
Research Article | DOI: https://doi.org/10.31579/2641-0419/128
*Corresponding Author: A.J.J. IJsselmuiden, Department of Cardiology, Amphia Hospital Mailbox 90158 4800 RK Breda the Netherlands.
Citation: Zwaan EM, Cheung ES, Simsek C, Kofflard MJM, Holtzer CAJ, Schölzel B, Meuwissen M, IJsselmuiden AJJ. (2021) Performance Analysis of a Novel Hydrophilic-Coated Transradial Guiding Catheter. J. Clinical Cardiology and Cardiovascular Interventions, 4(4); Doi:10.31579/2641-0419/128
Copyright: © 2021 A.J.J. IJsselmuiden, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 12 January 2021 | Accepted: 28 January 2021 | Published: 18 February 2021
Keywords: catheterization; complication; coronary disease; hydrophilic-coated guiding catheter; TR-PCI
Aim: The transradial approach (TRA) has taken an upswing, however access-site complications still exist. The choice of potentially less traumatic materials may minimize these complications. This article describes the use of a hydrophilic-coated 6F guiding catheter for diagnostic and interventional procedures and upper extremity dysfunction following these procedures.
Materials and Methods: This prospective observational study enrolled 217 patients who underwent elective transradial percutaneous coronary intervention (TR-PCI) for stable and unstable angina, or acute coronary syndrome between May 2014 and November 2016. All patients were treated using a 6F hydrophilic-coated guiding catheter (PRIMUM, PendraCare, Wellinq, the Netherlands). Catheter performance was assessed on a five-point scale ranging from very bad to very good. Procedure safety was assessed using the Major cardiac and cerebrovascular events (MACCE) criteria.
Results: The average number of guiding catheters used was 1.2 per patient. Overall performance of the catheters was rated Average/Good. Procedural success, defined as TIMI grade 3 flow and successful stent deployment, with a residual diameter stenosis of <25%, was 97.7%. MACCE occurred in 1.5% during the 6-months of follow-up.
Conclusion: These data indicate that the use of a hydrophilic-coated guiding catheter to perform percutaneous coronary interventions is safe and effective, with high procedural success and low complication rates. In addition, the short and long-term MACCE outcomes of the PCI were favorable.
Running title: Guiding Catheter Performance
ACC/AHA : American College of Cardiology/American Heart
Association classification
CAG : Coronary artery angiography
MACCE : Major adverse cardiac and cerebrovascular events
NRSP : Numeric Rating Scale for Pain
NSTEMI : Non ST-elevation myocardial infarction
PCI : Percutaneous coronary intervention
RAO : Radial artery occlusion
RAS : Radial artery stenosis
STEMI : ST-elevation myocardial infarction
TIMI : Thrombolysis in myocardial infarction
TRA :Transradial approach
TR-PCI :Transradial percutaneous coronary intervention
6F :6 French
Throughout the years, transradial approach (TRA) has become the standard access site during coronary interventions. The major factors contributing to this are the occurrence of less vascular site complications, enhanced patient comfort, less hospital days and therefore reduced cost [1,2]. Nevertheless, TRA is still associated with certain complications such as local access bleeding, radial/brachial artery spasm and forearm hematoma, which may result in upper extremity dysfunction [3-5]. The usage ofhydrophilic-coated guiding catheters provide smooth catheter introduction with low friction during advancement, even in tortuous or calcified vessels. The hydrophilic coating reduces vessel spasm and is expected to be less traumatic to the vessel wall. [6-8] Moreover, hydrophilic guiding catheters are less trombogenic than their non-hydrophilic counterparts. [9] A performance analysis of a 6 French (6F) hydrophilic-coated guiding catheter (PRIMUM, PendraCare, Wellinq, the Netherlands) was done in a subset of patients included in the ARCUS registry (Effects of transradial percutaneous coronary intervention on upper extremity function). [3] The aim of the study was to assess whether the usage of hydrophilic coated guiding catheters is safe and effective, and whether it could lead to favorable outcomes with TRA.
Materials and methods
Between May 2014 and November 2016, five interventional cardiologists kept record of the guiding catheter performance during transradial procedures. All patients enrolled in this registry were included in the ARCUS (Effects of trAnsRadial perCUtaneouS coronary intervention on upper extremity function), a study performed in a high-volume secondary referral center in the Netherlands. [3] For the ARCUS study, a total sample size of 400 transradial and 100 transfemoral patients was chosen, based on an expected upper extremity dysfunction rate of 30%. [3] Patients were included in the ARCUS study, if they had a palpable radial artery, and if Doppler ultrasound examination confirmed a non-occluded flow. Procedures using the contralateral radial artery or femoral artery after previous unsuccessful attempts were also included in this study. Exclusion criteria were 1) absence of informed consent 2) an occluded flow of the radial artery objectified by Doppler ultrasound 3) incapability to accomplish measurements due to comorbidities and 4) illiteracy. [3] For this sub-study, only patients treated with transradial PCI (TR-PCI) between May 2014 and November 2016 were included and patients were excluded from this analysis if they had a crossover procedure to the contralateral or femoral approach due to failure of the TRA or if there was no complete record of the hydrophilic-coated guiding catheter performance.
Guiding Catheter design
The hydrophilic-coated segment of the PRIMUM-catheter is approximately 7 cm proximal from the tip until 25 cm distal from the hub. [10] To facilitate optimal alignment and backup support the segment in the tip is uncoated. The proximal 25 cm of the catheter that stays outside the body is uncoated to ease manipulation, while the uncoated catheter segment in the valve of the sheath is designed to prevent unintentional movement of the catheter during the procedure. Hydrophilic coating provides no “stick-slip” effect, allowing more accurate and precise tip positioning in ostial lesions, and a 1:1 torque control of the tip. While the outer diameter is downsized compared to a 7 French catheter, the catheter’s large inner lumen (0.071”) allows good contrast injection even while performing the kissing balloon technique, and offers expanded device compatibility for larger profile devices. [10] The catheter has a small a-traumatic soft tip to minimize vessel damage.
Percutaneous Coronary Interventions
A hydrophilic-coated 6F sheath introducer (Glidesheath slender, Terumo Medical Corporation, Tokyo, Japan) [10], was attempted in all patients undergoing TR-PCI. [3] A 0.014-inch coronary guidewire was used to cross target lesions and contrast was injected manually in all cases. Non-patent hemostasis of the radial artery was achieved by using a compression device (Terumo Medical Corporation, Tokyo, Japan).
The primary endpoint of this registry was procedural success, defined as thrombolysis in myocardial infarction (TIMI) coronary flow grade 3, and successful stent deployment, with an angiographic visual estimated final residual diameter stenosis of <25%. [11] Secondary endpoints were guiding catheter safety (rate of catheter-related complications).
Guiding catheter performance characteristics
Guiding catheter insertion, torque control, opacification of the vessel, tip and catheter radiopacity, back-up support, and persistent catheter stiffness was rated by experienced operators on a five-point scale (1: Very Bad; 2: Bad; 3: Average; 4: Good; 5: Very Good). Furthermore, friction in and outside the sheath, the occurrence of kinking, the need for a guide liner or for deep intubation, vessel damage, guiding cannulation failure, and defective catheter were recorded. Back-up support was defined as the ability to advance a guiding catheter in coronary vessels conveniently, represented by the efficacy of transfer or the proximally applied push force to the catheter tip.
Torqueability was defined as the capacity of a guiding catheter to tolerate torque between the proximal hub and the tip without kinking or other irreversible damage to the system. Friction was defined as a contact force accumulated when two surfaces (i.e. sheath vs. guiding catheter or guiding catheter vs. vessel wall) interact and which can affect advancement/movement of the catheter tip (e.g. resistance).
Kinking of the catheter was defined as a visually observed in vivo indentation of one side of the catheter wall touching the opposite side of the catheter wall with a sharp curvature. Catheter stiffness was defined as the force needed to bend the wire. Overall guiding catheter performance was scored on a five-point scale by the operators.
Catheter induced pain and spasm
Procedural pain was assessed using the validated Numeric Rating Scale for Pain (NPRS). [12] Procedural radial artery spasm was also evaluated. Moderate spasm was defined as some resistance perceived by the operator, while the catheter still is effectively maneuverable, and distinct painful perception for the patient. Severe spasm was defined as catheter not steerable or retractable, with severe pain for the patient when the catheter was being manipulated.
Access-site complications
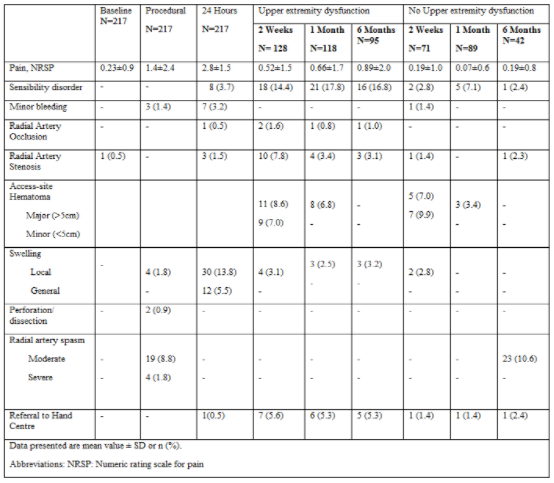
Access-site complications were noted during the procedure and clinical outpatient visits (after two weeks, one month and six months of follow-up) and when necessary patients were referred to a hand specialist. [3] Swelling, access-site bleeding, hematomas and their proportions were assessed. Furthermore, upper extremity function as a composite endpoint consisting of (isometric) strength, sensibility of all digits, and circumference measurements was also assessed.
Measures of long-term clinical outcome
All patients were interviewed personally and examined at their outpatient clinical visit up to approximately six months after their catheterization, to assess the long-term TR-PCI treatment outcomes and also specifically the complications involving the hand intervention. Long-clinical outcomes were measured in terms of Major adverse cardiac and cerebrovascular events (MACCE) defined as myocardial infarction, according to the Third Universal definition of Myocardial Infarction, target vessel revascularization, either by percutaneous coronary intervention (PCI) or coronary artery bypass grafting, death from any cause or a cerebrovascular accident. [13]
Descriptive statistics were provided for all variables considered in the analysis. For categorical variables, the data was presented as percentages. Continuous variables with normal distribution were presented using means and standard deviation (SD), non-normally distributed variables were presented using median and interquartile (IQR)-range. Between-group differences of dichotomous/ordinal variables were analyzed using Chi-square test with Yates continuity correction or for trend, respectively. Comparisons of continuous variables for more than two groups were analyzed using the Kruskal Wallis test. Statistical tests were carried out two-tailed at the 5% level of significance. Statistical analyses were performed with SPSS for Mac version 26.
A total of 234 patients treated with TR-PCI were included in the ARCUS study between May 2014 and November 2016. Seventeen (7.2%) patients were excluded from this registry because of crossover to the femoral or contralateral radial artery. In all these patients access to the radial artery was unsuccessful and crossover was not related to the performance of the guiding catheter.
The demographic and baseline characteristics of the total patient population (N =217) in this registry are presented in Table 1.
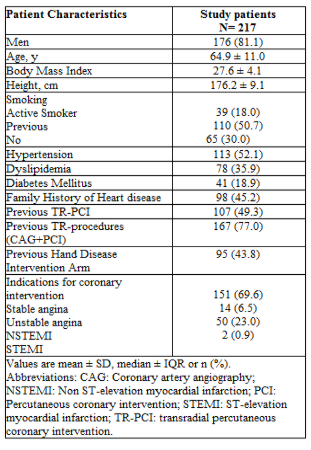
The mean age was 64.9 ± 11 years and 176 patients (81.1%) were male. Procedural characteristics and PCI complexity are summarized in Table 2.
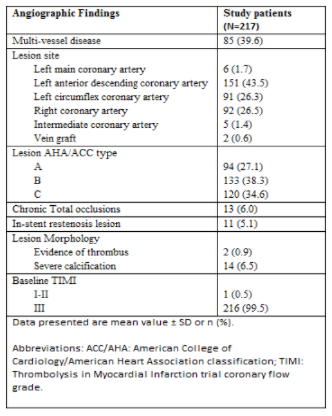
Among the 217 included patients, 116 patients underwent treatment of a single lesion, 76 patients had two lesions, 22 patients had three lesions, two patients had four lesions, and one patient had five lesions treated. The procedural characteristics and outcomes are listed in Table 3.
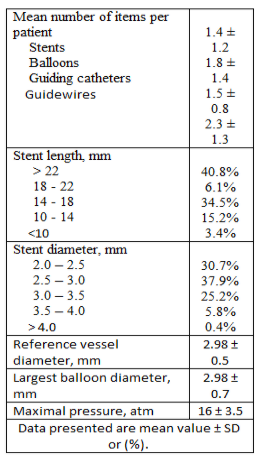
The average number of guiding catheters was 1.2 per patient. During 176 procedures, one type of guiding catheter shape was used. In respectively 35, five and one procedure there were two, three or four different catheter shapes used. Procedure success rate was 97.7%. Guiding cannulation failure resulted in procedural failure in five (2.3%) patients, in which nine guiding catheters in total were used. The reasons of guiding cannulation failure were wrong sizing (N=1) and severe calcifications, such as chronic total occlusions, whereupon the guiding catheter could not be advanced (N=4).
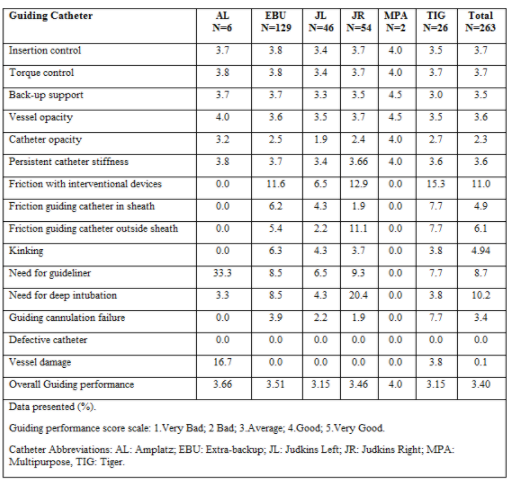
The guiding catheter performance as was reported by an opinion survey among the operators is listed in Table 4. The handling of the PRIMUM guiding catheter was rated Good-Average as it enhances good insertion control, exhibits good torque response, and effective back-up support, enabling adequate wiring, minimal guiding switches and sufficient equipment delivery. Operators considered the vessel visualization good, however, the visualization of the catheter tip was rated Bad-Average, although manageable by using a gentle puff of contrast, without affecting the procedure or its outcome.
The lowest scores was Average for the performance of the Judkins Left and Tiger (TIG) guiding catheter (Table 4).Friction during passage of the stent through the guiding catheter was reported in 4.9%, while friction outside the sheath was reported in 6.1% (Table 4).
Procedural complications
Dissection occurred in two patients during balloon dilatation. Both were adequately treated with stents (Table 4). Radial artery spasm was reported in 23 patients (10.6%), ranging from moderate spasm (N=19, 8.8%) to severe spasm (N= 4, 1.9%). All spasms were alleviated during the procedure and there was no patient injury reported (Table 5).
Chi-square test for trend indicated there was only a significant difference in spasms between gender groups, in favor of male patients, c2(2) =7.54, p=0.023. A Kruskal-Wallis Test revealed no statistically difference in body mass index across the three spasm severities (no spasm, N=192, moderate spasm, N= 19, severe spasm, N=4), c2 (2,N=215)=2.85, p=0.240.
MACCE during follow-up
Major events during follow-up were scarce, with a mean follow-up period
of 182 ±36 days. At two weeks after the procedure one patient, who presented with progressive angina, had a revascularization by means of PCI.
Furthermore, one patient had a successful resuscitation after a ST-elevation myocardial infarction (STEMI) followed by a coronary angiography, but there were no signs of stent thrombosis or significant coronary stenosis. One month after the procedure one patient underwent a PCI due to stent thrombosis. One patient required a semi-urgent coronary artery bypass grafting at six months due to stent thrombosis. No cerebral complications occurred during the study.
Post-procedural Access-site complications
The access-site complications and hand dysfunction are presented in Table 5. Noteworthy are the radial artery occlusions, which recanalized in 50%. Of this cohort 22 patients were referred to a hand rehabilitation specialist during the 6-month follow-up period.
This article presents to the best of our knowledge the first prospective registry regarding the performance and procedural results of a hydrophilic-coated guiding catheter in TR-PCI. This article is also the first comprehensive evaluation regarding access-site complications post TR-PCI using a novel hydrophilic-coated guiding catheter.
Theoretical advantage of the PRIMUM configuration is the catheter introduction with less friction during advancement due to the hydrophilic coating. With regard to improving catheter tip visualization new developments are ongoing.
This study reports the overall performance and safety of the catheter up to six months of follow-up. There have been concerns regarding long-term safety of hydrophilic-coated guiding catheters regarding distal embolic events. [14-16] However, these studies only provide low-level evidence and evidence from large-scale human trials are lacking.
Guiding catheter related dissection in TR-PCI was reported in 0.9%, compared to 2.2% in similar studies using an uncoated catheter. [17] Hydrophilic coatings on introducer sheaths reduce rates of radial spasms. [18] A hydrophilic coating on guiding catheters may contribute to reduce this rate even further. Radial artery spasm has been reported to be responsible for up to 38% of all transradial procedure failures. [19] In our study, spasm in the radial artery was reported as “Moderate” in 8.8%, and only “Severe” in 1.8%, which is far better in comparison with the moderate to severe spasm rate of 19% when using only 6F hydrophilic-coated sheaths. [17] Additionally, current rates are comparable with previously reported symptomatic radial artery spasm of 0.7% while using the sheathless Eaucath hydrophilic-coated 6F guiding catheter. [1] Procedural failure in our cohort was not attributed to spasm.
Upper extremity function assessment showed high rates of dysfunction as it is a very sensitive composite endpoint. [5] Upper extremity function following TR-PCI has never been examined, as thoroughly as in our study, therefore we cannot compare our outcomes with the existing literaturse. Although we did not compare the hydrophilic-coated catheter to an uncoated catheter, hydrophilic coating might limit upper extremity dysfunction following TR-PCI. Future research is needed and should focus on comparing hydrophilic vs. uncoated catheters in relation to upper extremity function in order to optimize TR-PCI and minimize access-site related complications. We believe that the current report can be used as a tool for comparison with other novel guiding catheters (e.g. Railway Cordis Sheathless).
Procedural complications and long-term clinical outcomes were similar to previous studies. [19] Overall, the patient characteristics of our cohort, with amongst others 73% B/C lesions, were comparable to the general population. These results may therefore also be applicable to a general patient population undergoing TR-PCI.
This registry was a prospective multicenter non-randomized registry. Patients were selected from the ARCUS trial when operators had completely filled out the catheter performance survey and procedural data was complete, which might cause selection bias, as this was not randomly achieved. Nevertheless, the data on upper extremity dysfunction represent objective measurements and reflect a higher level of evidence. The main limitation of this study is that there was no comparison with other, uncoated 6F guiding catheters or with sheathless interventions. A conclusion on the effect of hydrophilic coatings on upper extremity function could therefore not be drawn and should be a focus point for future research. Randomized studies are warranted.
In conclusion, this registry indicates the 6F PRIMUM guiding catheter to show high eligibility for use in TR-PCI. Use of the hydrophilic-coated PRIMUM catheter as a default system in routine TR-PCI was both feasible and safe, associated with high procedural success and a low complication rate. In addition, it showed favorable short and long-term MACCE outcomes. This report could serve as a tool for comparing the performance of different (novel) guiding catheters in the future.
Conflict of Interest:
The authors have no financial relationships or conflicts of interest to disclose regarding the contents of this article
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
