
Short Communication | DOI: https://doi.org/10.31579/2642-9756/087
1 Assistant Professor, Lady Hardinge Medical College, New Delhi, India.
*Corresponding Author: Kanika Chopra, Assistant Professor, Lady Hardinge Medical College, New Delhi, India
Citation: Barkha Vats, Sukriti Ghai, Reena Yadav, Kanika Chopra (2021). Placenta Accreta Syndrome- A Calamitous Diagnosisy. J. Women Health Care and Issues. 4(7); DOI:10.31579/2642-9756/087
Copyright: © 2021 Kanika Chopra, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 November 2021 | Accepted: 02 December 2021 | Published: 08 December 2021
Keywords: placenta accreta syndrome; hysterectomy; pelvic devascularization; conservative approach
Increasing incidence of Placenta accrete syndrome has become a worrisome issue due to its associated life-threatening complications for both the mother and the fetus. The ideal management for PAS disorder remains the matter of debate still. The critical step in its effective management being its suspicion knowing the underlying risk factors and its diagnosis in antenatal period. Still, cesarean hysterectomy remains the gold standard procedure with many newer conservative approaches under evaluation. Our basic aim behind writing this review is to highlight the recent changes in classifying and diagnosing PAS owing to the ever-increasing incidence of this catastrophic entity. Also, it will emphasize the well-established role of radical over conservative management and also all modalities used in conservative management so far.
Placenta accreta syndrome previously known as morbidly adherent placenta is a significantly grave obstetrical condition. PAS includes both abnormally adherent placenta where implantation of villi are in direct contact with myometrium without obvious plane of separation and abnormally invasive placenta where villi invade into the myometrium and even nearby organs. FIGO define PAS as grade 1, 2 and 3 [1]. It can be considered as a multifactorial pathology and results due to factors like defective decidua, abnormality in trophoblastic invasion, abnormal angiogenesis and thus neovascularization [2]. There has been a tremendous increase in the incidence of PAS in last three to four decades. The cited incidence of placenta accreta was 1 in 2510 in the 1980 which has risen to 1 to 533 in recent years. [3] The root cause of this rising incidence being increase in cesarean section rate. It accounts for considerable maternal mortality and morbidity and thus represent a major challenge to the obstetricians. So, it is prudent that having knowledge of risk factors, a high clinical suspicion is made, so that antenatal radiological diagnosis is made and patient managed in equipped facility. The standard treatment in majority of the cases of PAS is peripartum hysterectomy including our hospital, the exclusion being a case of focal accreta. Recently there was increasing inclination towards conservative approach, but radical treatment remains the best. Our basic aim behind writing this review is to highlight the recent changes in classifying and diagnosing PAS owing to the ever-increasing incidence of this catastrophic entity. Also, it will emphasize the well-established role of radical over conservative management and also all modalities used in conservative management so far.
Ultrasound is the first line diagnostic modality, but the signs seen and the terminology used happen to have variable heterogeneity. Moreover, diagnosis depends on the operator’s experience. 3-D power doppler use is under investigation and may prove to improve antenatal diagnosis. MRI do have a role in cases like posterior placenta, ultrasound suggestive of parametrium invasion of placenta and in patients with high BMI. This imaging modality has a high sensitivity and specificity with disadvantage of being not available readily and being expensive.
Management in a case of PAS is cesarean hysterectomy with the placenta in situ as the gold standard procedure as seen in figure 1, except in few cases of focally adherent placenta.
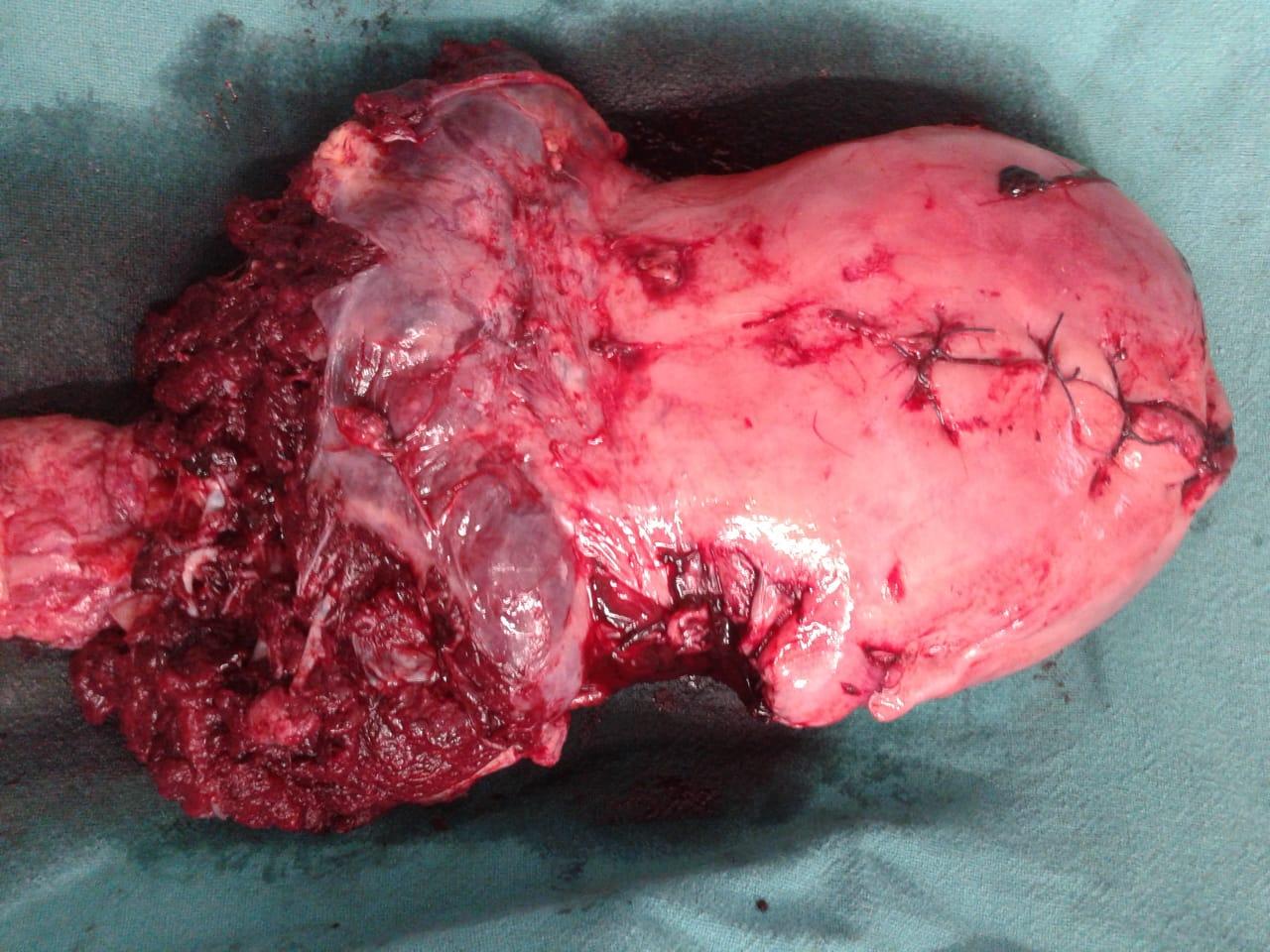
IS-AIP defines focal adherence as < 50>
Cases antenatally diagnosed should be referred or managed in a tertiary care center with a dedicated multidisciplinary team for optimum management of PAS. This team should include experienced obstetrician, pelvic surgeons, general surgeons, urologists, interventional radiologist, anesthesiologist, blood bank officer and strong nursing leadership. Delivery is planned at 35+0 to 36+6 if the risk factors for preterm delivery like preeclampsia, preterm rupture of membranes are not present. [6]
Alternative to conventional hysterectomy especially if there is bladder involvement is retrograde hysterectomy. In this approach retroperitoneal space is developed followed by internal iliac ligation. The vaginal vault is then opened posteriorly and a plane is developed through lateral dissection to separate the bladder. The blood loss in this procedure is lesser as compared to conventional hysterectomy. [7]
Delayed hysterectomy is another alternative. It is found to be beneficial because of prevention of complications during immediate hysterectomy like decrease risk of hemorrhage and need for massive blood transfusion. In a large case series in which 13 women with placenta percreta underwent delayed hysterectomy after a median 41 days of elective cesarean section. It was observed that blood loss was markedly less as compared to cesarean hysterectomy. [8]
Endovascular intervention like balloon catheter, arterial embolization or combination of these two have been found to decrease blood loss in some case reports but are not recommended.9,10 But these procedures have been found to be ineffective as seen in our hospital as well. The main reason behind this lies in the pathophysiology of development of PAS i.e., neovascularization and development of collaterals. There can be vessel injury, ischemia and thromboembolism related to these procedures.
Multitudinous other approaches have been defined in terms of number of case reports, series and retrospective studies highlighting the benefits of conservative approach, but none have been proved of much significance. The indications of conservative methods are also limited and includes:
The most important inception for conservative approach being no excessive bleeding following delivery of baby and patient hemodynamically stable with no coagulopathy. Informed consents prior to proceeding with it includes high risk of bleeding, infection, coagulopathy, uterine necrosis, need for hysterectomy in emergency, need for long term follow-up and risk of PAS in future pregnancies as well. Studies have shown that 31.4
It is one of the most dreaded complication as there is increased risk of post-partum hemorrhage, massive blood transfusion, peripartum hysterectomy, surgical injuries, ICU stay, sepsis, deep venous thrombosis, transfusion related lung injury, disseminated intravascular coagulation and even maternal death. Keeping all these factors in mind, measures should be taken to reduce the incidence of PAS and to diagnose it prenatally. Prevention strategies may include avoiding caesarean section birth, correct surgical techniques while closing the uterine incision, avoiding vigorous curettage, and treatment of postpartum endometritis. The most important contributor to the increased incidence is the rising cesarean section births. We know that cesarean section has revolutionized the fetal and maternity care but it must be performed only when indicated and should not be used as a surgery of convenience. Efforts should be made to promote vaginal delivery and reduce the cesarean rates.
None
None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
