
Research Article | DOI: https://doi.org/10.31579/2692-9759/137
Department of Internal Medicine, Pietersburg Provincial Hospital, Limpopo University, Polokwane, South Africa.
*Corresponding Author: Galina Bogoslovskaya, Department of Internal Medicine, Pietersburg Provincial Hospital, Limpopo University, Polokwane, South Africa.
Citation: Galina Bogoslovskaya, (2024), Peritoneal Tuberculosis Presenting as Chronic Ascites with Scrofula: A Case Report, Cardiology Research and Reports, 6(4); DOI:10.31579/2692-9759/137
Copyright: © 2024, Galina Bogoslovskaya. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 09 July 2024 | Accepted: 19 July 2024 | Published: 29 July 2024
Keywords: chronic ascites; extrapulmonary tuberculosis; ovarian cancer; peritoneal tuberculosis, scrofula
Bacteria are one of the factors that cause skin infections. Staphylococcus aureus was the most prevalent type, and because of the frequent use of antibacterial, many of them have become resistant. From this principle, this study was conducted at the Faculty of Medical Technology, Islamic University, from January 2023 to May 2023, and the aim of the study is to investigate and detect bacteria that cause skin infections and test the antifungal synergy of with the antibacterials. the results show (Staphylococcus aureus 45%, Escherichia coli,35%, pseudomonas aeruginosa 8%, Staphylococcus epidermidis 5%, klebsiella pneumoniae %4 and proteus mirabilis 1%) and it is necessary to test new antibiotic. The combination of the antifungal itraconazole with the antibacterial amoxicillin, norfloxacin and trimethoprim was tested, and some results gave a higher effect compared to the antibacterial. It is possible to use these synergies for skin infections, and we conclude that the anti-fungal has an effect on the bacteria when it is mixed with other antibiotics.
Despite the availability of effective treatments and the use of live attenuated vaccines in many parts of the world, tuberculosis (TB) remains one of the deadliest communicable diseases. Peritoneal TB (PTB) is seen in 4.9% of all extrapulmonary TB (ETB) cases [1]. Although TB affects the lungs in the majority of patients, ETB is the initial presentation in approximately 20% of adults, and it primarily involves the lymph nodes and pleura. ETB occurs more commonly in immunosuppressed individuals and young children. In those individuals with the human immunodeficiency virus (HIV), it occurs in more than 50% of the cases [1]. Although the Republic of South Africa has made notable progress in reducing the TB prevalence and deaths due to TB, as well as improving the treatment outcomes for new sputum smear-positive TB cases, the TB burden is still enormous [2].
Ovarian cancer is one of the most difficult gynecological cancer types to diagnose because of its nonspecific symptoms. In these cases, PTB is one of the differential diagnoses because it can mimic the pattern of advanced ovarian cancer while increasing the serum markers, such as cancer antigen 125 (CA125), that are classically associated with this cancer type. In a study by Oge et al., among 612 patients who underwent surgery for suspected ovarian cancer, 20 of the cases (3.2%) were diagnosed postoperatively with PTB [3]. Here, we have reported a new case of PTB that simulated ovarian cancer.
Case Description
A 27-year-old, female who had a normal vaginal delivery six months previously was referred to the internal medicine department for an evaluation of massive ascites causing severe abdominal distension, nausea, vomiting, bloating, and a weight gain of 4 kg in five months. She had no associated past medical history, and her symptoms became progressively more severe during the subsequent two months. Primarily, she underwent diagnostic testing for ascites by her general practitioner (GP), and it was determined that her CA125 level was elevated (428 kU/l; the normal limit is 0–35 kU/l). An exploratory laparotomy was performed by a gynecologist based on the suspected diagnosis of an ovarian malignancy. However, an ovarian malignancy was not found during the operation, and a peritoneal biopsy was conducted. She was discharged after the surgery.
While awaiting the results of the peritoneal biopsy, this patient experienced pain and tenderness in the right side of her neck, and she felt a small lymph node in the cervical region. At the same time, she began to exhibit a low-grade fever and sweating. Based on the above-mentioned background information, she was referred to the Pietersburg Provincial Hospital Internal Medicine Department for a diagnostic review and admission.
Upon examination, this patient appeared ill but afebrile, with no acute respiratory distress (respiratory rate of 18 in min.) or unstable vital signs. A visual inspection showed a single diffuse swollen area of approximately 4 × 3 cm with ill-defined borders in the right cervical region. The overlying skin was the same color as the surrounding skin. Upon palpation, the mass was slightly tender, fluctuant, compressible, mobile, and showed signs of matting (Figure 1). However, her other lymph nodes were not palpable, her lungs were clear, and her cardiovascular examination was normal. Her markedly distended abdomen was notable for massive ascites with no signs of peritonitis. There was mild tenderness in the abdomen upon palpation. Moreover, there was no lower extremity swelling. The remainder of the exam was significant for an unhealed low laparotomy scar that was oozing a yellow - colored fluid. There were no stigmata of chronic liver disease or a hernia. She had mild anemia, with a hemoglobin level of 11 g/dl and a normal white blood cell count (7,300× 109/1) and her blood biochemical profile was normal. In addition, her viral hepatitis test and HIV profile were negative.

Figure 1
This patient’s chest radiographs did not indicate any pathology but her abdominal and thoracic ultrasound revealed massive ascites with mild septation without pleural effusion (Figure 2).
At the time of presentation, this patient was taking furosemide and spironolactone, which were prescribed by her GP. We stopped these medications and admitted the patient to the medical ward. A puncture of the cervical mass resulted in the aspiration of 15 ml of yellow turbid liquid with marked caseous necrosis. Laparocentesis revealed a yellow-color translucent fluid (Figure 3). The ascites fluid had a high protein content, low glucose level, and marked lymphocytes with a serum ascites albumin gradient (SAAG) lower than 1,1exluding portal hypertension Furthermore the ascites fluid adenosine deaminase (ADA) levels were markedly high (45 U/l; the normal limit is less than 36 U/l)
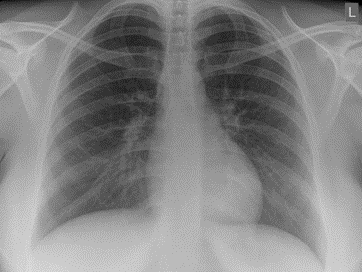
Figure 2

Figure 3
The histological examination of the peritoneal biopsy revealed numerous caseating epithelioid granulomas with multinucleated Langhans giant cells lymphocytes, and focal caseation. Special staining, such as the Ziehl-Neelsen stain, identified occasional pathological acid-fast bacillus organisms that were consistent with TB. Therefore, the ovarian malignancy diagnosis was excluded, and PTB with tuberculous lymphadenitis. The sputum were negative (GeneXpert; Cepheid, Sunnyvale, CA, USA), and patient was
prescribed the antituberculous treatment Rifafour (isoniazid, rifampicin, pyrazinamide, and ethambutol). Two days after the antituberculous treatment began, the general condition of this patient improved significantly, and she was discharged from the hospital 10 days after her admission to the medical ward. A careful retrospective evaluation of her respiratory system showed no indications of pulmonary TB. However, the later results of her ascitic fluid culture were positive for Mycobacterium tuberculosis. The mycobacterial culture of the lymph node aspirate showed negative results.
PTB can be acute or chronic, and traditionally, it has been divided into four types. The wet ascitic type is more common, and it is associated with a large amount of free or loculated fluid in abdomen. The ascitic fluid usually exhibits a high density due to the increased protein content of the inflammatory exudate. In addition, associated peritoneal enhancement is usually present. The dry, fixed, fibrotic type of PTB includes the involvement of the omentum and mesentery, and it is characterized by presence of matted bowel loops upon imaging. This type of PTB exhibits a fibrous peritoneal reaction, peritoneal nodules, and the presence of adhesions. Occasionally, loculated encysted ascites can be presented, which constitutes the third type of PTB be present, which constitutes the third type of PTB. Finally, the purulent and rare form of PTB usually develops secondary to tuberculous salpingitis, with the pockets adherent to the intestine and omentum containing TB pus (“cold” abscesses). However, a combination of these features is usually noted [4].
PTB exhibits a diverse and nonspecific symptomatology, and no single test is adequate for this diagnosis in all patients [5]. Liver cirrhosis, chronic ambulatory peritoneal dialysis, diabetes mellitus, and HIV are all risk factors for PTB. However, abdominal TB in a non-HIV patient is still a challenging diagnosis requiring a high index of clinical suspicion. In this particular case, the postpartum condition could have been a risk factor for the development of ETB, specifically PTB with scrofula [5, 6].
The extrapulmonary forms of TB constitute approximately one-sixth of all cases, and the prevalence of ETB seems to be rising, particularly due to the increasing prevalence of acquired immunodeficiency syndrome. The abdomen is involved in 12% of the patients with ETB, and gastrointestinal involvement is found in 66% to 75% of the abdominal cases, with the terminal ileum and ileocecal regions being the most common sites of involvement. This frequency is higher, and it could double or even triple, in HIV-positive subjects. EPT can affect all age groups, with a predilection for women between 20 and 50 years old [6]. The peritoneal transplantation of M. tuberculosis is haematogenous, and it is mainly transplanted from primary infections that often go unnoticed. More rarely, it can be transplanted after a first gastrointestinal infection. In other cases, the peritoneal infection represents seeding from the abdominal lymph nodes [7].
Clinically, PTB can mimic advanced ovarian cancer, with pelvic pain, abdominal distension, weight loss, and palpation of an abdominopelvic mass being present in both conditions. However, the search for and absence of other signs, such as menstrual disorders (55% of the cases) and infertility (5% to 10% of the cases), can be useful for the diagnosis of abdominal TB [8]. An association with other localizations, especially pulmonary, should be investigated, but its absence does not eliminate the diagnosis of PTB, as in our case. Several imaging techniques, such as ultrasonography and computed tomography, can sometimes guide the diagnosis. The existence of ascites with septas, peritoneal thickening, and heterogeneous enhancement are typical for inflammatory processes like TB. In addition, the CA125 level, which is an ovarian cancer biomarker of epithelial origin, can be high in several benign gynecological diseases (endometriosis, uterine fibroids, and pelvic inflammatory processes), extragynecological diseases (peritonitis, pancreatitis, hepatitis, nephrotic syndrome, and PTB), and nongynecological cancers with peritoneal metastases. In PTB cases, very high CA125 values (greater than 1,000 U/ml) can be seen [8]. Moreover, 90.1% of PTB patient have elevated plasma CA125 levels with a mean value of 565 U/ml [8]; therefore, CA125 has no place in the differential diagnosis between ovarian cancer and PTB. However, a decrease in the CA125 level has been correlated with the TB treatment response, and it has been indicated as a surveillance marker in antituberculous therapy [9, 10].
Ascites is a clinical condition that may represent the initial manifestation of a systemic disease or an otherwise unsuspected abdominal disease. In most cases, ascites appears as part of a well-recognized illness, for example, cirrhosis, congestive heart failure, nephrosis, or disseminated carcinomatosis. Occasionally, ascites may develop as an isolated finding in the absence of a clinically evident disease. In such cases, a careful analysis of the ascitic fluid may suggest the etiology [11]. For instance, a SAAG value of > or < 1>
In our case, the anatomopathological examination after the caseous granulation biopsy was sufficient to confirm the diagnosis. In addition, the search for mycobacteria using a polymerase chain reaction can be useful for the diagnosis, with a sensitivity of 75–80% and a specificity of 85–95%, but this technique is often unavailable. As in the case of our patient, surgical exploration is necessary in confirm or rule out the suspicion of a malignant ovarian tumor. The first route can consist of either a laparotomy or laparoscopy. However, transvaginal or transabdominal ultrasound-guided biopsies can be used in cases with a strong suspicion of TB, thus limiting postoperative complications [13]. The histological study of biopsies makes it possible to correct the diagnosis by showing gigantocellular granulomas with caseous necrosis specific for Koch’s bacillus. The treatment of PTB is essentially medical, and it is based on the daily administration of a quadritherapy combining isoniazid, rifampicin, ethambutol, and pyrazinamide for two months. Then, a four-month maintenance treatment is begun, using daily dual therapy combining isoniazid and rifampicin [14]. A surgical procedure is especially indicated in cases with a compressive or fistulised mass in order to flatten the caseous cavities.
Overall, PTB prevention is based on a Bacillus Calmette-Guérin vaccination, the detection of asymptomatic and atypical forms, chemoprophylaxis in the case of contact, and improvements in the hygiene of populations at risk [14].
Here we reported a case of postpartum PTB mimicking a malignant tumor. A 27-year-old woman who had a normal vaginal delivery six months previously presented to our department with ascites and an elevated serum CA125 level. PTB was diagnosed via a peritoneal biopsy. After undergoing treatment using the four-drug anti-TB regimen including isoniazid, rifampicin, ethambutol, and pyrazinamide, the patient recovered with the disappearance of ascites and a normal CA125 serum level after six months.
The clinical diagnosis of PTB should be considered in a relatively young female with nonspecific symptoms of abdominal distension, as well as lymphocytic ascites without malignant cells. Using a laparoscopy or a minilaparotomy to obtain tissue samples may be the most direct and least invasive approach for the diagnosis in order to avoid an unnecessary extended surgery.
Although the cytology and culture of ascitic puncture fluid can confirm the diagnosis confirm of PTB, in other cases, a laparoscopy or laparotomy with a biopsy is needed. In addition, the CA125tumor biomarker can be used to monitor activity in non-neoplastic ascitic states.
Key Points
•TB can spread from the lungs and lymph nodes through the bloodstream to many sites, including the abdomen, particularly the peritoneum.
•The TB symptoms depend on the affected organ, but they may be very atypical and nonspecific.
•CA125, an ovarian cancer biomarker, can be elevated in PTB cases.
•The diagnosis of PTB is based on the identification of M. tuberculosis in the infected fluid or a microscopic examination the peritoneal tissue and culture.
•A decrease in the CA125 level is correlated with the TB treatment response.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
