
Case Report | DOI: https://doi.org/10.31579/2641-0419/267
1 Department of Cardiovascular Disease, Infirmary Health Thomas Hospital. Fairhope, AL
2 Department of Cardiovascular Disease, Cleveland Clinic Florida. Weston, FL
*Corresponding Author: Antonio Lewis Camargo, MD Department of Cardiovascular Medicine Cleveland Clinic Florida Weston, Florida 33331.
Citation: Odigwe Celestine I, Etuk Aniekeme S, Antonio Lewis, Alejandro Sanchez, Jacob Mina A (2022). Percutaneous Right Atrial Thrombectomy Using Flow Triever (Inari) and En Snare Endovascular System : A Safe Alternative to Surgical Approach - Report of Two Cases. J. Clinical Cardiology and Cardiovascular Interventions, 5(6); Doi:10.31579/2641-0419/267
Copyright: © 2022 Antonio Lewis Camargo, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 28 April 2022 | Accepted: 05 May 2022 | Published: 13 May 2022
Keywords: right atrial thrombus; percutaneous thrombectomy; en snare endovascular system; inari flow triever 24 suction catheter
Surgical thrombectomy is considered the gold standard approach for removal of thrombotic disease within the right heart (RiTH), however some patients have prohibitive surgical risk and the percutaneous approach has been increasingly popular in the past few years. In this manuscript, we present two case reports of patients with both acute and chronic right atrial thrombi; in whom elevated surgical risk deemed them not surgical candidates and both successfully underwent mechanical thrombectomy with Flow Triever suction catheter and En snare endovascular system. To our knowledge, these are the first reported cases of the use of both of these devices for treatment of RiTH.
CT : Computed tomography
CTA : Computed tomography angiogram
DVT : Deep venous thrombosis
IVC : Inferior vena cava
TEE : Transesophageal echocardiogram
Right heart thrombus (RiHT) are complex structures composed of clotted blood products, fibrin meshwork and cellular components located within the right atrium. These commonly occur in patients with mechanical heart valves, ventricular or atrial septal closure devices, arrhythmias, indwelling central venous catheters, right-sided pacemaker leads or sequela of pulmonary embolism [1]. The incidence of RiHT is unclear; however, it occurs in about 10% of cases when associated with pulmonary thromboembolism [1,2]. Surgical thrombectomy has been considered the goal standard management modality for RiHT; though percutaneous embolectomy is an alternative treatment, but limited data support this approach [3]. We present a case series of 2 patients who successfully underwent right atrial thrombectomy using an Inari FlowTriever 24 suction catheter and En Snare endovascular snare system under transesophageal echocardiogram and fluoroscopy guidance.
Patient 1:
A 42-year-old female with a past medical history of end-stage renal disease on hemodialysis, type 2 diabetes mellitus, pulmonary embolism, and deep venous thrombosis presented with complaints of generalized abdominal pain and distension of 1-week duration. Abdominal pain was associated with nausea, vomiting, and diarrhea. On physical examination, blood pressure was 171/80 mmHg, pulse rate of 82 beats per minute, afebrile with a temperate of 98.5-degree Fahrenheit. She had a dialysis catheter in her right upper chest wall.
Abdomino-pelvic contrast computed tomography scan revealed ascites, with fluid analysis in keeping with cardiac origin. The patient had a transthoracic echocardiogram (TTE) to evaluate cardiac function, which revealed moderate concentric left ventricular hypertrophy, an ejection fraction of 60-65% and findings consistent with a right atrial thrombus/mass of 18 x 9 mm in size (Figure 1). This was confirmed using transesophageal echocardiography (TEE) (Video 1).
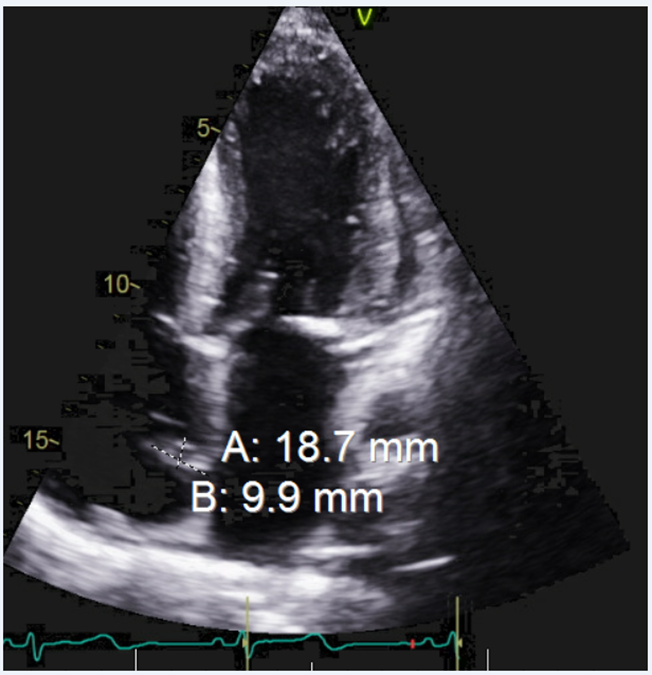
This was confirmed using transesophageal echocardiography (TEE) (Video 1).
The mass was initially believed to be attached to the dialysis catheter, however it was later found to be attached to the right atrial wall at the junction of the superior vena cava (Video 2) following the removal of the dialysis catheter. Due to her multiple co-morbidities, she was considered to be high risk for surgical thrombectomy.

After a multidisciplinary team discussion, the decision was made to proceed with percutaneous mechanical thrombectomy using a new technique involving both Inari Flow Triever 24 suction catheter and the En Snare endovascular system under TEE and fluoroscopy guidance. The En Snare was used to detach the mass from the atrial wall, while the Inari Flow Triever 24 suction catheter was used for extraction (Video 3).
Macroscopic analysis following removal had findings consistent with chronic thrombus with fibrotic changes (Figure 2), this was later confirmed with pathology. Repeat TEE showed complete resolution of RiHT (Video 4).

Patient 2:
An 89-year-old male with a medical history of hypertension and diabetes mellitus presented with complaints of deterioration of functional class of a day’s duration and was unable to speak in full sentences due to respiratory distress. On physical examination, the patient was tachycardic with a pulse of 114 beats per minute, tachypneic with a respiratory rate of 25 breaths per minute, normotensive with a blood pressure of 110/77 mmHg and afebrile with a temperature of 98.1 F. The left lower extremity looked edematous compared to the right.
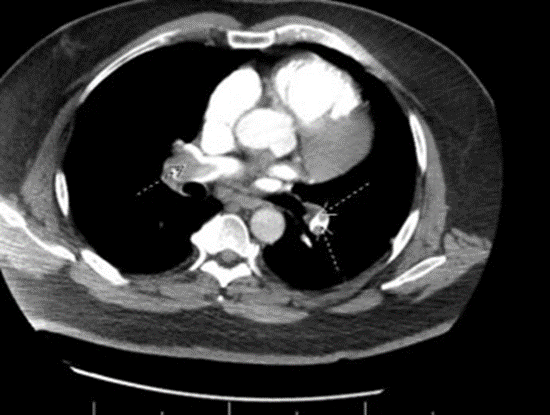
A computed tomography angiogram (CTA) of the chest was obtained revealing bilateral pulmonary thromboembolic disease (Figure 3) (PE). TTE noted a flattened interventricular septum consistent with right ventricular pressure overload and severely dilated right atrial cavity with a large mobile mass (Video 5).
Lower extremity doppler ultrasound was positive for a left Deep venous thrombosis (DVT) extending from the left common femoral to the soleus veins. Heparin infusion was initiated for therapeutic anticoagulation. Due to the presence of right heart strain and no signs of shock in keeping with the diagnosis of submassive PE, thrombectomy was considered, however the patient was deemed not a surgical candidate due to age. The decision was made to attempt clot removal with a percutaneous technique given the prior success with patient #1. Again, via TEE and fluoroscopic guidance, the transvenous approach using both Inari Flow Triever 24 and En Snare was used. Post-procedure transesophageal echocardiogram showed complete resolution of the right atrial mass (Video 6).
The patient also underwent an Inferior vena cava (IVC) filter placement and a mechanical thrombectomy for the left lower extremity DVT with good results. Acute thrombi (Figure 4) was confirmed via pathological analysis and the patient was discharged on oral anticoagulation in stable condition a few days later.

Right atrial masses are common incidental findings on echocardiography. A list of differential diagnoses includes atrial myxoma, vegetations from infective endocarditis, metastatic malignancies, and thrombi, with right atrial thrombi being the commonest [4]. Right atrial thrombi formation can be precipitated in the presence of foreign bodies such as central venous access extending into the right atrium. The morphology and mobility potential of right atrial thrombi have been grouped into various types; A, B, and C [2]. The management involves evacuating the thrombus either surgically or with newer techniques involving percutaneous catheter-assisted thrombectomy. We have presented two
cases where right atrial thrombus of varying etiologies were successfully managed via percutaneous catheter-assisted thrombectomy with Inari flow catheter and En Snare endovascular system. In our first case, the thrombus was chronic, and was associated with the presence of a dialysis catheter in the right atrium. This is the first reported case where the Inari Flow Triever 24 suction catheter was used alongside the En Snare endovascular system for removal of a chronic thrombus. However, in our second patient, the thrombus was acute coexisting with pulmonary embolism.
Percutaneous thrombectomy is a minimally invasive approach for treating right atrial thrombus. It is associated with reduced blood loss, infection risk, and improved patient recovery time compared with surgical thrombectomy. A review article in 2011 was conducted to assess the advantages of percutaneous mechanical thrombectomy and findings showed that percutaneous mechanical thrombectomy had a lower rate of complications with high technical success rate [5].
There is sparse literature supporting the use of Inari flow catheter for right atrial thrombi removal. A case was reported in 2019 where a patient developed right atrial thrombi following total hip replacement and was managed with a similar approach [6]. Also, a case series in 2020 described the successful evacuation of right atrial thrombi using the Inari flow catheter in three patients with acute thrombi [3]. Our case series describes the successful mechanical thrombectomy using the Inari FlowTriever for both acute and chronic right atrial thrombi removal, along with En Snare endovascular snare system.
Percutaneous thrombectomy is a great alternative to the surgical approach, especially in patients who are at high risk for surgery. Considering the associated benefit of a minimally invasive approach for right atrial thrombi removal as well as reported cases of this procedure done successfully with the Inari flow catheter and the En snare endovascular system, a randomized control trial has become imperative for this novel technique to become standard of care.
None.
None.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
