
Review article | DOI: https://doi.org/10.31579/2641-5194/001
Jangaon Institute of Pharmaceutical Sciences, Depot. Of Pharmaceutics, Jangaon, India.
*Corresponding Author: Jangaon Institute of Pharmaceutical Sciences, Depot. Of Pharmaceutics, Jangaon, India. e-mail: swathigoli45@gmail.com
Citation: Swathi Goli. Peptic Ulcer Disease: Maintenance treatment with H2 blockers. J. Gastroenterology Pancreatology and Hepatobilary Disorders. 1(1) Doi: 10.31579/2641-5194/001
Copyright: © 2017 Swathi Goli. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 08 December 2017 | Accepted: 26 December 2017 | Published: 30 December 2017
Keywords: peptic ulcer disease; helicobacter pylori; nonsteroidal anti-inflammatory drugs; eradication treatment
Peptic ulcer disease (PUD) is a prevalent disease, it affecting around 5-10% of the general population worldwide, but with notable regional and racial variations. The two most common etiological causes are the chronic infection with Helicobacter pylori (Hp) and the use of non-steroidal anti-inflammatory drugs (NSAIDs). Its diagnosis is based mainly in the endoscopy and the active search of concomitant Hp presence. The discovery of the link between H. pylori and peptic ulcer has changed dramatically its management, because it has become a curable infectious disease.
The eradication therapy of is the best choice to achieve the final cure of PUD in infected patients. Several current international recommend a standard triple therapy as first-line therapy, including a proton pump inhibitor and a combination of amoxicillin and clarithromycin. This combination therapy has shown a decreased efficacy over the years. The main reason is increasing antibiotic resistance, particularly to clarithromycin and metronidazol, of certain Hp strains. Several new treatment options or modifications of already established regimens have been introduced in last years, to overcome these treatment failures.
For the subgroup of patients with H. pylorinegative ulcers, avoiding NSAIDs intake also has a clear influence in evolution of the disease and in some cases drives to the complete healing of the peptic ulcer. In refractory or recurrent cases, continuous therapy with anti-secretory agents and/or the replacement of conventional NSAIDs by selective drugs for inhibition of cyclooxygenase-2 (COX-2) are useful treatment options.
Peptic ulcer (PU) can be defined as the presence of a profound loss of substance affecting the mucosa of the stomach and/or duodenum, reaching beyond the muscularis mucosa, generally to the muscle layer due to the environmental gastric acid secretion.
The two most common etiological causes are the chronic infection with Helicobacter pylori (Hp) and the use of non-steroidal anti-inflammatory drugs (NSAIDs), including of course, the acetylsalicylic acid (ASA). There are other less common causes that can cause a PU, which are considered together, account for less than 5% of cases. Zollinger-Ellison syndrome or gastrinoma is one among them which is a neuroendocrine tumor, usually located at the head of the pancreas or in the duodenal wall, overactive and gastrin secretory (Table 1).
The goals of pharmacotherapy are to eradicate H pylori infection, to reduce morbidity, and to prevent complications in patients with peptic ulcers. Acid suppression is the general pharmacologic principle of medical management of acute bleeding from a peptic ulcer, using histamine-2 receptor antagonists (H2RAs) and proton pump inhibitors (PPIs). [38] Both classes are available in intravenous or oral preparations. Discontinuation of NSAIDs is paramount, if it is clinically feasible. For patients who must continue with their NSAIDs, PPI maintenance is recommended to prevent recurrences even after eradication of H pylori.
Epidemiology
The glandular parts of the stomach located in the antrum and fundic regions are responsible for secretion of the enzymes and gastric acid for digestion of food. The acid-secreting oxyntic cells or parietal cells in the fundic region are the main sites of gastric acid secretion. The regulation of the secretion of gastric acid is carried out by various hormones and neurotransmitters (Figure 1). The parietal cell secretion of acid is mediated by the primary modulator histamine (HA) which may be released when enterochromaffin-like (ECL) cells are stimulated by gastrin (released from G cells of the antrum) and acetylcholine (Ach) (released from enteric neurons). Stimulation of the vagus nerve is known to initiate the release of both gastrin and acetylcholine (ACh) from their respective sites.
Acetylcholine can also directly stimulate parietal cells to increase acid secretion. Gastrin is also capable of stimulating the proliferation of the parietal cells by a direct action. Acetyl choline, histamine and gastrin stimulate acid secretion by activating specific G-proteincoupled receptors on the basolateral membrane of the parietal cells. ACh and gastrin activate phospholipase C to catalyze the formation of diacylglycerol and inositol triphosphate from membrane bound phospholipids. The release of Ca2+ from intracellular stores and the subsequent increase in cytoplasmic calcium ions (Ca2+) activates H+ /K+ -ATPase enzyme system (gastric proton pump). The binding of HA to the H2 -receptor activates adenylate cyclase, resulting in an increase in cyclic AMP, which activates the proton pump [11]. The proton pump is thus, the terminal stage in gastric acid secretion, which makes it an ideal target for developing irreversible inhibitors of acid secretion.
Histamine exerts a strong stimulant action on the gastric acid secretion from the parietal cells by acting on histamine H2 -receptors. The H2 -receptor antagonists were the first class of drugs to demonstrate an effective reduction in acid secretion. The discovery of H2 -receptor antagonists revolutionised the field of treatment of peptic ulcer as these were not only effective at healing ulcers but also kept them in remission when given as maintenance therapy [Bianchi PG, Tam PK, Saing H, Collen MJ]. Early studies indicated that these agents could heal peptic ulcers in 60% to 85% of patients within 4 to 8 weeks, compared to 20% to 40% healing rates in the placebo group. [Thomas JM, Misiewicz G et al, Feldman M ]. Currently, there are four US-FDA approved H2 -receptor antagonists in market: cimetidine, famotidine, nizatidine and ranitidine. The advent of this class of drugs came in early 70s when Black et al [Black JW] reported the discovery of thiourea derivative burimamide, the prototypic agent from this class, which inhibited acid secretion based on the antagonism of the histamine-2 receptors. Despite its higher potency over commercially available anti-secretory agents at that time (anticholinergics), its introduction into therapy was hampered by its poor bioavailability.
The mechanisms through which the Hp favours the development of PU, are better known in the duodenal, than in gastric side. In patients infected with the bacteria, triggers an inflammatory and immunological response to the level of the gastric and duodenal mucosa, with release of number of pro-inflammatory cytokines such as IL-8 and TNF-α. Thus appears acute and chronic gastritis, which reduces the thickness and quality of mucus layer [8].
The most typical manifestation of the uncomplicated peptic ulcer is the presence of a burning or corrosive pain, mainly located at the epigastrium. Sometimes, it can be characterized as a vague abdominal pain, nausea, vomiting, diffuse discomfort, or may be perceived as a pressure or feeling of abdominal fullness or hunger.
Typically in the duodenal ulcer, epigastric pain appears during the fasting state, between one and three hours after meals or at night. It can also occur in relation to stress situations.
This epigastric pain is relieved by eating any kind of food or taking antacids pills in few minutes, and reappears cyclically again, within two hours. Symptoms may persist for several days, weeks or months.Two- third of patients with duodenal ulcer refer that the pain wakes them at night, being uncommon to have pain upon waking in the morning. There is infrequent presence of anorexia and/or weight loss in these patients. By contrary, most of them often manifest hyperphagia and weight gain, probably because the pain usually subsides with ingestion of food. This is the well known three steps - sequence of “pain/ingestion of food/alleviation” [14].
Several complications can occur in patients with peptic ulcer disease of any etiology. They are the main reasons for the high morbidity and mortality associated with this disease found until now.
The routine application of different gastroprotection strategies and eradication therapies for Helicobacter pylori infection, have reduced significantly the incidence relative to that seen in the previous decades. They are more common in habitual smokers and chronic NSAIDs users [16,17]. There are four major complications of peptic ulcer disease: Bleeding, perforation, penetration and obstruction.
Although its incidence has declined a little in the recent years; however remains being the most common complication and appears in around 10-20% of patients. It is a frequent cause of admission in emergencies.
Ulcers related with NSAIDs are more likely to bleed than those caused only by H. pylori chronic infection. Populations at a greatest risk are the elderly and those with other serious conditions, such as respiratory, cardiac, cerebrovascular o renal problems [18].
A total of 80-90% of upper gastrointestinal hemorrhage are not from variceal bleeding origin , and around 40-50% of these are caused by peptic ulcer disease. The mean associated mortality is around 5.5% [19].
It is an uncommon complication, which represents approximately 5% of ulcer-related complications. Until about 1970, peptic ulcers represented the most common cause of obstruction to gastric emptying [25]. In the last years, however, has decreased the frequency of obstruction secondary to peptic ulcer and currently gastric malignancies are the leading cause of gastric outlet obstruction [26].
It is mandatory to perform a good clinical history and a complete physical examination, in order to make a complete data collection of all the symptoms and signs of PUD. Also, it is extremely important to register all the past medical antecedents, and the duration of alcohol intake, history of NSAIDs and smoking consumption, and also for the posible existence of previous episodes of peptic ulcer.
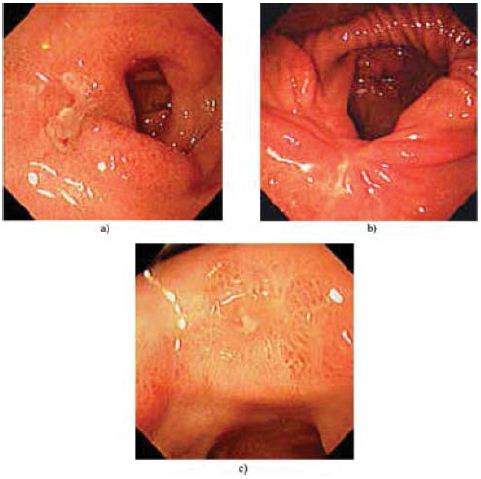
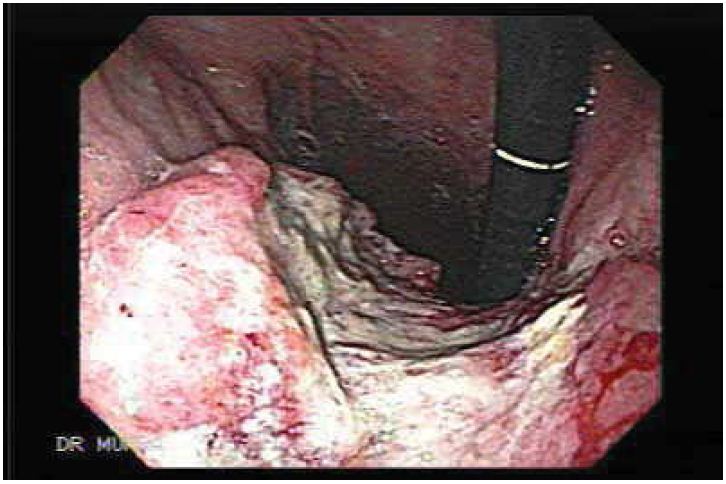
The signs suggesting benign origin are the presence of regular mucosal folds surrounding the ulcer base and the fibrin deposit at the crater base (Figure 1). The features that suggests malignancy, are the finding of overhanging margins, irregular or thickened borders and/or the presence of an ulcerated mass, that protrudes into the lumen (Figure 2).
Malignancy of the duodenal ulcers is exceptional. Therefore, it is rutinary biopsy is not recommended. However, it is mandatory to take several mucosal biopsies form the margins at any gastric ulcer, despite it is benign appearance. A follow-up endoscopy will be performed until the healing is completed [27].
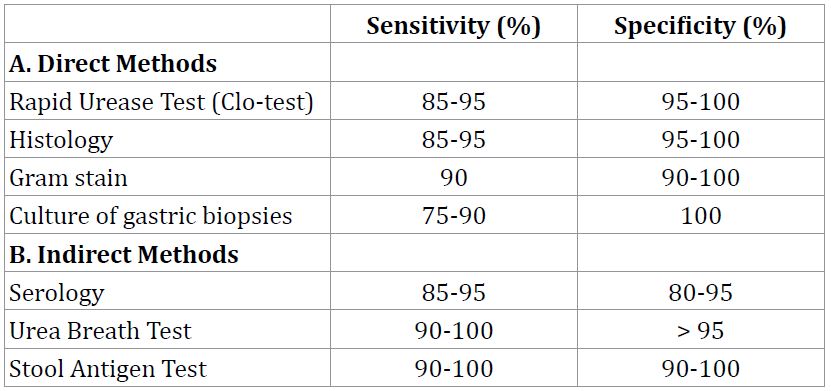
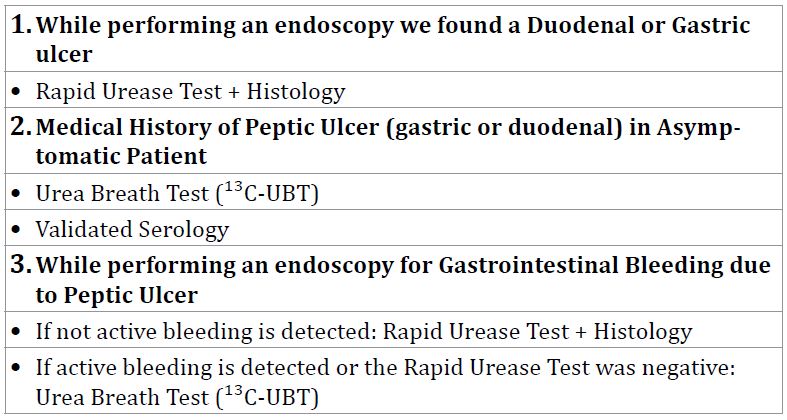
Diagnostic tests for H. pylori are divided into direct (based upon the need for endoscopy) and indirect tests, and several tests are used not only for diagnosis, but also in the follow-up after the eradication treatment in order to confirm this one (Table 2 and 3) [28].
General care
It is essential to avoid potential contributing agents such as NSAIDs or tobacco. There are no firm recommendations on alcohol intake or dietary habits, apart from not eating foods that can aggravate the symptoms [29].
Helicobacter pylori-negative
The main etiology is related to the use of NSAIDs, so withdrawing these treatments is a crucial step. In H. pylorinegative, NSAID-negative ulcers, a detailed search should be made to detect other contributing factors, such as medical comorbidities, poor nutritional status, ischemia and acid hyper-secretory disorders. The management of uninfected patients is based on the classic anti-secretory therapy [29,30].
PPIs are most effective when taken 30-60 minutes before meals. Global ulcer healing rates are above 75%, although PPIs achieve better results than H2RAs (near 100%). Therefore, the use of PPIs is recommended whenever possible. If a standard PPI therapy fails to heal a peptic ulcer, it is recommended to try twice daily dosing or switch to another PPI. For large ulcers (>2-3 cm), double dose of PPI is recommended for 12 weeks. Higher doses are necessary to control symptoms in other hypersecretory states, such as the Zollinger-Ellison syndrome.
The H2RAs and PPIs are usually well tolerated with a low incidence (< 3>
In this regard, it has been described that pantoprazole has the lowest potential for P450 metabolism and drug interactions [32]. In view of the inconclusive data, PPIs with weaker inhibition power of CYP2C19, are preferred in combination with clopidogrel, compared with those with stronger inhibition such as omeprazole [33].
H. pylori infection in NSAIDs users: H. Pylori infection is associated with an increased risk of the development of gastroduodenal ulcers and its complications in NSAIDs and low-dose aspirin users [34]. The available data helps in H. pylori eradication before starting NSAIDs treatment. It is also appropriate to test and treat this infection, following the presentation of any clinical ulcer. If NSAIDs or aspirin are continued, treatment of such patients with a PPI in addition to the eradication therapy, can reduce the risk of recurrent ulcer complications.
Refractory ulcers: Peptic ulcers that have not healed after proper treatment for 12 weeks are considered as refractory lesions [29]. In this context, the following conditions must be investigated: Persistence of H. pylori infection or false negative in the initial diagnosis, hidden NSAIDs use, non-compliance of prescribed treatment, giant or fibrotic ulcers, ulcerated tumors, tobacco consumption and acid hypersecretory states. Chronic ischemia caused by the narrowing of celiac artery may also be considered, in this situation. In the absence of all these risk factors, it is recommended to insist on all medical options before indicating surgery.
Pregnancy and lactation: Omeprazole is listed by the FDA as a pregnancy class C medication, whereas all other currently available PPIs, and H2RAs such as cimetidine and ranitidine, are class B. Although the results in some analysis of prospective data have shown that the global risk is low in pregnancy with potential toxicity during lactation, the lack of data in humans, precludes to achieve definitive conclusions regarding their safety [35]. Currently, there are no guidelines to treat H. pylori infection during pregnancy. It has been suggested that eradication should be deferred after delivery and lactation [36].
Treatment choices include standard triple therapy, sequential therapy, quadruple therapy, and levofloxacin-based triple therapy. Standard triple therapy is only recommended when resistance to clarithromycin is low. Chronic use of NSAIDs in patients with H. pylori infection increases the risk of PUD.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
