
Research Article | DOI: https://doi.org/10.31579/2639-4162/145
1Graduate in Health Technology, Physical Therapy and Rehabilitation profile. Assistant Professor. Associate Researcher. Department of Postgraduate and Research, Faculties of Medical Sciences, Sancti Spiritus. E
2Dra. Medicine. Specialist in First Degree in Comprehensive General Medicine and in normal and pathological Physiology. Instructor Professor. Department of Basic Biomedical Sciences, Faculties of Medical Sciences, Sancti Spiritus.
3Dra. Medicine. Specialist in First Degree in Comprehensive General Medicine and in normal and pathological Physiology. Instructor Professor. Department of Basic Biomedical Sciences, Faculties of Medical Sciences, Sancti Spiritus.
4Dra. Medicine. Specialist in First Degree in Comprehensive General Medicine and in normal and pathological Physiology. Instructor Professor. Department of Basic Biomedical Sciences, Faculties of Medical Sciences, Sancti Spiritus.
5Dr. Veterinary medicine. MSc. Preventive Veterinary Medicine. Assistant Professor Departamento Medios Diagnósticos, Faculty of Medical Sciences, Sancti Spiritus.
*Corresponding Author: Adrian González Méndez, Universidad de Ciencias Médicas, Departamento de Postgrado e Investigaciones, Sancti Spiritus, Cuba.
Citation: Adrian G. Méndez, López Cruz AI, Sandra R. Hernández, Lorelys M. González, Díaz Rodríguez NE, et al, (2024), Physiological Variables in Cardiovascular Rehabilitation with Resistance Training in Patients with Ischemic Heart Disease, J. General Medicine and Clinical Practice, 7(4); DOI:10.31579/2639-4162/145
Copyright: © 2024, Adrian González Méndez. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 January 2024 | Accepted: 11 March 2024 | Published: 17 March 2024
Keywords: cardiovascular rehabilitation programs; ischemic heart disease; hyperinsulinism
Introduction: Resistance training recognized as an essential component in cardiac rehabilitation programs.
Objective: to evaluate the behavior of physiological variables after the application of resistance training complementary to aerobic training in patients diagnosed with ischemic heart disease. Method: A quasi-experimental before-after study without a control group was carried out with the objective of evaluating the behavior of the physiological variables after the application of cardiovascular rehabilitation with supervised resistance training complementary to aerobic training in patients diagnosed with ischemic heart disease at the Gym of Ergometry and Cardiovascular Rehabilitation of the Cardiology Service of the Provincial General Universitario "Camilo Cienfuegos" Hospital of Sancti Spiritus.
Results: The average age was 64 years and the male sex (84.62%). The main diagnosis was Acute Coronary Syndrome with ST elevation. Peak oxygen consumption increased to 22±1 ml/kg/min and METs to 8.5 (p=0.000). The blood pressure response was normal (maximum 210 mmHg) and the maximum heart rate reached was 122±54 beats per minute (p=0.00). The workload increased from 20.5±11 pounds to 38±18 pounds. No changes in physiological safety variables reported.
Conclusions: The functional capacity of the patient was significantly increase according to peak oxygen consumption and according to METs, as well as the basal heart rate and muscle strength enhanced without changes in the safety variables.
Cardiovascular rehabilitation programs (CRP) constitute a multifactorial system of action, a set of activities necessary to ensure patients with heart disease an optimal physical, mental and social condition, which allows them to occupy, by their own means, such a normal place. as possible in society. It should be noted that these programs are mainly indicated when ischemic heart disease is diagnosed. [1]
Cardiac rehabilitation procedures in people who have suffered an acute coronary infarction are closely related to the prognosis and subsequent risk of developing new infarctions (secondary prevention). The existence of associated risk factors, such as hyperlipidemia, hyperglycemia, arterial hypertension, obesity and hyperinsulinism, increase the chances of a poor prognosis and condition endothelial dysfunction; Therefore, to fulfill the main objective of improving the prognosis, it is necessary not only to reduce morbidity and mortality, but also to increase functional capacity and reform the risk factors for coronary heart disease, the psychological profile and quality of life.[1]
The precept of physical exercises, like any other therapy, must be based on a good knowledge of the benefits and risks, as well as on the particularity and individual characteristics of the patient; When this is the case, the benefits are maximum. [1]
Currently it has been shown that physical training programs reduce the mortality of patients with cardiovascular disease by around 12% for each metabolic unit (MET: unit of measurement of the metabolic rate; it is based on the amount of energy necessary for a person to remain seated and awake corresponds to 3.5-4 mL O2/kg/min=1.2 call/min) of increase in exercise capacity, so that patients with uncomplicated acute myocardial infarction are suitable for mobilization early, which could begin from the first day in the medical institution. [2]
Current medical practice seeks to prevent diseases and achieve this at the lowest possible cost. In this regard, regular physical activity can help achieve these goals, especially if it is considered a healthy lifestyle habit. The acute response to exercise produces an increase in O2 needs and sympathetic activity, which represents a potentially risky situation, so it is necessary to know the state of cardiovascular health and, failing that, the individualized behavior of the patient. want to do physical exercise. [3]
It should be noted that heart disease, in any of its four basic forms (coronary, valvular, myocardial or congenital), can alter the exchange of O2 and CO2 during physical activity. In fact, heart disease, throughout its evolution, causes a decrease in functional capacity, which can be used as an evaluation method; The loss of physical capacity is basically due to a decrease in cardiac output, which does not increase adequately during physical activity for various reasons. In the case of the patient with ischemic heart disease—in the clinical forms given by the World Health Organization (WHO), which include cardiac arrest, angina pectoris, acute myocardial infarction, heart failure and arrhythmias—the degree of involvement depends on systolic and diastolic function, as well as the anatomical and functional severity of the injuries. [3]
Cardiac rehabilitation programs (CRP) are multifactorial action systems, which were recommended by the WHO in the 60s of the last centuries, and have been defined as the “set of activities necessary to ensure cardiac patients a physical, mental and optimal social situation that allows them to occupy, by their own means, a place as normal as possible in society”; It is mainly indicated if there is ischemic heart disease, but it is applicable to all types of cardiovascular disease. [3]
Currently, the benefits in terms of cost-effectiveness of cardiac rehabilitation and secondary prevention (PR- Cuyp’s) programs have been identified, determining a significant improvement in quality of life, reduction in mortality and recurrence of hospitalizations, this secondary to the gains obtained in maximum oxygen consumption, which allows greater tolerance to effort. [4]
The objective of this work is to evaluate the behavior of physiological variables after the application of cardiovascular rehabilitation with resistance training to patients with a diagnosis of ischemic heart disease in the Ergometry and Cardiovascular Rehabilitation Gymnasium of the Cardiology Service of the Provincial General University Hospital. Camilo Cienfuegos” from Sancti Spíritus.
A quasi-experimental before-after study was carried out without a control group with the objective of evaluating the behavior of physiological variables after the application of cardiovascular rehabilitation with supervised resistance training complementary to aerobic training in patients with a diagnosis of ischemic heart disease in the Gym. of Ergometry and Cardiovascular Rehabilitation of the Cardiology Service of the “Camilo Cienfuegos” Provincial General University Hospital of Sancti Spíritus in the period from January 1 to December 31, 2018.
Study universe: consisting of the 87 patients who, during the study period, were admitted to the Ergometry and Cardiovascular Rehabilitation Gymnasium of the Cardiology Service of the “Camilo Cienfuegos” General University Hospital in the province of Sancti Spíritus with a diagnosis of ischemic heart disease on a rehabilitation. The inclusion period for the study was carried out between the months of January and June 2018. During that stage, all patients who attended the gym with a diagnosis of ischemic heart disease undergoing rehabilitation were analyzed. The sample consisted of 39 patients who met the following criteria:
Inclusion criteria:
• Patients of both sexes.
• Diagnosis of ischemic heart disease in any of its manifestations: acute coronary syndrome with ST-segment elevation (STEACS), acute coronary syndrome without ST-segment elevation (NSTEACS), chronic stable angina, ischemic heart disease after percutaneous coronary intervention (PCI) and surgery myocardial revascularization.
• Have an early evaluative ergometric study with a functional capacity (FC) equal to or greater than 4 MET, according to New York Heart Association (NYHA) criteria.
• Stable ischemic heart disease with optimal medical treatment.
• Willingness to participate in the study.
Exclusion criteria:
• Patients with unstable angina, significant ventricular arrhythmias, heart failure and blood pressure equal to or greater than 140/90 mmHg in the previous two weeks.
• Patients with myocardial ischemia and/or hypo or hypertensive response in the stress test.
• Present diseases of the osteomyoarticular or neurological systems that prevent physical training.
Discontinuation criteria:
• Suspended on two or more occasions from the rehabilitation program due to decompensation of his underlying illness.
• Voluntary abandonment.
• Poor adherence to treatment.
The data were processed automatically by the statistical software SPSS ( Statistical Package for Social Sciences ), version 17.0 for Windows. The results were presented using frequency distribution tables. Descriptive statistics were used to obtain the averages, standard deviations, minimum and maximum values and frequencies. The t test for related samples was applied to the quantitative variables, considering it statistically significant when p ≤ 0.01 and the 99% confidence intervals were calculated. Qualitative variables were expressed as percentages.
During the development of the research, the ethical and legal aspects were considered in obtaining the information and informed consent was obtained from the participants following the provisions of the 1976 Helsinki Declaration for medical research: respect for people (autonomy), beneficence, non-maleficence and justice.
During the 6 months of the inclusion period, a total of 87 patients were admitted to the Ergometry and Cardiovascular Rehabilitation Gymnasium of the Cardiology Service of the “Camilo Cienfuegos” General University Hospital in the province of Sancti Spíritus with a diagnosis of ischemic heart disease undergoing rehabilitation. Those who did not meet the inclusion criteria described above were excluded (n=23) and after the evaluation of the early evaluative ergometric test, 25 more patients were excluded from the study due to having functional capacity less than 4 MET, myocardial ischemia and hypertensive response. during the test. The remaining 39 joined the PRC. There were no losses during the study.
The distribution of patients in a resistance exercise program according to demographic and clinical variables. The average age was 64 ± 10 years with a minimum age of 37 years and maximum age of 78 years and predominance of the group from 50 to 59 years with 71.7%. Regarding sex, a predominance of males (84.62%) compared to females (15.38%) is observed. The main diagnosis for which patients attended the rehabilitation gym was Acute Coronary Syndrome, with ST segment elevation (48.72%) and without ST segment elevation (23.08%). Patients with a diagnosis of Chronic Stable Angina (12, 82%) and Myocardial Revascularization Surgery (15, 38%) had a lower representation (Table 1).
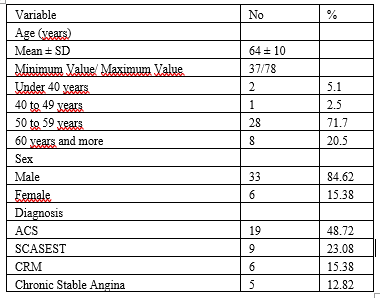
Table 1: Characterization of patients in a resistance exercise program according to demographic and clinical variables. Source: patient interview and medical examinationSTEACS: acute coronary syndrome without ST segment elevation.
NSTEACS: acute coronary syndrome with ST segment elevation.
CRM: Myocardial Revascularization Surgery.
When evaluating the behavior of the response variables before and after resistance training, it can be seen that the changes in functional capacity according to peak oxygen consumption and according to METs, as well as
in basal HR and muscle strength were statistically significant (p ≤ 0.01), while the modifications produced in the variables basal BP, peak BP and training HR were not (Table 2).
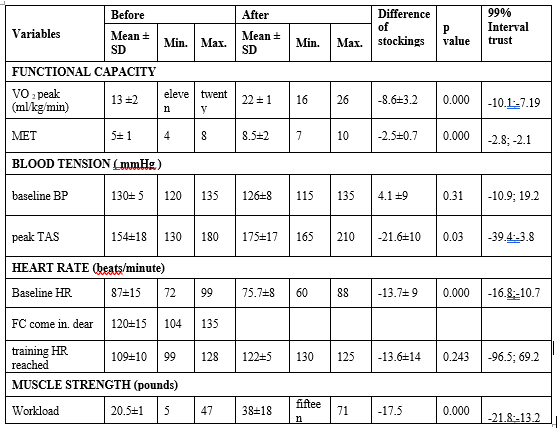
Table 2: Physiological response variables before and after resistance training.
Source: medical examinations of patients
VO 2 max: Maximum oxygen consumption. MET: metabolic equivalent
BP: Blood pressure SBP: Systolic blood pressure.
HR: Heart rate. SD: standard deviation,
Training HR: Training heart rate
Max : Maximum value. Min.: Minimum value
Before the application of PRC, functional capacity evaluated according to peak oxygen consumption was moderately to severely decreased (13±2 ml/kg/min) and later increased to 22±1 ml/kg/min (normal FC). Regarding functional capacity according to METs, this was limited in the first stress test, an average of 5±1 METs can be observed (less than 7 METs is considered high risk for cardiovascular events). In the second stress test, the modifications produced in this variable were highly significant (p=0.000), reaching 8.5±2 METs , for a mean difference of -2.5±0.7 (more than 7 METs are considered low risk for cardiovascular events). The modifications in muscle strength generally evaluated for all muscle groups before and after
ER were highly significant (p=0.00) with an increase in the magnitude of the workload for each muscle group and the subsequent increase in muscular strength and physical capacity of patients averaged from 20.5±11 pounds before rehabilitation to 38±18 pounds after.
The behavior of the physiological safety variables TAS, TAD and HR during resistance training is shown, it is evident that during lifting the load the response in systolic blood pressure was an average of 162 ± 8.80 mmHg , while for DBP the mean was 101±6.83 and for HR it was 113±5.70 (Table 3).
| Variables | Minimum | Maximum | Half | Standard deviation |
| Systolic blood pressure (mph) | 150 | 175 | 162 | 8.80 |
| Diastolic blood pressure (mmHg) | 95 | 110 | 101 | 6.83 |
| Frequency Cardiac (beats/minute) | 110 | 125 | 113 | 5.70 |
Table 3. Physiological safety variables during resistance training
Source: medical examinations of patients
In relation to age and sex, these results coincide with those of Domínguez et al., ( 5) where males predominated and maximum oxygen consumption improved from 15.6 ml/kg/min to 24.3 ml/kg/min. min. In Atef and Abdeen [6] a total of 30 patients were randomly distributed into 2 groups (15 patients/group). No significant differences in age (P = 0.77; P > 0.05), weight (P = 0.71; P > 0.05), height (P = 0.49; P > 0.05), BMI (P = 0.55; P > 0.05) and resting heart rate (P = 0.99; P > 0.05) between groups A and B.
Coinciding with the results of a similar study carried out by Arias et al., [7] functional capacity increased in the incremental stress test (1.76 METS; 95% CI 1.59 to 1.96 p < 0>
In Ortega et al., [8] the male sex was the most prevalent with 64 (87.7%) with an N = 73, and a mean age of 54.5 ± 8.7, a statistically significant decrease was observed. of systolic blood pressure (p= 0.041), but not diastolic blood pressure (p= 0.170). Statistically significant differences were obtained in all stress test parameters (p <0>
In Heyden [9] where a combined phase II cardiovascular rehabilitation exercise program was evaluated, VO2 improved by 7.34% with a magnitude of change of 1 ml/kg/min, p<0>
Główczyńska et al., [10] worked with 850 enrolled patients, 291 (34.2%) patients had MD, 425 patients were assigned to the hybrid comprehensive telerehabilitation (HCTR) group, the Cardiopulmonary Stress Test (CPET) was performed twice before and after the telerehabilitation program in 385 patients, 129 (33.5%) had diabetes mellitus (DM) (HCTR-DM group) and 256 patients (66.5%) did not have DM (group HCTR-no DM), 425 patients assigned to the usual care (UC) group CPET was done twice in 397 patients, 137 (34.5%) had DM (UC-DM group) and 260 patients (65.5%) did not had DM (CU- nod group ). At the time of randomization, the ventilator anaerobic threshold was higher in patients without DM compared to patients with DM either after HCTR (15.9 ± 5.7 vs. 13.6 ± 4.5 [ ml/kg/min], < 0 xss=removed>
Betancourt et al., [11] in their study, oxygen consumption showed an increase of 3.6 ml/kg/min during rehabilitation, finding statistically significant differences in the three measurement moments, but a greater increase was evident between weeks 1 and 6 (p = 0.00), when a change of 2.2 ml/kg/min was recorded. The measurement of initial and final systolic/diastolic blood pressure showed a decrease (p < 0>
Regular physical activity in patients with cardiovascular diseases reduces the risk of death. Physical exercises improve cardiorespiratory function in various situations, which is why it is important to use it as a form of prevention and treatment of ischemic heart disease.
Resistance training complementary to aerobic training in patients with ischemic heart disease undergoing cardiovascular rehabilitation significantly improved the patient's functional capacity according to peak oxygen consumption and according to METs, as well as basal heart rate and enhanced muscle strength without alterations in safety variables or appearance of cardiovascular complications during training. Cardiac rehabilitation programs are beneficial to achieve better control of cardiovascular risk factors, lifestyle changes and functional capacity.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
