
Research Article | DOI: https://doi.org/10.31579/2768-0487/028
1Specialist general surgery Dubai hospital UAE.
2Head of General Surgery Department Liaquat National University Hospital Karachi, Pakistan.
3Consultant General Surgeon Indus Hospital Karachi,Pakistan.
4Associate Professor General Surgery Siut Karachi, Pakistan
5General Surgeon Siut Karachi, Pakistan.
6Consultant General Surgeon Liaquat National Hospital Karachi, Pakistan.
7Specialist Internal Medicine Dubai Hoapital Dubai, UAE
*Corresponding Author: Aliya Ishaq, Specialist general surgery Dubai hospital UAE.
Citation: A Ishaq, R soomro, N Lodhi, Muhammad S Khan, A Parveen, et al. (2021) Phyllodes Tumor of Breast:A 17 Years Audit of 260 Patients with Biopsy Proven Phyloldes Tumor Treated in our Institute. Journal of Clinical and Laboratory Research. 3(1); DOI:10.31579/2768-0487/028
Copyright: ©2021 Aliya Ishaq. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 27 May 2021 | Accepted: 08 June 2021 | Published: 11 June 2021
Keywords: phyllodes; breast neoplasms; benign; malignant
Phyllodes are rare breast neoplasms with higher rate of local and systemic recurrence. This study presents the results of an audit of all cases of biopsy proven phyllodes tumor presenting to breast services in Liquat National University Hospital Karachi, Pakistan, from 1993 to 2010. Total 260 female patients were retrospectively audited, 151 had benign, 35 borderline and 74 had malignant histology. Mean follow up duration for all types was 2 years. The mean age for benign lesions was 28, for borderline 36.8 and for malignant lesions 41 years. For all histopathological types the mean tumor size was 6.2 cm. It was 5.4 cm for benign, 7.8 cm for borderline and 11.2 cm for malignant lesions. 200/260 (76.9%) patients had breast conservation while 60/260 (23.0%) had mastectomy.
Histopathology type and grade has statistically significant relationship with recurrence ( p value .0001 % ) Overall recurrence rate was 20/260 (7.69%) with one patient with malignant phyllodes having recurrence 6 times despite clear margins and two patients with borderline phyllodes having recurrence twice . Tumor recurred in 2/151(1.3% ) of benign , 5.7% borderline ( 2/35 ) and 21.6% malignant ( 16/74 ) cases .Malignant group had 8 (10.8% ) systemic and 12 (16.2%)local recurrences. All patients with local recurrence and involved margins had reexcision except for 2 who had mastectomy with muscles involved posteriorly during the first surgery where re-excision was not possible. mortality rate for malignant phyllodes was 5.4 % ( 4/74 deaths as a result of systemic recurrence )
Conclusion: Phyllodes tumor is an aggressive disease, in our series, grade and type of tumor on histopathology is the significant risk factor for local and systemic recurrence with rate reaching up 21.6% for local and 10.8% for systemic recurrence in malignant lesions.
Phyllodes are uncommon neoplasms constituting less than 1 (0.3 to 0.9) percent of breast tumors [1, 2, 3, 4]. Histopathologically they are classified as benign, border line and malignant [5, 6].They are clinically, radiologically and pathologically very similar to fibroadenomas, causing diagnostic difficulties with a low pre-operative diagnostic rate [7, 1].Phyllodes have both epithelial and stromal component and it is the stromal component that has the metastatic potential. They have very high rate of local recurrence and approximately 15% tumors recur locally [8]. Factors contributing to local recurrence are positive resection margins within 1 cm, increased mitotic index, tumor necrosis, larger tumor size, stromal overgrowth, cellularity and atypia[9].Positive resection margin is one of the most important factor for recurrence.Treatment strateges are diverse,controversial and no consensus guidelines are available [10, 11].Review of literature shows small reterspective series without long term follow up[12, 13].
Genetic mutations in the chromosomal regions of +1q, +5p, +7, +8, −9p, −10p, −6, and −13 correlated with borderline and malignant phyllodes tumors of the breast [14]. Adjuvant radiotherapy is recommended in borderline and malignant PTs with tumor-free margin < 1 cm and high-risk malignant tumors. Adjuvant chemotherapy or target therapy may be helpful for metastatic PTs. Molecular and genomic techniques may predict clinical outcomes of benign and borderline PTs more precisely [15].
There is paucity of large series in literature for phyllodes tumor because of rarity of this entity and absence of long term follow ups specially for third world countries. This retrospective study have tried to answer the same questions regarding management strategies,factors associated with recurrence,role of radiotherapy and the safest minimal margin of resection but will be among one of the largest single institutional studies on phyllodes over a period of 17 years with long term follow ups of up to 15 years.
To review different management strateges of all types of phyllodes tumors,factors associated with recurrence of these tumors and to find out the safest minimm margin of resection and role of radiotherapy in preventing recurrence.
Study Design: reterospective study.
Study Place: Breast Clinic Liaquat National Hospital and medical college Karachi, Pakistan.
Duration of study: 1993 – 2010 (17 years).
Data Collection: All data was retrived and reviewed from breast clinic files patients who did not have follow up were contected via phone and OPD.
Data Analysis: All enteries were done on designated spread sheats and SPSS version 19 was used or statistical analysise .Variables including age,histopathological typ,size of tumor,type of surgery,margin of clearance including minimum and maximum margin,use of radiotherapy,follow up duration,local and systemic recurrence,time to recurrence,treatment of recurrence and mortality were analysed .Sub group analysis was done and Chi-square test was used to show statistical significance with a p-value of < 0.001 where applicable.
Inclusion Criteria:
Exclusion Criteria:
There were 260 female patients diagnosed with phyllodes tumor during the 17-year study period (1993-2010). There were 151 histologically benign lesions, 35 borderline lesions and 74 malignant lesions.
Mean follow up duration for all types was 41.3 months ± 36.37 (range 5-180 months) The mean follow-up period for benign lesions was 31.9 months (range 5-132months), for border line 36.9 months (range 5-146 months) and for malignant lesions it was 62.5 months (range 8-180 months).Over all for all three types the mean age at the time of diagnosis was 32 years (range 12-85 years). The mean ages of patients with histologically benign lesions was 28.02 years±0.98, for borderline 36.8 years ±1.9 and for malignant lesions 41 years ±1.7 .All patients presented with a palpable breast lump. There is no statistically significant co-relation between age and histopathological type (p value 0.32).
Tumor Size:
Over all for all histopathological types the mean tumor size was 6.278 cm ± 4.14 ( range 1-21 cm ).The mean tumor size for benign lesion was 5.48 cm (range 1-20 cm), for border line 7.83 cm (rang 1-21 cm ) and for malignant phyllodes it was 11.2 cm (rang 2-30 cm ). The mean size of malignant lesions was larger (11.2 cm) than benign and borderline lesions (5.8cm and 7.83 cm, respectively) and there is statistically significant co-relation between size and type of tumor (p value 0.000), the more malignant the tumor type the larger is tumor size. No statistically significant relationship between size of tumor and recurrence is noted in our study (p value .265).
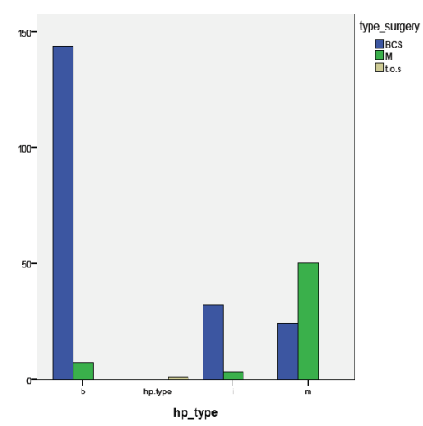
Type of Surgery:
Breast conservation (BCS) was done in 200/260 (76.9%) patients while 60/260 (23.0%) were treated with mastectomy. BCS was done in 144 (95.36%) cases of benign, 32 (91.4%) cases of bordline and 24 (32.4%) cases of malignant lesions. Mastectomy was done in 7 cases (4.63%) of benign, 3 (8.82%) cases of border line and 50 (67.56%) cases of malignant phyllodes as shown in graph below,
Recurrence:
Recurrences were noted in the present study in20/260 (7.69%) cases in 14 patients with one patient with malignant phyllodes having recurrence 6 times and two patients with intermediate phyllodes having recurrence twice once from IM to malignant and second time from malignant to malignant. Tumor recurred in 2/151(1.3% ) of benign , 5.7% borderline ( 2/35 ) and 21.6% malignant ( 16/74 ) cases in 11 patients.
Histopathology type has statistically significant relationship with recurrence (p value .0001 %), the more aggressive the histopathology type the more are the chances of recurrence. There were two patients in benign group who had local recurrence and the histopathology of recurrence for one patient was benign and for second it was intermediate. Two patients with intermediate phyllodes had recurrence and the histopathology of recurrence for both of them was malignant later on both these patients had local recurrence again as malignant phyllodes and then systemic recurrence and subsequently expired.
There was no systemic recurrence in benign and border line phyllodes tumors. Patients with malignant phyllodes had both systemic and local recurrences. For malignant phyllodes the over all rate of recurrence including both local and systemic recurrence was 16/74 (21.6%) in 11 patients. While the number of only systemic recurrences was 8 (10.8%) and number of local recurrences was 12 (16.2 %%).There were 4 patients who had both systemic as well as local recurrence.
The time to recurrence ranged from 15 days -72 months with mean time of 9.8 months ±17.46, the mean time of recurrence for individual histopathology type is 7.5 months for benign, 9 months for border line and 4.9 months for malignant lesions. All patients with recurrence were advised for WLE 0r mastectomy except for 2 patients who were advised only for radiotherapy as they already had mastectomy with excision of involved chest wall muscles and had positive margins and re-excision was not possible both of these patients expired.Out of remaining 12 patients 5 had wide local excision along with radiotherapy (41.6%) all of these 5 patients are alive without subsequent recurrence, 4 patients (33.3%) had mastectomy with radiotherapy and all these 4 patients died of systemic recurrence,one (8.3%) patient had only mastectomy without radiotherapy as tumor size was small and margins were clear ,this patient is alive with out further evidence of recurrence.One patient did not take any treatment and died of synstemic recurrence. Relationship between histipathology type and patient out come is shown below.

Out comes of surgical management.
Over all for all three types the mean margin of resection was 6.84 mm ± 4.3, while the minimum margin of resection was less than 1mm and maximum resection margin was 15 mm. 47 out of 260 18.0% patients had minimal margin of clearance of less than 1 mm. Of these 18% patients 27 (10.3%) had benign pathology, 8 (3.0%) had intermediate pathology and 12 (4.6%) had malignant lesions. When data was further analyzed for sub types it was found that number of patients in benign group who had minimum margin of clearance of less than 1 mm was 27/151 ( 17.8%),for intermediate type the figure was 08/35 ( 22.8%) and for malignant tumors it was 12/74 ( 16.2%).All these patients with minimum margin of clearance of less than 1 mm were advised re-excision except for 5 patients who were advised only radiotherapy ( out of these 5 patients 2 had mastectomy as initial surgery and posterior margin which included muscles of chest wall was positive so re –excision was not possible and only radiotherapy was advised rest of three patients had BCS ,they had maximum margin more than 1 cm at 3 or more sites and size of tumor was small so only radiotherapy was advised ).In benign subtype 27 patients with minimum margin less than 1 mm were advised re-excision but only 1 patient underwent re-excision (3.7%) rest did not under go re-excision and none of them had recurrence. In intermediate group 8 patients had minimum margin of clearance of less than 1 mm,all of these patients were advised re-excision and none of them was advised radiotherapy .None of them initially had re-excision, only one of these patients (12.5%) had recurrence after a period of 10 months as a malignant lesion and after that recurrence patient underwent mastectomy and had radiotherapy as well. In patients with malignant histopathology 12 patients had minimum margin of clearance of less than 1 mm (16.2%) Of these 12 patients in malignant group 5 patients were advised radiotherapy only for reasons mentioned above and seven were advised re-excision. Only two underwent re-excision one had BCS and second had mastectomy. Of 5 who had radiotherapy one expired with systemic recurrence rest survived and did not have local or systemic recurrence. Those who had re-excision one of these who had BCS survived with no recurrence and the one who had mastectomy with radiotherapy died of systemic recurrence. Out of remaining 4 who were advised re-excision but they did not under go re-excision 4 subsequently had no recurrence and survived and one patient lost follow up. Recurrence rate was 12.7% for patients with involved margins (minimum margin of clearance less than 1 mm ) verses 7.4% in patients with clear margins.
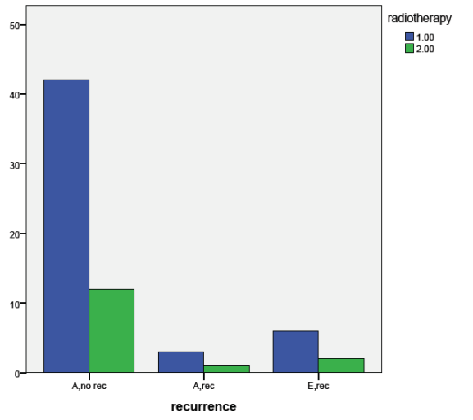
Radiotherapy:
Radiotherapy was given to 0 .19% patients (51/260). None of the patients with histological benign and intermediate tumor were given radiotherapy, all patients who received radiotherapy were histological malignant .So, and 68.9% (51/74) of malignant phyllodes patients were given radiotherapy. When recurrence was compared in patients who took radiotherapy verses who did not take radiotherapy in malignant phyllodes group it was found that 17.64% (9/15) of patients who took radiotherapy had recurrence and 20% (3/15) of patients with malignant phyllodes who did not take radiotherapy had recurrence however, this was not statistically significant ( p value 0.979%).This is shown in graph below.
Where,
Phyllodes tumors of the breast have a diverse range of biologic behaviour. The mainstay of treatment of non metastatic tumors is complete surgical resection with wide resection margins (atleast 1 cm) [9]. Wide local excision of tumor with 1 to 2 cm margin is the treatment of choice for border line and malignant tumors however for benign tumors 1mm margin of excision is sufficient and in benign tumors some literature supports wait and watch policy for tumors having positive margins [1]. In the study conducted by Chen et al. [2], surgical margin ( < 1 cm ) was significantly correlated with recurrence (P <0.001 ); In our study margins were considered as positive when the minimal resection margin was less than 1mm as apposed to other studies which took 1 cm as clear margin9,16,17,18.Further more the mean resection margin in our study was 6.48± 4.3 mm.In our study only 1.3% of benign and 5.7% of intermediate tumors recurred locally with minimum margin of clearance of 1 mm . 17.8% of our patients with benign phyllodes had minimum margin of clearance of < 1mm and none of them had local recurrence over a mean follow up period of 41.3% months.22.8% of our patients with borderline phyllodes had positive margins and only one of these patients had recurrence rest did not have recurrence. Our patients with malignant phyllodes have 21.6% recurrence and only 12.5% of these patients ( 2 patients ) had positive margins ( < 1mm ) in rest margins were clear ( > 1mm ).In our study margin of clearance of > 1mm has almost similar results as achieved in other studies that have minimum margin of clearance of up to 1 cm [9,17,18]. In our study clear margin (> 1mm) was found to be significant risk factors for recurrence (p value 0.0001%) as 12.7% of our patients with involved margins have recurrence as compare to 7.4 % with clear margins.
The analysis of data from the Surveillance, Epidemiology, and End Results (SEER) Program for the years 1983e2002 demonstrated that local failure rates for benign tumors range between 5.15% and 20.30% for malignant tumors [3, 4]; and in approximately 22% of cases, malignant phyllodes may give rise to haematogenous Over all rate of systemic. Metastasis for all types of phyllodes is 10% and for malignant phyllodes alone the rate of systemic metases is 20 %, local recurrence does not predict distant metastasis [5].The most frequent sites of distant metastases are the lungs followed by soft tissue, bone, and pleura [6]. In our study, 1.3% of benign, 5.7% if border line and 16.2% of malignant phyllodes had local recurrence.In our study, 10.8% of malignant phyllodes had systemic recurrence while the overall rate of systemic recurrence for all three types in our study is 3.76%.The common sites of systemic recurrence in our study were lungs,soft tissues and bone.
In the M.D. Anderson series of 101 patients, large tumor size was implicated as having an increased risk of recurrence [7].In our study tumor size was not found to be a significant risk factor for recurrence (p value 0.26%).
In our study, histopathological type was found to be a significant risk factors for recurrence (p value 0.0001%) with recurrence rate of 21.6% in malignant as compare to 5.7% in intermediate and 1.3% in benign group.
There is no proven benefit of radiotherapy or chemotherapy although radiotherapy may prove beneficial [8, 9] and some supports that radiotherapy should be given in malignant phyllodes for lumps of 2 cm or more in size if lumpectomy is done and for tumors of 5 cm or more if mastectomy is done [10, 11]. In two recent studies adjuvant radiotherapy was associated with better local control. Belkacémi et al [12]. Conducted a retrospective study in which 9% of patients received adjuvant radiotherapy. In the malignant and borderline group (n ¼ 159), radiotherapy significantly decreased local recurrence (p ¼ 0.02). In a prospective study, 46 patients with borderline or malignant phyllodes underwent breast-conserving surgery (with negative margins) were treated with adjuvant radiotherapy. In this study, after a median follow-up of 56 months, none of the 46 patients developed local recurrence [29].In our study after median follow up of 41.3 months 17.64% of patients with malignant phyllodes who took radiotherapy had recurrence compared to 20% who did not take radiotherapy but this value is not statistically significant (p value 0.979) and the other factor is that we did not give radiotherapy to any of the patient with intermediate phyllodes.
The role of endocrine therapy, such as tamoxifen has not fully understood in phyllodes tumours. Oestrogen and progesterone receptor expression has been shown in 40% and almost 100%, respectively. The use of endocrine therapy in either adjuvant or palliative setting has not been proven.Stromal c-kit positivity and epithelial endothelin-1 negativity are more often associated with malignant phyllodes tumour. The overall positive rate of c-kit immunoreactivity was 13% in benign and 67% in malignant phyllodes tumour.17 Endothelin-1 epithelial cytoplasmic staining was seen in 100% of benign and 17% of malignant phyllodes tumour [28].
Factors associated with recurrence of phyllodes tumors are histopathology type,size of tumor,margin of excision and use of radiotherapy in case of malignant phyllodes.
The mainstay of treatment of non metastatic phyllodes is complete surgical resection with resection margins of more than 1 mm. Phyllodes tumors have higher incidence of local recurrence with malignant lesions having more propensity to recur than benign. Histopathology type of recurrent tumor is always more aggressive than the original tumor. Systemic recurrence is one of the bad prognostic marker as all of patients in our series and all of our patients with systemic recurrence died. Radiotherapy should be given to patients with malignant phyllodes after discussion with oncologist and criteria need to be established for recommending radiotherapy in malignant phyllodes tumors.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
