
Case Report | DOI: https://doi.org/10.31579/2640-1045/107
Department of Endocrinology, Aga Khan University, Stadium Road, Karachi, Pakistan.
*Corresponding Author: Sajjad Ali Khan, Department of Endocrinology, Aga Khan University, Stadium Road, Karachi, Pakistan.
Citation: N Ram, Sajjad A Khan, D Ali, M Saleem. (2021) Pituitary Macroadenoma: A Rare Presentation of Hypothyroidism. Endocrinology and Disorders. 5(8): DOI:10.31579/2640-1045/107
Copyright: © 2021 Sajjad Ali Khan, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 21 October 2021 | Accepted: 08 November 2021 | Published: 12 November 2021
Keywords: hypothyroidism; pituitary macroadenoma; hyperprolactinemia; rare presentation; thyroid replacement therapy; MRI lesion
Hypothyroidism is a common endocrine disease which occurs when the levels of Thyroid hormones produced by the Thyroid gland are decreased.
Here we present a case of a 19-year-old female, who presented with symptoms of hyperprolactinemia, weight gain, unilateral blurring of eyes and headache. Examination findings of the patient were significant for presence of Acanthosis Nigricans and Hirsutism. Rest of the systemic examination was normal. Laboratory investigations revealed Hyperprolactinemia, Hypothyroid profile and dyslipidemia. MRI brain and pituitary done showed findings consistent with Pituitary macroadenoma. Patient was treated along the lines of hypothyroidism with Thyroxine. Follow-up after 3 months showed improvement of her symptoms and disappearance of lesion of MRI scan.
This case was a rare presentation of Hypothyroidism. Such unusual and uncommon presentations should be reported and studied in detail to prevent misdiagnosis and provide the correct treatment to the patients.
Hypothyroidism is a common endocrine disorder in which there is deficiency of Thyroid hormones. Common clinical presentations may vary in different age groups, different sexes, and according to the time period between the disease onset and diagnosis. Commonly occurring symptoms include tiredness, lethargy, intolerance to cold, weight gain, constipation, voice changes, and skin dryness [1].
One third of individuals suffering from primary hypothyroidism have increased levels of prolactin [2]. These individuals may present with symptoms of hyperprolactinemia such as menstrual irregularities, galactorrhea, low bone mass, decreased libido, impotence, infertility, erectile dysfunction [3].
Differentiating between pituitary adenoma and hyperplasia using imaging techniques still is difficult despite of advancements in imagining modalities [4].
Long standing cases of Primary Hypothyroidism may lead to pituitary hyperplasia. Lack of circulating levels of Thyroxine (T4) and Triiodothyronine(T3) leads to loss of negative feedback loop which in turn causes the release of large amounts of Thyrotrophin releasing hormone (TRH) from the Hypothalamus [5].
Hypothyroid patients in which these adenomas have occurred have shown regression after correction of hypothyroidism by Thyroxine supplementation. Therefore, hypothyroidism should always be considered as a differential in patients presenting with pituitary adenomas, and if a clinician is able to identify the cause of the lesion as hypothyroidism then medical treatment should be given rather than opting for surgical treatment options [6].
Here we present a case of a 19-year-old girl who presented with clinical features consistent with pituitary macroadenoma, however, after workup she was diagnosed with hypothyroidism. Her symptoms and lesions resolved after Thyroid replacement therapy.
This a rare presentation of Hypothyroidism and necessitates discussion so physicians may be able to identity such presentations of Hypothyroidism and avoid unnecessary surgical procedures.
This case report was reviewed and approved by the Ethics Review Committee of The Aga Khan University.
19-year-old female, weighing 100 kgs, known case of Poly Cystic Ovary Syndrome (on Oral Contraceptive Pills) presented to the endocrinology clinic with complaints of
Oligomenorrhea – for the past 1 month
Galactorrhea – for the past 1 month
Occasional blurring of eyes (right sided) since the past
Weight gain
Headache- past 1 month
On presentation, patient’s vitals were Temp 36.2, BP 120/79, Pulse 79/75 bpm. R/R 18/min. Examination findings included Acanthosis Nigricans ++ and Hirsutism +. Rest of the systemic examination was normal. Lab investigations revealed Hyperprolactinemia (Prolactin level of 39) and dyslipidemia (cholesterol 310, LDL, 221, HDL 45, TG 303).
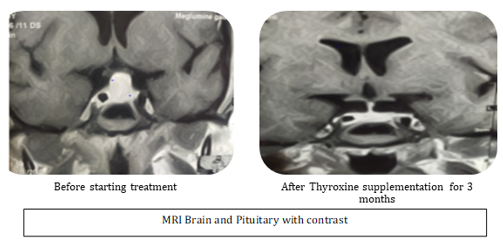
MRI Brain with pituitary and contrast was done which showed Pituitary Macroadenoma measuring 18 x 16 x 11.7 mm with lateral extension into the cavernous sinus on either side. The mass is abutting bilateral ICA. Superiorly mass is abutting the Optic Chiasm and Inferiorly bulging into the sphenoid sinus. Further workup of the patient was done which showed findings consistent with Hypothyroidism (TSH >150, FT4<0>
Patient was started on tablet Thyroxine 150mg/day and advised to lose weight and follow-up with the consultant after 3 months on Thyroxine supplementation.
3 months after the initial visit, patient presented with:
Improvement in Headaches
Irregular menstrual cycle
Weight loss of 10 kgs (100 to 90kgs)
On presentation, patient’s vitals were Temperature 36.2, BP 120/69, Pulse 105, R/R 20. TSH done was 0.030. MRI brain and pituitary showed disappearance of the abnormal signal intensity pituitary gland which was previously seen.
One third of individuals suffering from primary hypothyroidism have increased levels of prolactin [2]. Our patient presented with high prolactin levels of 39.
Increase in size of the pituitary gland may be seen in cases of hypothyroidism. This is a caused by reactive hyperplasia and is related to the level of TSH increase. This kind of a clinical picture is suggestive of long-standing hypothyroidism and severe symptoms; however, this is not always true. Individuals may present with no symptoms or symptoms consistent with other endocrine diseases.
Precocious puberty may be seen in children while adults may present with symptoms of amenorrhea or decreased libido.
Thyroid function tests should always be tested whenever a patient presents with symptoms pointing towards presence of a pituitary tumor [7]. Our patient presented with menstrual irregularities, galactorrhea, weight gain and pressure symptoms of headache and unilateral blurring of vision. These symptoms are consistent with the features of pituitary macroadenoma. Our patient underwent workup for thyroid disease and showed labs consistent with hypothyroidism i.e., TSH >150, FT4<0>
Increase in Thyrotrophic cells is a phenomenon seen is protracted case of Hypothyroidism and may present with features consistent with pituitary macroadenoma [8]. The mechanism which causes increase In numbers of Thyrotrophic cells is through the negative feedback loop; decrease in levels of circulating thyroid hormones causes the thyrotrophin releasing hormones (TRH) to overstimulate the thyrotrophs [8].
It is difficult to differentiate between TSH-producing macroadenoma and hyperplasia of pituitary thyrotroph cells on radiological modalities like the CT and MRI. However, in case of pituitary hyperplasia, the lesion would not appear in follow-up repeat MRIs after thyroxine supplementation. This is a way to establish a definitive diagnosis and avoid the need for needless surgical procedures [9]. Initial presentation of our patient showed a lesion on MRI measuring 18 x 16 x 11.7 mm. Patient was started on Thyroid replacement therapy and MRI repeated after 3 months. The lesion disappeared on repeat MRI, suggesting a diagnosis of pituitary hyperplasia.
Study done in National Center for Diabetes, Endocrinology and Genetics in Amman, Jordon showed a decreased in size of the pituitary gland of 85% individuals on follow-up MRI after Thyroxine treatment [10].
Thyrotoph hyperplasia has been described in the background of primary hypothyroidism. Most cases present with elevated levels of TSH which can in cause increase in size of pituitary gland. The treatment for such a case is by giving Thyroxine supplementation, however, it should not be done in cases of any visual field deficit [11]. Our patient had minor visual deficits, with only occasional blurring of her right eye so surgery was not considered.
Surgery should only be done in cases where a decompression of optic chiasm is required. Additionally, if a pathological diagnosis is needed for a mass which is not responsive to or deteriorates after thyroid replacement therapy [9].
MRI- Magnetic resonance imaging
This case was a rare presentation of Hypothyroidism. Such unusual and uncommon presentations should be reported and studied in detail to prevent misdiagnosis and provide the correct treatment to the patients.
Financial and other conflicts of interest: None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
