
Case Report | DOI: https://doi.org/10.31579/2690-8794/109
Bait Balev Nesher and The Ruth and Bruce Rappaport Faculty of Medicine, Technion, Israel Institute of Technology, Haifa, Israel.
*Corresponding Author: Jochanan Naschitz, Bait Balev Nesher and the Ruth and Bruce Rappaport Faculty of Medicine, Technion, Israel Institute of Technology, Haifa, Israel.
Citation: Jochanan E. Naschitz (2022) Perineal Ecthyma Gangrenosum, J, Clinical Medical Reviews and Reports. 4(2); DOI: 10.31579/2690-8794/109
Copyright: © 2022, Jochanan E. Naschitz, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 October 2021 | Accepted: 16 December 2021 | Published: 05 January 2022
Keywords: ecthyma gangrenosum, perineum, neutropenia, glyoblastoma, abemacilib, temozolomide
Perineal necrotic lesions have a narrow differential diagnosis, when ecthyma gangrenosum (EC) should be considered in priority. A 43-year old woman receiving immunotherapy for metastatic glioblastoma was admitted under clinical deterioration and severe neutropenia. Shortly after admission an erythematous eruption occurred involving the chest and perineum. Within a few hours the lesions evolved from erythema to necrosis. Broad spectrum antibiotics were started. Results of lesional cultures revealed Pseudomonas aeruginosa. The diagnosis of EC was established. A life threatening infection, EC needs to be quickly diagnosed, differentiated from other necrotizing eruptions, and treated in emergency.
Ecthyma Gangrenosum (EC) is classically described as a cutaneous manifestation of pseudomonas aeruginosa bacteremia. However, similar lesions are caused by other bacterial or fungal infections. Ecthyma gangrenosum usually occurs in patients who are critically ill and immunocompromised. Fever begins a few days before the appearance of the skin lesions. At onset EC presents a round or oval erythematous lesion 1 cm to 15 cm in diameter that. A hemorrhagic focus emerges in the central area and may progress to a bulla. The lesion spreads at the periphery and turns into a black necrotic ulcer with an erythematous rim. The transformation of an early lesion into a necrotic ulcer may take a few hours [1, 2]. EC may appear on the gluteal region, perineum, extremities, trunk, or face (1-4). EC requires prompt diagnosis and antibiotic treatment. When therapy is delayed, the mortality ranges from 18% to 62%. Perineal necrotic lesions have a narrow differential diagnosis and EC should be considered in priority.
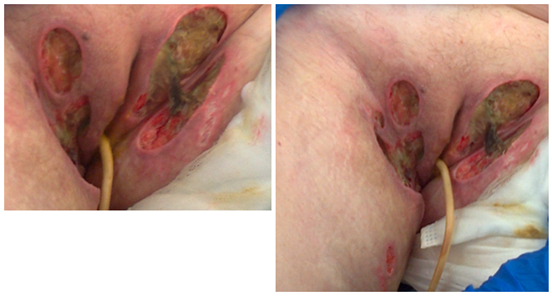
A 43-year-old woman was admitted to our ward for end-of- life palliative care. One year ago she was diagnosed with frontal glioblastoma. The tumor has been resected, followed by radiation therapy, and chemo and immune therapy. The portable Optune device was applied locally to create electric fields that disrupt cancer cell division. Lately, under a course of abemacilib and temozolomide she developed severe neutropenia and thrombocytopenia. The bodily temperature was normal. After discontinuation of these medications and repeated administration of granulocyte colony stimulating factor there was delay in recovery. Blood cultures were negative. At this time a necrotic skin ulcer was revealed on the patient's back and numerous similar lesions on her perineum. In urgency bacterial cultures from skin ulcers were taken and empirical treatment with piperacillin-tazobactam was started. A biopsy specimen from an ulcer's rim showed necrosis of the dermis, a neutrophilic infiltrate and numerous hyphae and spores. Cultures from the ulcer revealed growth of pseudomonas aeruginosa and candida species. In the following, a course of cephamezine was provided, the perineal ulcers were debrided and treated with topical gentamycin cream. The patient's vital signs returned to normal. The white blood cells increased to 5200/mm3 with 73% neutrophiles, platelets 87.00/mm3, hemoglobin 9.7 g/dL. At the time of her transfer to our institution she was in minimal consciousness state. She received enteral nutrition and a regimen including dexamethasone 12 mg, levetiracetam and pantoprazol. The skin lesions at this time, two weeks after their first occurrence, are shown in Figures 1 and 2. The oval lesion of the patient's back, covered by a black necrotic tissue, has characteristic features of EC. The ulcers on the patient's labia majors, perineum and upper thighs, of various sizes and dept, resulted from spontaneous or surgical debridement of the necrotic tissues. After an uneventful course in our department the patient developed high fever and hypotension. Broad spectrum antibiotic treatment was started, and she was referred to an acute care hospital. She died two days later.

The diagnosis of EC in this patient is straightforward. The patient was predisposed to infection in being deeply immune depressed, neutropenic, and was under high dose dexamethasone treatment. The lesion's swift evolution within a few hours from erythema to necrosis as well as their round or oval shape were suggestive of the diagnosis. Lastly, pseudomonas aeruginosa cultured in the lesion was consistent with the diagnosis. Unusual, but not exceptional in this case were the large number of the lesions in a close cluster confined to the perineum and thighs [3-5], along with one distant lesion on the chest wall. Also, ecthyma gangrenosum without bacteremia in this patient is not exceptionally rare [6, 7]. In the differential diagnosis of lesions resembling those of this patient's, genital herpes simplex and herpes zoster are pertinent. In the normal host, herpetic lesions may remain few and continue to form for only 3–5 days. The total duration of disease is generally 7–10 days; however, it may take as long as 2–4 weeks for the skin to return to normal. Herpes zoster is more severe in immunocompromised subjects and lesions continue to form longer than one week, and scabbing is not complete in most cases until 3 weeks into the illness. Unilateral vesicular lesions in a dermatomal pattern should lead rapidly to the diagnosis of herpes zoster and specific treatment should be started immediately. However, herpes simplex virus can also cause dermatomal vesicular lesions [8]. A clinical clue, which could possibly help in differentiating between herpes zoster and zosteriform herpes simplex is that vesicles of herpes simplex are uniform within a cluster while the vesicles of herpes zoster vary in size [9, 10]. Necrotizing fasciitis is a potentially fatal soft tissue infection that may affect the upper and lower extremities, scrotum, perineum and abdominal wall, rapidly spreading along the fascial planes [11]. All the above-described feature differ from the patient's single-day eruption, not dermatomal distribution, deep subcutis necrosis, large size of individual lesions. In addition, a cutaneous adverse reaction to medications should be considered. A variety of cutaneous adverse effect to abemacilib have been described but none resemble the lesions of this patient [12].
Suspicion of EC should prompt initiation of empiric broad-spectrum antibiotic therapy that includes coverage for P. aeruginosa. The recommended treatment for both bacteremic and nonbacteremic EC is an antibiotic that is effective against Pseudomonas species, such as cefepime, a carbapenem (imipenem/cilastatin, meropenem, or doripenem), or piperacillin-tazobactam. The proposito received a treatment with piperacillin-tazobactam followed by cefepime, a fourth-generation cephalosporin antibiotic [13].
A life threatening infection, EC needs to be quickly diagnosed, differentiated from other necrotizing eruptions, and treated in emergency. The present case is typical regarding the clinical context and exceptional by the multitude and severity of skin lesions.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
