
Research Article | DOI: https://doi.org/10.31579/2641-0419/098
*Corresponding Author: Lairikyengbam SKS, Chief Cardiologist, SKY Hospital & Research Centre, Imphal, India.
Citation: Lairikyengbam SKS, Ramdeo Yadave., Moirangthem Vidyathoi Devi (2020) Pharmaco-Invasive Therapy for Acute ST-Elevation Myocardial Infarction. - A Viable Alternative to Primary Percutaneous Coronary Intervention. J. Clinical Cardiology and Cardiovascular Interventions, 3(12); Doi:10.31579/2641-0419/098
Copyright: © 2020 Lairikyengbam SKS, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 23 October 2020 | Accepted: 09 November 2020 | Published: 13 November 2020
Keywords: thrombolysis; pharmaco-invasive therapy.
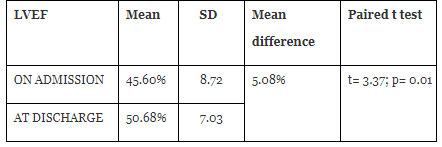
Primary percutaneous coronary intervention (pPCI) is considered as the preferred treatment for acute ST-Elevation myocardial infarction (STEMI). However, its availability is limited to less than 10% in rural and sub urban population in India (1). Therefore, Pharmaco-Invasive Therapy (PIT) (Thrombolysis first followed by planned coronary stenting) as an alternative to pPCI for acute STEMI has more recently been explored. A retrospective observational study of 60 patients with acute STEMI treated at the Dedicated Heart Attack Treatment Centre of SKY Hospital & Research Centre, Imphal, India over a period of 2 years has shown that Pharmaco-Invasive Therapy improved survival of patients with acute STEMI to 100% and increased Left Ventricular Ejection Fraction (LVEF) by 5.08% at the time of discharge and may be used as a viable alternative to pPCI in the treatment of patients with acute STEMI when pPCI cannot be performed within recommended time.
Cardiovascular disease is World’s first fatal disease. It contributes to 30% of global mortality and 10% of the global disease burden [2, 3]. Myocardial Infarction (MI) is one of the five main manifestation of coronary artery disease (CAD) [4]. In epidemiological studies, the incidence of myocardial infarction in a population can be used as a proxy for estimating the CAD burden [4].
Acute ST-Elevation myocardial infarction results from sudden total or subtotal occlusion of one or more coronary artery [5]. Early revascularisation of the occluded coronary artery is the principle of treatment for such patients presenting within 12 hours of onset of symptoms, preferably within 30 minutes of arrival to hospital. Primary percutaneous coronary intervention is the recommended treatment strategy for acute STEMI, if the same can be performed within 120 minutes from the first medical contact (FMC) [6]. However, there are several hardles to be overcome to achieve this target in many areas of the World. Availability of PCI facility with skilled manpower is limited to few centres of big cities [5]. Furthermore, to do timely pPCI for acute STEMI in many such centres may not always be practically possible 24 hours a day. The aim of this paper is to study if Pharmaco-Invasive Therapy is as effective as pPCI for acute STEMI
Material and Method
The present study was conducted at SKY Hospital & Research Centre, Imphal, India. Data of eighty patients with acute STEMI admitted over 2 years ending February 2020 were collected. Out of this, 60 patients who received Pharmaco-Invasive Therapy were included in the study. Patients with acute STEMI who presented with acute stroke, multi-organ failure or who died within one hour of presentation to the hospital were excluded from the study. In the study, the remaining 60 patients whose coronary angiogram showing > 70% residual diameter stenosis of the culpil lesion after Thrombolytic Therapy were included. The time interval in minutes between the arrival at the hospital to the start of thrombolysis was obtained. The time interval in hours from the time of thrombolysis to the time of coronary stent implantation of each case has also been obtained.
Complete history and clinical examination of all the 60 patients were carried out, including 12 lead ECG, troponin-T test, routine laboratory investigations, chest x-ray (CXR) etc. Bedside echocardiogram was provided to all the patients with acute MI on admission and at discharge. The diagnosis of STEMI was made using World Health Organization (WHO) definition and diagnostic criteria of MI [4].
All patients were seen in the Dedicated Heart Attack Treatment Centre (HAC) which was established at SKY Hospital & Research Centre in July, 2016 providing 24 hours emergency service specifically for patients with suspected M.I. Our HAC Team consists of Consultant Cardiologist/middle grade Cardiologist on site, other Emergency Medical Officers, well trained nurses and technicians. In the HAC, ECG was given to all the patients within 5 minutes of presentation to the Emergency Room (ER). Loading dose of dual anti-platelet (DAP) therapy was given within 15 minutes to all the patients who were diagnosed with STEMI. After ruling out any contraindication (such as increased risk of bleeding), thrombolysis was given using fibrin specific fibrinolytic agents. Injection reteplase [dosage: 10 units intravenous (IV) over 2 minutes (1st dose), followed by 10 units IV over 2 minutes (2nd dose) after 30 minutes], or Injection tenecteplase (dosage 30 mg IV for patients weighing less than 60 kg, 35 mg IV for patients weighing 60 kg - 69 kg, 40 mg IV for patients weighing 70 kg - 79 kg, 45 mg IV for patients weighing 80 kg - 89 kg, 50 mg IV for patients weighing ≥ 90 kg ) [7]. All thrombolysed patients also received Inj. enoxaparin as per protocol.
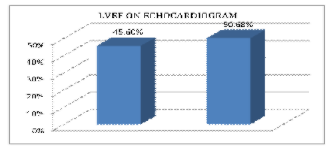
All patients received thrombolysis within 12 hours of admission, majority 40 (76%) within 30 minutes (Table-1) and coronary stenting within 10 days. All patients with STEMI received Echocardiogram to estimate Left Ventricular Ejection Fraction (LVEF) on admission and at discharge (Figure-1).

Following our discharge protocol which included, among others, mobilization for at least 100 steps on level without angina and dyspnea, all patients who received the PIT were discharged home with a 12 days median length of hospital stay.
With respect to survival rate, all the sixty patients who received Pharmaco-Invasive Therapy during the study period survived at the time of discharge.
Revascularization of an occluded coronary artery as early as possible is the principle of treatment for patients with acute STEMI [5]. Timely performed primary PCI is considered as the preferred treatment strategy for acute STEMI. When this treatment cannot be provided within the recommended time, Pharmaco-Invasive Therapy has been tried with comparable outcome [8]. The STREAM trial [8] clearly showed that PIT and pPCI were comparable in the rate of primary composite end points (death, reinfarction, cardiogenic shock, heart failure at 30 days) in the treatment of acute STEMI if pPCI could not be performed within 60 minutes of presentation to Emergency Department. The STEPP-AMI study [9] also demonstrated that Pharmaco-Invasive Therapy is not inferior to primary PCI in the treatment of acute STEMI with similar outcome at 2 years of follow up. However, it remains unclear whether late presenters will benefit from the STREAM like PIT. In our study it is possible that establishment of Dedicated Heart Attack Treatment Centre at SKY Hospital helped provide a quick diagnosis, loading dose of DAP, 3rd generation Thrombolytic agent and Enoxaparin which might have helped restore at least partial coronary blood flow distal to the culprit lesion which subsequently got balloon-dilated and stented. It was also observed that there was no case of failed thrombolysis in our study-population in comparison to 12.1% in STEPP-AMI study.
Conclusion
Pharmaco-Invasive Therapy for acute STEMI in a well fashioned Dedicated Heart Attack Centre has shown improved survival along with increased left ventricular ejection fraction. This treatment strategy may be considered as a viable alternative to primary PCI for emergency treatment of acute STEMI in many developing countries where timely primary PCI cannot be performed. Large clinical trials may help further substantiate the finding of the present study.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
