
Case Report | DOI: https://doi.org/10.31579/2690-4861/418
1Cardiac Surgery Division, Tor Vergata University Hospital, Rome, PC 00133, Italy.
2Cardiology Unit of the Cardiac Surgery Division, Tor Vergata University Hospital, Rome, PC 00133, Italy.
*Corresponding Author: Dario Buioni, Cardiac Surgery Division, Tor Vergata University Hospital, Viale Oxford 81, Rome, PC 00133, Italy.
Citation: Cristina Viscogliesi, Dario Buioni, Paolo Nardi, Calogera Pisano, Eleonora Latini et al., (2024), Perforation of Left Ventricular wall and Ipsilateral Pleura by a Right Ventricular Pacemaker lead: Case Report, International Journal of Clinical Case Reports and Reviews, 17(1); DOI:10.31579/2690-4861/418
Copyright: © 2024, Dario Buioni. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 12 February 2024 | Accepted: 27 March 2024 | Published: 11 April 2024
Keywords: pacemaker; right ventricular pacemaker lead; lead migration; left ventricular perforation; transvenous lead extraction; pneumothorax; pericardial effusion
Introduction: Malposition of pacemaker lead is uncommon event and it usually regard the right ventricle. In rare cases, the perforation can involve the left ventricle and this is a potentially life-threatening complication.
Case presentation: We described a case of both septum and LV free wall perforation by an RV pacemaker lead in an 84-year-old woman. Perforation also resulted in left pneumothorax and she became symptomatic. She also had pericardial effusion, so she underwent cardiac surgery to repair the bleeding lesion. As the swab for Covid-Sars 2 was positive, we had to wait for the negativization for the replacement of the ventricular lead.
Conclusions: early identification is mandatory to prevent this complication and transvenous lead extraction with cardiac surgery backup should be considered.
Published event rates of pacemaker lead perforation range from 0,1 to 0,8%. It includes acute, subacute and late perforation but subclinical lead perforation occurs more frequently. [1] Cardiac perforation is uncommon complication of transvenous pacemaker implantation and it usually regard the right ventricular apex due to the thin wall [2] Malposition in the left ventricular is an uncommon event and its incidence could be underestimated because the patient remains asymptomatic. The diagnosis can derive from the 12-lead ECG, the chest radiographs and from the computed tomography (CT). CT scan is considered the gold standard for evaluating for perforation [3]. It is used to confirm pericardial or pleural effusion and lead position or displacement [2].
An 84-year-old woman with a dual-chamber pacemaker implanted via the left cephalic vein for second degree atrioventricular block 2:1 (Mobitz 1). The day after the implantation, the chest x-ray showed dislocation of the lead and it was implanted the same day. In the hours following the implantation, the patient complained chest pain modifiable with the acts of the breath. Chest CT scan documented share of left PNX predominantly anterior with a maximum thickness of about 15 mm and minimal pericardial effusion of 1 cm. The day after a CT scan was performed to check the pnx. The flap was greater and the CT showed the ventricular catheter beyond the wall of the ventricle for about 5 mm, close to the pericardium and the pulmonary pleura. She therefore performed PMK check which showed increased right ventricle lead impedance and unipolar capture; increased ventricular threshold in bipolar. Before the transfer to our cardiac surgery room, the patient tested positive for Sars-Cov 2.
During the intervention, after the sternotomy, an important quantity of frankly blood liquid was aspirated and the clot on the anterior wall of the ventricle was removed. The electrod-catheter was 5 mm out of the left ventricle, about half a centimeter from the course of the anterior descending artery. Repair was carried out with a U point in polypropylene 4-0 reinforced with double pledgets and application of pericardium patches with Coseal glue and Tabotamp. The left pleura was opened to drain the pnx.
After surgery, she underwent cardiac CT (Figure. 1) which showed the tip of the ventricular lead projecting outwardly passing the antero-septal wall at the apical level and coming into close contact with the parietal pericardium at that level.
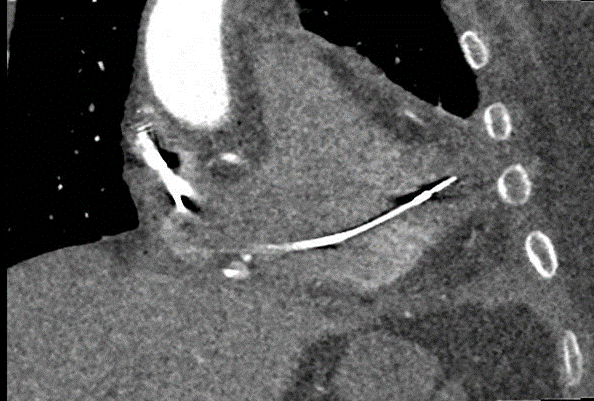
Figure 1: Therefore, after 20 days from the first, she was subjected to an operation of PMK repositioning under general anesthesia with transesophageal ultrasound monitoring.
Cardiac pacemaker devices are used for cardiac conduction abnormalities and arrhythmias. The complication derived from them, can be divided into three categories: acute within 24 hours, subacute if within one month, chronic after one month. The most common complication included pneumothorax, lead malposition and myocardial perforation. [2]
Pacemaker lead perforation is often attributed to one or a combination of factors including patient characteristics, concomitant therapies such as steroids or anticoagulants, implant techniques and the designed characteristics of the lead.
Anyway, anatomic variations largely account for lead misplacement into LV during the implantation of a cardiac device. The most common route is the interatrial septum and PFO. Possible complication of malposition of the lead into the left ventricular wall is the formation of thrombi around the site of lead placement, with subsequent risk of systemic thromboembolic events (more than one-third of cases).
This event occurs when the diagnosis is delayed. The patients who remain asymptomatic may opt for anticoagulation with warfarin with targeting international normalized ratio between 2,5 and 3,5. If cerebral embolic events occur, catheter surgical extraction should be reconsidered. [4]
The therapeutic options for a misplaced lead are limited and they depend on the symptomatology of the patients, on the time elapsed from implantation and on the bleeding risk of the patient. Adequate lifelong anticoagulation with warfarin is the therapy of choice if the lead has been placed for a long time. Lead extraction should be reserved for failure of anticoagulation or during other concomitant cardiac surgery. [5] Otherwise, if misplacement is diagnosed early after implantation, that is less than one year, with or without any associated thromboembolic episode it should be percutaneously removed and repositioned. [6]
In this report, we demonstrated that such a complication could become a life-threatening complication. The patient should undergo a sternotomy due to pericardial effusion complicated by cardiac tamponade.
As shown by the retrospective study on 26 patients made by Marius Schwerg et al., pericardial effusion and tamponade were present in 38% and 19%, respectively. [7] Therefore this complication si not so rare and in case of unclear results, thoracic CT scans are essential to determine if the pleural or LV free wall is implicated and to establish an appropriate diagnosis. [8]
The American Heart Association suggests that transvenous lead extraction is not the preferred strategy for patients with cardiac perforation due to pacing/defibrillation lead. [8] But our patent was symptomatic for pneumothorax and she had pericardial effusion, so we were forced to do a sternotomy. Once resolved the Sars-Cov 2 infection, we proceeded to lead extraction and replacement of the same catheter in a hybrid operating room, under careful hemodynamic and transesophageal echocardiographic monitoring with a cardiac surgical backup.
No specific recommendations are known to exist for this uncommon complication, but in this case, there were signs and symptoms that suggest the diagnosis. To assess whether the pleural or LV free wall is involved, x-Ray is not enough. CT scan is essential to not delay the diagnosis. This patient was hemodynamically instable and she hard to undergo a sternotomy. Maybe if the hospital where she implanted the pacemaker, had requested the CT scan first, we would have been able to arrange the hybrid operating room to proceed to lead extraction, avoiding the sternotomy, the delayed of replacement of PMK and one month of recovery.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
