
case report | DOI: https://doi.org/10.31579/2834-5142/028
1 Department of Nursing, Intensive Care Unit, University of Arkansas for Medical Sciences, Little Rock, Arkansas, USA.
2 Department of Geriatrics, College of Medicine, University of Arkansas for Medical Sciences, Little Rock, Arkansas, USA.
3 Department of Nephrology, College of Medicine, University of Arkansas for Medical Sciences, Little Rock, Arkansas, USA.
*Corresponding Author: Manisha Singh, Department of Nephrology, College of Medicine, University of Arkansas for Medical Sciences, Little Rock, Arkansas, USA.
Citation: Julie Daniel, Masil George, Manisha Singh (2022). Physician Assisted Death -An Ethical Dilemma Revisited. International Journal of Clinical Nephrology. 4(2); DOI:10.31579/2834-5142/028
Copyright: © 2022 Manisha Singh. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 08 April 2022 | Accepted: 31 May 2022 | Published: 06 June 2022
Keywords: physician-assisted death; end-of-life care; euthanasia; ethics; goals of care
Physicians often face ethical dilemmas when providing advice regarding withdrawal of care. In the nephrology world, we are especially at risk due to the high mortality of our patients. Yet our training tends to lag behind in certain aspects of end of life goals of care discussions. Some of our patients enquire regarding physician-assisted death (PAD) as an option and our current training does not enable us to provide an informed answer. In end-stage-renal patients, opting out of dialysis will certainly result in a rapid demise for most, however, some patients request further assistance. We updated information to be, at the least, able to help our most vulnerable patients with the information. The process of dying, sometimes prolonged to weeks, is a very painful procedure, and not under the patient's control.
Withdrawal of care, even with the best palliative care options, does not always result in the control that physician-assisted death (PAD) can provide. It appears as a reasonable option to some patients at the end of life. Is PAD a part of doing “everything that can be done” to keep a patient comfortable (as a part of comfort goals of care)? The provision exists in certain states. However, moving to another state at the end of life is not really practical or even a kind option to consider.
A physician can have moral and ethical dilemma around these queries. Our paper discusses available data on this issue intending to empower providers with optimal information. Professional position guidelines do not agree with or recommend physician-assisted-death. This knowledge helps clear the conscience of providers knowing that, at the least, we are doing what most other physicians would do. The question remains: Is PAD a part of “everything that can be done” for the patient? This manuscript aims to update regarding this issue especially as there have been recently active discussions worldwide with the launch of newer technology-assisted death.
We present a case modified extensively from real life cases for academic discussion only. We do not provide any recommendation regarding the practice.
Physician assisted death is legal in California, Colorado, District of Columbia, Hawaii, Maine, New Jersey, Oregon, Vermont, and Washington. Medical aid in dying is legal Montana via court decision, but there is no statute in place. Over half of the American states have considered enacting laws to allow mentally competent adult residents with a terminal illness to voluntarily request and receive a prescription medication that would allow the person to die at a time of their choice [1]. 73% of the American public [2]and 55% of physicians [3] support aid in dying for the terminally ill. In the United States, less than 18% of physicians report having received a request for PAD, and less than 5% have complied [4]. This highlights the fact that requests for PAD are infrequent, and only a small percentage is carried through. PAD can be legally practiced in other countries such as Netherlands, Switzerland, Belgium, Luxembourg, Columbia and Canada. While the majority of physicians support medical assistance for the dying individual, only a small number of practitioners are both willing and able to provide this service.
Mr. KD is a 66 year old man on in-center hemodialysis for renal failure. He makes the following request: “Doctor, could you please change something while I am on dialysis to stop my heart?” Mr. KD developed renal failure four years ago and has been on dialysis since. His comorbid medical problems include lung cancer (for which he receives palliative chemotherapy), diabetes, poorly controlled hypertension, recurrent infection with Clostridium Difficile (three times over six months), and congestive cardiac failure with preserved ejection fraction. When we discussed goals of care, he stated that he did not want to stop dialysis to wait for death to happen over a course of several days. He wanted to die at a time and location of his choice, especially because his son was deployed overseas and he wanted his son to be present at the bedside at the time of his death. It was also important to him to have mental clarity up to the point of death.
Mr. KD had done some research and mentioned how some states have the provision of physician assisted death (PAD) and wondered if he could relocate to a state that allows him to access this.
Commonly used terms to describe expedited death process are explained below. The terms PAD and euthanasia are sometimes used synonymously. Comfort care goals are to prevent or relieve suffering as much as possible and to improve quality of life while respecting the dying person’s wishes. However, there is a major difference as illustrated in the table below.
Euthanasia | Physician Assisted Death | Comfort care/ Withdrawal of care/hospice |
Physician prescribes the medication for the purpose of causing death. | Physician prescribes the medication for the purpose of causing death. | Physician assists in comfort measures, curative intent medications can be continued on palliative care, whereas in hospice such attempts are stopped with the sole purpose to keep the patient comfortable symptomatically. |
Physician directly administers the medications for the purpose of causing death. | Patient administers the medication for the purpose of causing death. | Physician directly administers the medications for use for comfort measures. |
Table 1: Types of physician assistance in the process of death
Date | Case | Outcome |
June 1997 | Washington v. Glucksberg [Error! Reference source not found.] | Court rules: no constitutional violation by the states in banning PAD. The court left the matter of the right to a physician's aid in dying to the states. |
October 1997 | Oregon's Death with Dignity Act becomes law [Error! Reference source not found.] | Allows terminally ill Oregonians to end their lives through the voluntary self-administration of lethal medications, expressly prescribed by a physician for that purpose. |
November 1998 | Pathologist and PAD advocate Jack Kevorkian charged with murder [Error! Reference source not found.] | Media attention generated. Convicted of second degree murder in 1999; served eight years in prison. |
November 2008 | Washington's initiative, the Death with Dignity Act, is passed | Effective March 2009: Allows Washington residents with less than six months to live to request lethal doses of medication from medical and osteopathic physicians. |
December 2009 | Baxter v. Montana [Error! Reference source not found.] | Rights of the Terminally Ill Act protects aid prescribing physician from liability. |
November 2012 | Massachusetts initiative defeated | Death with dignity vote defeated by 51% (1.52 vs. 1.45 million) |
May 2013 | PAD legalized in Vermont. | Patient Choice and Control at End of Life Act: residents with terminal disease have the option to be prescribed a dose of medication to hasten the end of their life. |
Jan 2014 | New Mexico: Morris v. Brandenburg | In Bernalillo County, an individual's right to die is upheld. |
November 2014 | Brittany Maynard ends her life in Oregon after moving from California | Social media attention generated, encouraging a review of the California law. |
October 2015 | California’s End of Life Option Act signed to law | Legalizes physician-assisted death for Californians with terminal illnesses. |
December 2016 | Colorado’s Proposition 106 goes into effect | End of Life Options Act: made assisted death legal among patients with a terminal illness who receive a prognosis of death within six months. |
February 2017 | District of Columbia’s Death with Dignity Act goes into effect | Washington, D.C. is the sixth jurisdiction in the U.S. to enact an assisted dying statute. |
May 2018 | Ahn v. Hestrin | California’s End of Life Option Act was overturned by a county judge on a technicality. |
June 2018 | California’s End of Life Option Act reinstated | The Court of Appeals issued an immediate stay to the previous month’s judgment, putting the law back into effect. The court gives until July 2nd to file objections. |
January 2019 | The Hawaii statute, the Our Care, Our Choice Act, goes into effect | Allows patients the ability to choose their own medical care at the end of life and, at the same time, ensure robust safeguards are in place to prevent any possible abuse. |
September 2019 | New Jersey and Maine laws have been enacted | New Jersey’s Medical Aid in Dying for the Terminally Ill Act goes into effect in August. The Death with Dignity Act in Maine follows by September. |
June 2021 | New Mexico’s End of Life Options Act goes into effect | New Mexico becomes the 10th jurisdiction to enact a PAD law. |
March 2022 | Oregon removes the residency requirement in the state’s Death with Dignity Act [Error! Reference source not found.] | In a settlement to a lawsuit brought by a physician, Oregon will no longer enforce the residency requirements to receive PAD prescriptions, and the state agrees to submit a repeal for the requirement in the next legislative session. |
Table 2: Major landmarks [Error! Reference source not found., Error! Reference source not found.]
In America, the lower courts (district courts and courts of appeals) decided that death is a fundamental right protected by the constitution, but these rulings were later reversed by the Supreme Court. The Supreme Court concluded that, while there may be a liberty interest involved, the constitution does not protect this right. The state’s interest in preserving life is therefore considered more legitimate than the need to protect such freedoms. The Supreme Court did emphasize that the states would be responsible for deciding legislation.
Interestingly, constitutional law only “protects those fundamental rights and liberties which are, objectively, deeply rooted in this Nation's history and tradition” [Error! Reference source not found.]. This creates a backwards-facing judicial system that often has difficulty keeping up with the pace of science and technology, but does create a buffer that isolates short-lived swings of opinion and influence from the law.
In Oregon, where physician assisted suicide has been allowed since 1997, the statistics shed light on practical application of this provision. Nearly all of the patients were white (96.5%), and only one African American has died under this statute since its inception. 73.3% of patients had at least some college education, and nearly half (43.7%) had a bachelor’s degree or higher [Error! Reference source not found.].
Those who do not live in a jurisdiction that allows medical assistance in dying could potentially relocate to a state that does. As a result, most patient-physician relationships average only eight weeks [Error! Reference source not found.]. The physical, financial, and social burdens of traveling to another state while severely disabled or terminally ill are usually too great for those near the end of life.
Common causes for patient requests for aid in dying
Against popular belief, pain control is only reported as an end-of-life concern in 25% of cases that have utilized Oregon’s Death with Dignity Act. The loss of autonomy (91%), inability to engage in activities that make life enjoyable (90%), and the loss of dignity (76%) are the most frequently cited reasons. In contrast, financial implications are rarely a factor (4%), whereas nearly half are concerned about the loss of bodily functions (46%) or the burden placed on caregivers (44%) [Error! Reference source not found.].
Other causes include the following [Error! Reference source not found., Error! Reference source not found.]:
1. Illness related experience
2. Sense of self:
3. Fears about the future:
Ethical and legal concerns
In a world where our fates are no longer decided by the capriciousness of nature, does living eventually become a greater burden than dying? Could it be considered torture to force someone to stay alive far longer than they desire, especially if death is inevitable within a limited time span?
Healthcare providers are moral agents whose conscientious objection should be respected within the bounds of reasonable accommodation. The statutes currently in place in America protect providers and organizations who wish to refrain from prescribing or dispensing lethal medications. If a practitioner wishes to participate in assisted dying but is operating from a facility or within the staff of an entity that prohibits it, they may be subject to discipline or termination. However, they may still operate outside the scope of the sanctioning organization or as an independent contractor without punishment.
It is an ethical imperative for a patient to be aware of and have access to all services to which they are entitled. In the event that a provider objects to a patient’s request, they are obligated to refer them to another professional who is willing to comply. Similarly, care teams should be aware of the laws and policies relating to their local practice. If a patient requests aid in dying but cannot obtain it within the jurisdiction, providers should offer information on locations and facilities that provide the service.
The states currently allowing aid in dying have very similar laws which provide numerous safeguards to protect both patients and providers. Prior to March 2022, the patient was required to prove residency in the jurisdiction, though there was no minimum length of residency required. Participation is voluntary for all involved, and it is a felony similar to first degree murder to coerce or unduly influence someone to request the medication.
The positions of medical associations tend to remain conservative until after local laws have been enacted, and generally echo judicial findings. Most professional groups such as the American Academy of Hospice and Palliative Medicine were once opposed to PAD, but are increasingly taking a position of “studied neutrality” [Error! Reference source not found.].
The main concern cited by opponents of the laws is that certain populations of patients will be particularly vulnerable to abuses within the system. Such populations include those of lower income or educational status, the elderly, patients with dementia, and others [Error! Reference source not found.]. However, there have been no legitimate cases of abuse reported in America to date. Other complicating moral factors when considering PAD include concerns over surrogates’ conflict of interests, coercion or undue influence, and capacity assessments in the case of such requests. The dual axioms of beneficence and non-maleficence are guidelines that can only be defined by an action’s relative injury [Error! Reference source not found.]. This means that the ethical considerations of each case must be evaluated individually.
Current understanding of the process of PAD
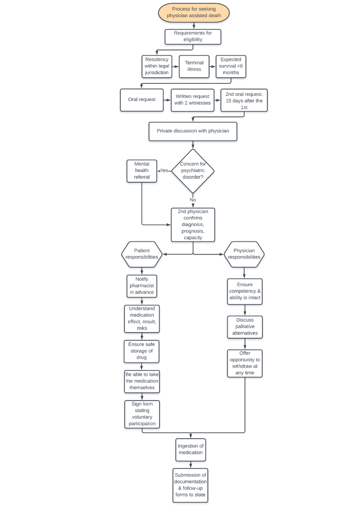
Our interpretation based on the above information incorporating the different states’ approach to PAD is as follows. The process begins with a patient making two separate oral requests for aid-in-dying at least fifteen days apart. They must sign a written request in the presence of two witnesses, one of which is an uninterested party. They must discuss their wishes with the attending physician without anyone else present (except an interpreter) to ensure that the decision is voluntary. The physician will evaluate the patient’s competency for informed, rational consent, as well as their physical ability to take the medication themselves. The patient would be referred to a second physician to confirm the diagnosis, prognosis, and decisional capacity. If either physician suspects the patient may have a psychiatric disorder, they must also be referred to a mental health specialist for evaluation.
The patient should express understanding of the effects of the medication, the probable result, and the potential risks involved. The physician would clarify that the patient can take the drug whenever they want, but can choose not to take it at all or withdraw the request at any time. They should understand the importance of maintaining the drug in a safe and secure location until they are ready to ingest it. They would discuss realistic alternatives including comfort care, hospice, palliative treatment, and pain control. Finally, the provider would give another opportunity to withdraw the request. If they still desire to proceed, the physician would then write the prescription.
Before taking the medication, the patient must sign a form stating that they took it voluntarily. The attending physician is required to submit thorough documentation and a follow-up form to the state according to local laws. No contract, will, insurance policy, or other agreement may be conditioned or affected by a person’s request or denial of medical aid in dying. Death after ingestion of the drug is not considered suicide or homicide, but a natural death resulting from the underlying disease.
At a time of astronomical advances in medicine and technology, the speed of progress necessitates frequent reviews of our beliefs about medical, societal, and personal ethics. While we have succeeded in prolonging life beyond its “natural” end, the sectarian belief that physicians have no part in death may need further discussion. Physicians must continually examine their understanding of the cycle of life and death, patient rights to know their choices, and access to such care.
Acknowledgements
Authors report no conflict of interest. All listed authors are in authority for the content and subsequent revisions of the article and have contributed equally.
Funding
No funding sources.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
