
Case Report | DOI: https://doi.org/10.31579/2641-0419/190
1* Senior Consultant & Coordinator, Department of Clinical & Interventional Cardiology, Evercare Hospitals Dhaka, Bangladesh.
2 Senior Registrar, Department of Clinical & Interventional Cardiology, Evercare Hospitals Dhaka, Bangladesh.
3 Registrar, Department of Clinical & Interventional Cardiology, Evercare Hospitals Dhaka, Bangladesh
*Corresponding Author: A Q M Reza, Senior Consultant, Department of Clinical & Interventional Cardiology, Evercare Hospitals Dhaka, Bangladesh.
Citation: A.Q.M Reza, Atique Bin Siddique, Poppy Bala, Mohammad Ziaur Rahman, Mahmood Hasan Khan, (2021) Percutaneous Intervention in Acute Renal Attack. J. Clinical Cardiology and Cardiovascular Interventions, 4(13); Doi:10.31579/2641-0419/190
Copyright: © 2021 A Q M Reza, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 30 June 2021 | Accepted: 12 July 2021 | Published: 16 July 2021
Keywords: renal infarction; renal artery thrombosis; renal impairment
A young patient with renal infarction presented with right lower abdominal pain due to renal artery thrombosis is a rare clinical condition that warrants epidemiologic, clinical, angiographic, and prognostic importance. The patient’s condition was acute and was featured with abdominal pain, leukocytosis, and minimal renal impairment.
The case presented here enabled us to widened our vision with patients presented with abdominal pain should warrant clinical suspicion about renal infarction although this is a rare clinical entity.
Renal infarction (RI) is an uncommon condition resulting from a sudden disruption of blood flow in the renal artery. RI is frequently misdiagnosed or diagnosed late because of its rarity and nonspecific clinical presentation, which may result in irreversible damage to the renal parenchyma or an increase in the risk of other embolic events affecting other organs. The prevalence of RI has been estimated from autopsy studies at 14 per 1000 [1]. Recent studies based on admissions to the emergency department have reported estimated incidences of 0.004%–0.007% [1,2]. Many etiologic factors are known to favor the occurrence of RI, but atrial fibrillation (AF) is currently considered the most important risk factor for this condition. AF was recently identified as the main causal factor in 64% of published cases of RI [3], and an incidence of renal thromboembolism of 2% was reported in a series of almost 30,000 patients with AF followed for up to 13 years [4]. Other risk factors for RI include valvular or ischemic heart disease, endocarditis, hyper coagulation disorders, hematologic disease, and spontaneous renal artery dissection, reflecting the multiplicity of underlying causal mechanisms. However, despite extensive investigations, the cause of RI remains undetermined in some cases. Renal infarct affects elderly patients, with an average age of 67 with neither gender nor predominance side predominance. Patients generally complain of flank pain and/or upper abdominal pain which are often associated with nausea and vomiting. Occasionally, patients may have hematuria. Fever is also common and was present in about half of the reported cases. Blood pressure may be acutely elevated, and this is presumed to be through a renin-mediated mechanism. Signs of extra renal embolism may also be present. In contrast, renal infarct may be completely asymptomatic and then diagnosed incidentally as a result of abdominal CT examination5. Here we will report a rare case where a young patient without any risk factors presented with lower abdominal and back pain due to acute renal infarct and successfully managed quickly by percutaneous renal artery thrombus extraction followed by stenting.
This 41-year-old normotensive, non-diabetic, nonsmoker Bangladeshi gentleman presented to the emergency department with 12 hours history of lower abdominal pain and back pain. He was admitted to an outside hospital 10 hours prior to our Emergency unit, where no obvious cause of pain was sought out there. On arrival his BP was 110/80 mm Hg, Pulse 80/min, body temperature 36.6-degree C. USG whole abdomen done outside hospital showed no abnormality. In our Emergency unit CT scan whole abdomen with contrast done, advised by general surgeon suspecting acute abdomen which revealed no definite etiology. They found a large wedge shaped area of infarct in the anterior cortex of the right kidney measuring maximum 6.2 cm in largest dimension (Figure 1). Both kidneys are normal in position, size & contour, there are two renal arteries seen on the right side. The main renal artery is arising at L1 vertebral level at 10 O’clock position. The main renal artery showed slightly irregular outline and ill-defined irregular filling defect approximately 3 cm distal to its origin suggestive of intraluminal thrombus. From emergency unit urgent cardiology consultation was requested which was arranged immediately. Immediately ECG & echocardiography were done, which revealed no significant abnormality. Neither past nor present cardiac issue was found. Abdominal CT showed normal abdominal Aorta. No source of thrombo - embolism was found. After discussion with patient party and with their full consent it was decided to take the patient to cath lab for immediate renal angiography.

Renal angiography showed right renal artery thrombosis (Figure 2). So we decided to aspirate the thrombus with suction catheter. After suction tight stenosis was noticed just before the bifurcation of the main renal artery. We crossed the lesion with a floppy wire and gradually dilated the lesion with 2.0 mm X 15 mm and 4.5 mm X 10 mm balloons successively. A dissection was noticed just 3 cm after the origin of right renal artery.

So we decided to put two stents. Distal segment was stented with 6.0 mm X 18 mm and a 7.0 mm X 18 mm stent was given overlapping & covering proximal to that, covering the dissection. Final angiogram showed right renal artery was well dilated with good distal flow and patient’s pain almost subsided immediately (Figure 3).To find out the cause behind the acute thrombosis, patient was evaluated for anti-phospholipid syndrome, protein C & S deficiency and hyperlipidemia which all came negative. Patient was discharged after 4 days with pain free and stable condition.

Blood Chemistry:

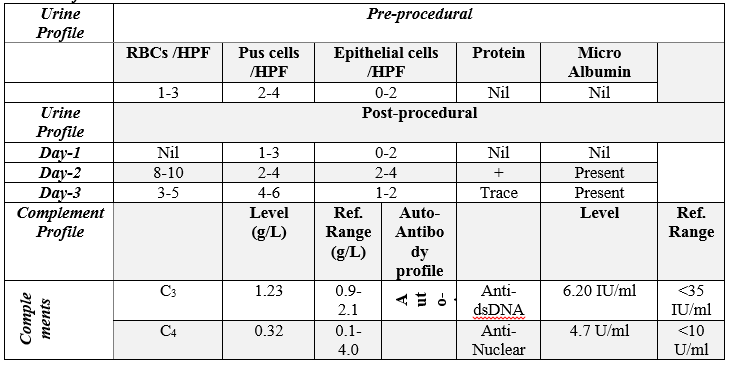

Follow-up Investigations:
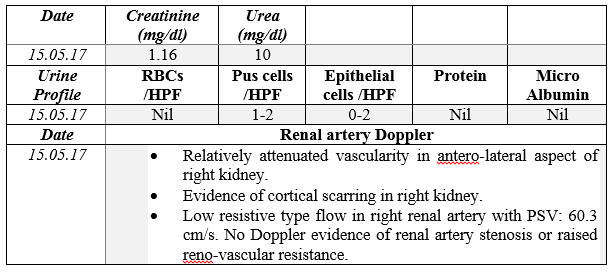
The patient was followed up. The follow-up investigation profile after 03 months:
Renal infarct is typically caused by blood or cholesterol clots occluding the renal artery or branch vessels. The source of blood clots, typically, is from atrial fibrillation causing thrombogenesis in the left atrium and left atrial appendage. Cholesterol-based emboli cause partial occlusions with a more chronic presentation. In a study of over 600 patients with peripheral arterial thromboembolism, the most common site of peripheral arterial thromboembolism was the extremities (61%), followed by the mesenteric arteries (29%), the pelvic arteries (9%), the aorta (7%) and, followed last, by the renal arteries (2%) [4]. In a case series of 27 patients, 41% had obvious cardiac disease, almost all with atrial fibrillation; however, 59% had no discernible structural or arrhythmic cardiac disease [8]. Idiopathic patients are typically younger [8] and have a paucity of thrombogenic risk factors [9].
Complete infarct (involving entire kidney due to occlusion or interruption of the renal artery) is the rarest, seen typically after trauma or interventions involving the aorta [11]. Most kidney infarction results from emboli caused by atrial fibrillation or endocarditis11 causing only partial occlusion of the renal artery or a branch. Rare causes reported include spontaneous renal artery dissection [12], dilated cardiomyopathy [13], paradoxical embolism [14,15] and involved multiple organs. Bilateral infarction has also been reported7 including bilateral (global) renal infarction subsequent to dissecting aneurysms of the aorta [16] with septic emboli from endocarditis, lupus vasculitis or with sickle cell disease [17] or fibro- muscular dysplasia of the renal arteries [18,19]. Reports of other causes associated with renal infarction include trauma, vasculitis, instrumentation, transplant, sepsis [17], sickle cell disease [20] and anti-phospholipid antibody syndrome [21,22] cocaine use [23] and subsequent to carotid artery dissection [24]. In our case there were no risk factors.
The most common complaints at presentation are flank pain [7] or abdominal pain [25], usually constant in nature [5]. Other common features include fever [7,8], nausea and vomiting [7,8,25]. Lumbar and flank tenderness [8] are seen and are even more likely in the idiopathic/younger group. Oliguria is rarely found [25]. New-onset hypertension is uncommon, but can be seen especially if there are underlying renal artery lesions [11].
The typical patient tends to be older, with an average age of 67 in one series [7], although significant portions are younger. Reviewing 89 cases from the literature [2,7,25,26] the mean age at presentation was 65.7 years, with no significant gender predominance or right or left kidney predominance. About 10% of the cases presented with bilateral renal involvement. Previous thromboembolic events in 20/89 (22%) were observed.
Urinalysis is recommended, with hematuria being a very common finding, seen in all cases in one study [7]. However, hematuria is not universal, with about one-half of the patients in another study showing no hematuria [25], and two cases from another center also with no hematuria [27]. In contrast, elevations of lactate dehydrogenase (LDH) are almost universal, with nearly all patients in one study [8] and in all cases in other reports [3,27]. Proteinuria was seen in 45% of the patients in one retrospective case review [25]. The white blood cell count was often elevated [3,8]. Serum creatinine was not markedly elevated at presentation, but a small increase was seen [8] at peak in one study and a more marked elevation was seen in another slightly larger case review [25]. C-reactive protein is also often elevated [8].
Because of the infrequent nature of this malady, no large prospective studies have evaluated the optimal treatment modalities regarding the dosing of heparin, the use of low molecular weight heparin or thrombolytics or using medical management vs. surgical management. At this time, there are only recommendations based on the consensus in the literature.
The most common sequel to renal infarction is loss of renal function and persistent hypertension [11]. However, many patients go on to have normal kidney function [7,11,25] with no permanent hypertension. A small percent will need dialysis, 8% in one case series [25].
Repeat embolic events have been observed, some with events prior to the renal infarct and some with subsequent events [25]. Because of the lack of prospective study data, it is unknown what the benefit of continuing anticoagulation would be. However, given data regarding other catastrophic thrombotic events, it is likely recommended to continue indefinitely in the setting of atrial fibrillation.
Renal infarction is an extremely rare clinical condition. Sharing the knowledge of its epidemiologic, clinical, angiographic, and prognostic features are noteworthy. We report such a rare clinical entity with its successful interventional treatment not only to notify the clinicians but also for identification of such cases clinically, diagnose it in early phase and treat it successfully. As it is an extreme rare clinical scenario it was a challenge for us. We took the challenge and overcome it successfully with full recovery of the patient. So, for the clinicians we should be aware of such rare conditions & their epidemiologic, clinical, angiographic features and treat these cases in time and save the vital organs of human body as well as serve the humanity.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
