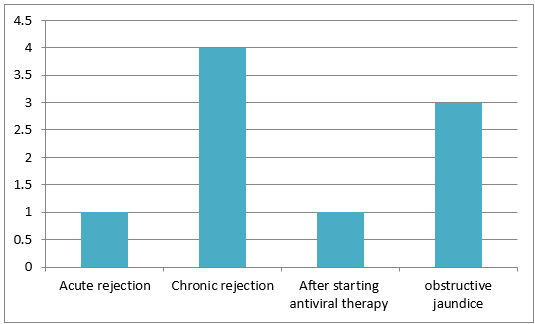
From the 9 patients who had elevated liver enzymes, one was due to acute rejection, 4 were due to chronic rejection, one was due to cholestasis which has started after antiviral therapy and three patients were due to obstructive jaundice as demonstrated in (figure 1).
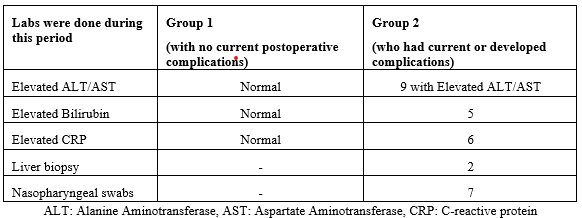
The labs that were required during this period showed in table 2.
From the three patients with obstructive jaundice, ERCP was performed in two patients while the third was postponed due to non-urgency.
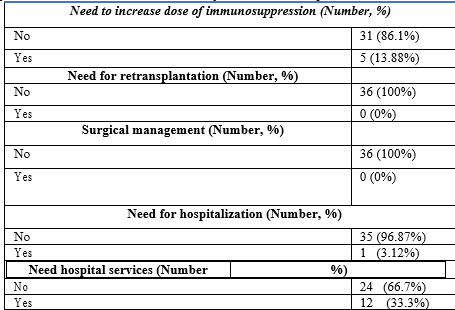
We needed to increase the dose of immunosuppressive therapy for five patients due to chronic rejection and needed to decrease the dose of immunosuppressive therapy in one patient due to elevated FK trough level.
During the identified period of follow up, 12 of our patients needed hospital service; two needed abdominal ultra-sonographies, seven had to perform CT chest and nasopharyngeal swabs, two needed urgent ERCP, and one needed percutaneous coronary angiography.
We had three patients suspected of COVID-19 infection. The first patient was a 55 years old male patient who underwent living donor liver transplantation for liver cirrhosis due to chronic hepatitis C infection which was diagnosed in 2017, the patient was not diabetic or hypertensive, the patient’s maintenance immunosuppressive medication was everolimus 0.75mg orally twice daily and cyclosporine 75 mg orally twice daily. His complaint was a cough with yellowish expectoration, dyspnea, and high-grade fever of three days duration which aroused our suspicion toward the possibility of COVID-19 infection. A nasopharyngeal swab for SARS-COV2 was done by RT-PCR and was negative. CT chest and CBC were normal and all his symptoms completely resolved with IV antibiotics after 2 days duration. The patient’s immunosuppressive therapy was continued as previously adjusted.
The second case was a 56 years old male who underwent living donor liver transplantation for HCC (within Milan criteria) on top of hepatitis C infection in 2017, complicated by recurrence of HCC with metastatic pulmonary nodules 2 years after transplantation. He is not diabetic or hypertensive. His current immunosuppressive medication was tacrolimus 2mg orally twice daily and everolimus 0.75mg orally twice daily. His complaint was a dry cough, dyspnea without fever, chills, or gastrointestinal symptoms. A Nasopharyngeal swab for SARS-COV2 was done by RT-PCR and was negative. CT chest and CBC were normal. Symptomatic treatment was prescribed for follow up with the oncology department.
The last patient was 32 years old male who underwent living donor liver transplantation for cryptogenic cirrhosis in 2019, he was not diabetic or hypertensive, his maintenance immunosuppressive medication was tacrolimus 2mg orally twice daily and everolimus 0.75mg orally twice daily. He complained of fever with cough and greenish sputum for 2 days duration, CBC, CRP, Chest-Xray were normal with complete disappearance of fever after starting IV antibiotics. Negative nasopharyngeal swab for SARS-COV2 by RT-PCR. No one of our suspected COVID patients had decreased the dose of immunosuppression. Hospitalization was not needed in any of our patients suspected to have COVID-19.
Four patients discovered to have COVID infection; all were undergone living donor liver transplantation for HCV related cirrhosis in 2014, 2018, 2019, and 2020 respectively; none of them were diabetic or hypertensive. There maintenance immunosuppressive medication was tacrolimus. They developed symptoms suggestive of COVID infection as fever, dyspnea, and dry cough. Nasopharyngeal swabs were positive, all were having mild infection for which home isolation and supportive treatment were only sufficient. Modification in the dose of immunosuppressive medications was not required.
No living donor liver transplant surgery was performed during the COVID-19 pandemic because we have been concerned about the risk of infection transmission to patient and medical staff, also to restore the resources and ICU beds during this pandemic. Actually, no case for urgent transplantation was needed during this period. Ways of management needed to our patients demonstrated in table 3.
We now hope that the work of transplantation can recover gradually without the risk of infection transmission in all donors, patients, and our medical staff following the passage of the pandemic situation.
Recently our transplantation team has been discussing a gradual return to our active program with major modifications in order to avoid the risk of COVID-19 infection among patients, donors, and the medical staff. We are still facing a shortage of ICU beds which will probably be the most important factor affecting the number of cases selected for liver transplantation
Emerging infectious diseases is a nightmare facing organ transplantation. Indeed, the emergence of a novel SARS-CoV-2 has a great impact on organ transplantation worldwide. The impact has not been just for restriction issues related to donors or recipients, but also for the availability of health-care resource utilization as the intensity of cases in certain jurisdictions exceeds available capacity. [25] With the emerging SARS-CoV-2 pandemic, solid organ post-transplant patients remain highly vulnerable to severe infection, morbidity, and mortality. [26]
Unlike infections with other similar viruses such as severe acute respiratory syndrome coronavirus (SARS-CoV) and Middle East respiratory syndrome coronavirus (MERS-CoV) that was reported in transplant recipients during prior outbreaks of these viruses; There are a few available data about COVID-19 infection in organ transplant recipients or donors. [27]
Most organ transplantation centers worldwide have been postponed all elective organ transplantation. On March 9, 2020, France, Strasbourg stopped all living donors and deceased kidney transplantation, also most of the outpatient clinics dealing with PR transplantation or post-transplantation are managed through video or teleconference. Living donor kidney transplant procedures are mostly being postponed throughout Germany. In Spain only emergency life-saving transplant procedures continue, after excluding COVID-19 in both the donor and recipient with cancellation to all non-emergency appointments. Hong Kong established a 50% reduction in elective LDLT in order to minimize the utilization of medical resources, ICU beds, isolation wards, and the availability of healthcare providers for fighting the infection. [28]
Many transplant centers worldwide developed COVID-19 donor and recipient clinical screening programs such as Canada, Switzerland, Italy, and Spain. Accordingly, the Japanese Society for Transplantation (JST) established a recommendation to screen donors for significant exposure to COVID-19, travel history to high-risk countries, and symptoms including fever and respiratory symptoms together with home or hospital isolation for 14 days prior to intervention in order to avoid COVID-19 exposure for both lung and liver living donors, in cases where transplantation can be postponed for 14 days. Also; the Korean Society for Transplantation (KST) published their recommendation on March 13, 2020, for testing both living and deceased donors for SARS-CoV-2 NAT by a nasopharyngeal swab prior to appointment. However, there is still variation in approach to donation between different countries according to the burden of COVID-19 infection and availability of service resources. [25]
In Lombardy, Italy, and between 5 and 18 March; three deaths out of 111 long-term liver transplant survivors had been reported due to severe COVID-19 disease. All three COVID-19-related deaths were long-term transplanted patients on minimal immunosuppressive regimens. [23]
In our liver transplantation center, we stopped all outpatient clinics during March and April till now and deferred all non-urgent liver transplantation lists; fortunately, we are not faced with cases needing urgent liver transplantation.
During this period all our post-transplant patients were followed through telemedicine by our transplant hepatologists on-call team. We could successfully manage most medical problems through telemedicine; with only 12 patients needed hospital service including abdominal US, CT chest, nasopharyngeal swabs, ERCP, or PCI. From our entire post-transplant patients, three were suspected and four were proven to have COVID-19 infection with symptoms of fever, cough, and dyspnea; all of them completely improved with no mortality. We had no need for a decrease or modification in the dose of immunosuppressive medications.
Currently, the number of COVID-19 confirmed cases after liver transplantation is limited. In general, the clinical manifestations of COVID-19 in post-transplant patients were found to be similar to the general population. [29]
Since the day of Wuhan’s closure in China on January 23; 22 cases of COVID-19 infection were confirmed to be in organ transplant recipients. There were 19 kidneys and 3 liver transplant patients. As supposed that the transplant patients have a higher threshold of self-protection and usually appreciation the self-protection instructions against infection with SARS-COV-2. All patients were given strict clear instructions of using social distancing, facial masks, hand washing, and self-isolating measures. [28] Bergamo reported also three of two hundred transplant recipients with confirmed COVID-19 infection. [22]
In literature, a unique case report of COVID-19 infection has been reported in a 55-month-old girl, who acquired infection 5 months after undergoing liver transplantation, fortunately, she recovered completely despite the high level of immunosuppression. [30] Another case report on unanticipated LDLT records liver donation from a COVID-19–infected donor, the donor was apparently healthy with mild symptoms; lopinavir plus ritonavir was started on the recipient then shifted to hydroxychloroquine due to drug-drug interaction. Fortunately, the result of the serial COVID-19 rRT-PCR test via both nasopharyngeal swab and serum were negative. Further information on the pathogenesis and transmissibility of COVID-19 in organ transplantation is still required. [31]
The impact of immunosuppression in the post-transplant setting is currently not known and further data is needed before any specific recommendation can be made. It is expected that due to immunosuppression post-transplant, infected patients may have more intense and prolonged shedding of the virus. This will also increase the risk of viral transmission among healthcare workers. Antivirals for COVID-19 will be available in the very near future, and drug-drug interactions with immunosuppressive medications will also need to be considered.
Telemedicine technology is considered low-cost, widely available, and accepted by patients and providers which provide care to patients without compromising clinical care. The emerging COVID pandemic enables us with a chance to leverage this technology not just in times of crisis, but also to provide improvement in access, safety, and efficiency for primary and specialty care. [32]
Actually, we faced some difficulties with our patients while using telemedicine due to inaccessibility and low social and cultural levels; this may explain the limited number of patients that can actually communicate with us so it is very important especially in low developed countries to find another way for following up and communicating with patients during the pandemic such as home visits or getting outpatient clinics in a safe place away from hospital settings.
In this context during the COVID-19 pandemic, telemedicine has been successful for follow up of post-liver transplant patients resulting in minimizing the risk of infection transmission particularly in integrated systems of care. The pandemic has highlighted the utmost importance of working as a team and to share knowledge and experience for the benefit of patients. Indeed, many kinds of research for COVID infection whether regarding outcomes, predictive diagnostics, and management strategies including the optimal approach to immunosuppression adjustment in organ transplantation is largely needed.
Recommendations:
Abbreviation:
SARS-CoV-2: Severe Acute Respiratory Syndrome Coronavirus-2.
WHO: World Health Organization?
LDLT: Living donor liver transplantation.
ESLD: End-stage liver disease.
ARDS: Acute respiratory distress syndrome.
CT: Computed tomography.
CMV: Cytomegalovirus.
ERCP: Endoscopic retrograde cholangiopancreatography.
PCI: Percutaneous coronary intervention.
JST: Japanese Society for Transplantation.
Declarations:
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
