
Case Report | DOI: https://doi.org/10.31579/2767-7370/041
1 Assistant Profession Urology. Grant Medical College and J.J. group of hospitals, Mumbai. Institute where the work was carried out: Government Medical College, Nagpur, India.
2 Consultant Urologist and Head of Department, Urology. Government Medical College, Nagpur. Institute where the work was carried out: Government Medical Collège, Nagpur, India.
3 Senior Registrarin Urology. Grant Medical College and J.J. group of hospitals, Mumbai. Institute where the work was carried out: Government Medical Collège, Nagpur, India.
*Corresponding Author: Kaustubh Vaidya, Assistant Professor in Urology. Grant Medical College and J.J. group of hospitals, Mumbai. Institute where the work was carried out: Government Medical College, Nagpur, India.
Citation: Kaustubh Vaidya, Dhananjay Selukar, and Ojas Vijayanand Potdar, (2023). Penile Constriction Devices – 3 Cases Experience, J. New Medical Innovations and Research, 4(4): DOI: 10.31579/2767-7370/041.
Copyright: © 2022, Kaustubh Vaidya. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 24 April 2023 | Accepted: 28 July 2023 | Published: 21 August 2023
Keywords: penile constriction; decompression
Penile constriction devices are a rare but challenging clinical entity in urologic practice. they are applied for myriad reasons and depend on the age group. In adult and elderly males, they are applied to enhance sexual experience, in adolescent and young males they are applied as a part of sexual curiosity. Here we present a series of 3 cases with penile constriction devices. A 24-year-old male patient presented after 5 days with a metallic bolt over his penis, with distal edema and discoloration. The bolt was cut with a motorized rotating saw and decompression was done. A 57-year-old man with a rubber band applied to the base of his penis, the rubber band was cut, and the patient was managed conservatively. And a 51-year-old male with a metal ring applied to the penile base before sexual intercourse, The ring was cut with a rotating saw, and penile congestion was relieved. All the cases were managed conservatively without any adverse sequelae.
Penile constriction devises are a rare but challenging clinical entity in urologic practice. They are applied for myriad reasons which vary with the age group. In adult and elderly males, they are applied to enhance sexual experience, in adolescent and young males they are applied as a part of sexual curiosity.
A 24-year-old male presented to the emergencydepartment with complaints of penile pain and swelling. He stated that 5 days prior, after watching pornographic videos, he had placed a large metal bolt over his penis to increase penile length and to enhance his sexual experience. Followingthis he had fallenasleep with the metal bolt on and after wakingup in the morning, around8 – 10 hours later,he could not remove the bolt. He had notedincreased swelling and pain over the swellingover the penis.
Out of embarrassment, patient did not seek medical attention for 5 days. Examination revealed a stainless-steel bolt over his penis at the proximal aspect. Distal penile stump was edematous with congested appearance (Figure1). Mild blackishdiscoloration of the skin was present with dusky appearance. He was able to void with only minimal difficulty, urinary bladder was not palpable. Patient was posted for surgery under spinal anesthesia. A tongue depressor was placed under the bolt. Dorsal slit was given to decompress subcutaneous edema and to glide out the bolt. But these attempts failed. So, decision was taken to cut the metal bolt. Metal bolt was cut with a motorized circular saw (Dremmel rotating saw) (Figure2,3) at diagonally opposite points into two halves. Tongue depressorkept under the bolt to protectpenile shaft from saw-tooth injury.Damp towels were placed on the exposed skin to protect it from flying sparks. Continuous ice water irrigation was used during sawing to lower the temperature and avoid thermalinjuries to skin and penis.Skin and soft tissues under the bolt area was debrided up to buck’s fascia. Skin closed primarily with 3-0 Monocryl sutures.

Figure 1: Photograph showingthe metal bolt at the base of the penis.
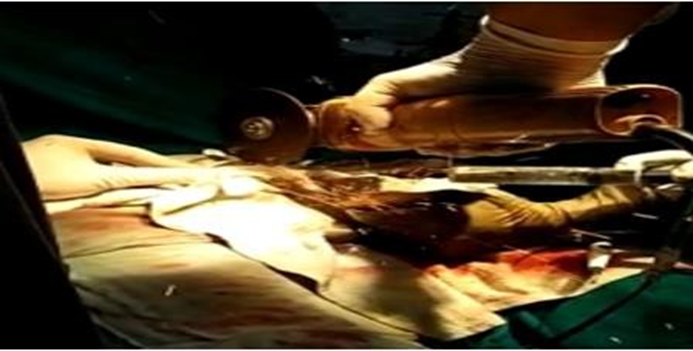
Figure 2: Image showing Dremmelrotating saw being used to cut the metal bolt at the base of the penis.

Figure 3: Image showing the metal bolt cut into two pieces and then removed from the base of the penis.
A 57 years old gentleman presented with rubber band appliedto the base of the glans penis for sexualpleasure. Patient presented 1 day afterapplication of the band (Figure4). Patient triedto cut the band, but failed due to oedemaPatient had engorgedsemirigid distal penis with oedema,with no cyanoticskin changes or any difficulty micturition. Rubber band was cut and with conservative management oedema resolved without any loss in erectile function.

Figure 4: Image showing rubber band trappedat the base of glans penis.
A 51 years old man presented to emergency department with metal ring applied to thebase of penis before sexualintercourse for sexualenhancement. Patient failed to remove the ring post-coitus, and presented 16-18 hrs with penile swelling and pain. Patient had mild difficulty micturition. Ring was cut with a motorised circular saw. Skin ulceration was present under the metal ring, managed conservatively with dressings (Figure5).

Figure 5: Image showing metal ring applied at the base of penis.
Penile strangulation is an unusual clinical condition that was first reported 1755 by Gauthier Penile strangulation with constriction devices can have serious sequalae if it is not treated emergently [2]. Usually patients have delayed presentation, once patient is exhausted with all the home remedies and pain and swelling starts to appear, 5 days in our case. patients present late due to Embarrassment and associated social stigmata, which can have clinical implications. Strangulation can cause vascular compromise with ischemia of skin, loss of penile sensation, skin necrosis and ulcerations, sepsis, urethral injuries, urethro-cutaneous fistula formation, gangrene or even autoamputation of penis. In 1991, Bhat et al. presented an excellent original classification for penile incarceration composed of five grades from only distal edema as follows: [3]
Silberstein et al., developed a grading system with two broad categories as low- and high-grade penile injuries, with high grade injuries as those requiring secondary surgical intervention after removal of the strangulating object [4]. The type of constricting device appeared to impact the degree of penile injury, with the more severe injurie occurring from non-metallic devices [4]. Chronic use of constriction devices may result in lymph stasis and long-term lymph edema mimicking elephantiasis [5]. There are many methods for removing thick, hardened strangulating materials, including aspiration of the corpora or the use of saws, grinders, dental drills, and the string method, degloving or amputation of penis [6].
Though a rare clinical presentation in urologic practice, penile strangulating devices needs urgent decompression to prevent long term sequalae.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
