
Case Report | DOI: https://doi.org/10.31579/jnmir.2021/002
Department of Internal Medicine, Mohamed Tahar Maamouri Hospital, Nabeul, Tunisia.
*Corresponding Author: Zeineb Alaya, Department of Internal Medicine, Mohamed Tahar Maamouri Hospital, Nabeul, Tunisia.
Citation: W Osman, L Hassini, Z Alaya, Mohamed A Khalifa, M Mtaoumi, et al. (2021) Pelvic osteosarcoma: resection and reconstruction using a customised plate. J. New Medical Innovations and Research. 2(1); DOI:10.31579/jnmir.2021/002
Copyright: © 2021 Zeineb Alaya, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 19 October 2020 | Accepted: 11 December 2020 | Published: 06 January 2021
Keywords: osteosarcoma; pelvis; reconstruction; plate; Enneking zone; neoadjuvant chemotherapy; autologous graft; lombo-femoral plate
Introduction
Primitive bone tumours of the pelvis represent a considerable challenge for carcinologic surgeons. Resections made in the acetabular zone could disrupt the continuity of the pelvic ring. The morbidity that comes after such a procedure requires a reconstruction surgery in order to improve the functional outcome. In this aim, multiple techniques have been reported.
Case report
We report the case of a 23-year-old male with no medical history diagnosed with a right pelvic bone osteosarcoma located in Enneking zones I and II. He first underwent neoadjuvant chemotherapy followed by a large resection of the whole bone. A reconstruction was then made using a vascularized fibular autologous graft and stabilized by a long customized lombo-femoral plate. Recovery of walking was possible using crutches. No recurrence was note at one year follow-up.
Conclusion
Malignant primitive tumours of the pelvis threaten the vital and functional prognoses of patients. It is now possible to perform conservative resections in more than 80% of case without compromising the survival of patients or their functional outcome.
Ten to 15% of primitive malignant bone tumours are localized around the acetabulum [1,2]. Their prevalence is as much as 10 new case per year per million [3]. Regardless their histological variety, these tumours raise two major technical challenges : fist, large in resection margins have to be respected while resection of a tumour that is often of considerable size because of frequent diagnosis delay (4-7);second, a complex reconstruction is often mandatory because of the disruption of the pelvic ring. In order to improve the functional outcome after large pelvic resections of these tumours, multiple techniques have been reported such as arthrodesis, prosthetic reconstructions and different bone grafting. We report a right pelvic bone reconstruction using a vascularized fibular autologous graft and stabilized by a customized lombo-femoral plate.
A 23-year-old otherwise healthy male presented with unbearable pain of the right inguinal region, evolving for many weeks. Plain antero-posterior pelvis radiographs showed a Lodwick type II large lytic lesion of the right ilium with surrounding soft tissue calcifications (fig. 1).

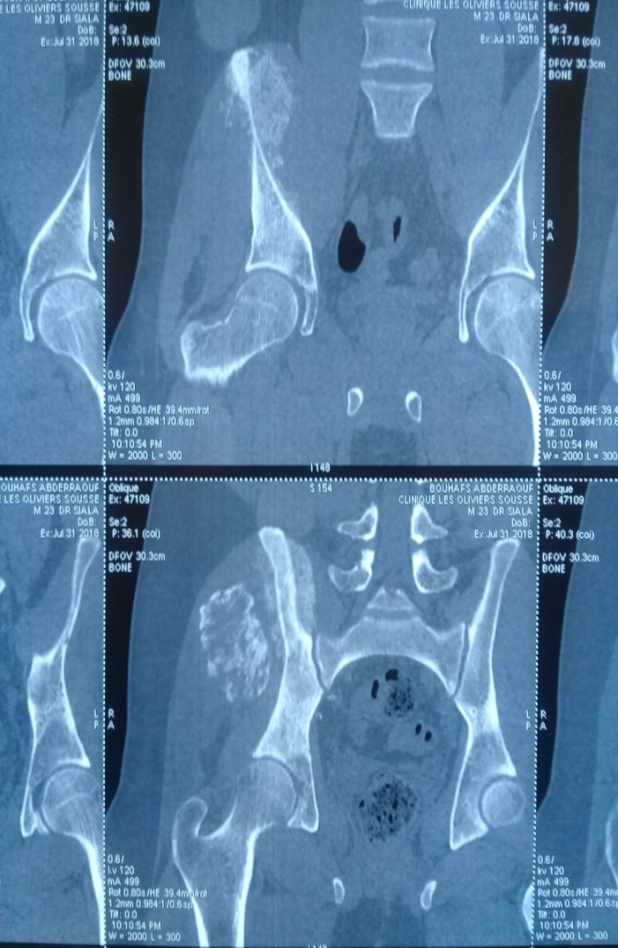
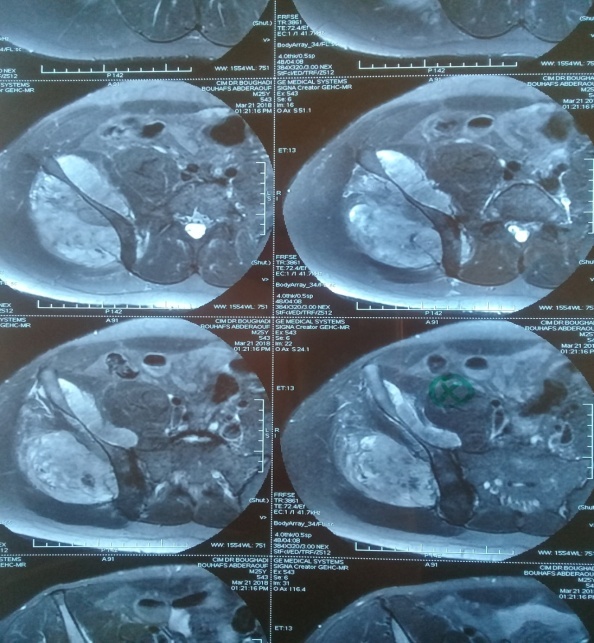
ComputedTomography scan (CT scan) confirmed this aggressive lesion of the rightilium (fig. 2).Magnetic Resonance Imaging (MRI) precised that the lesion was located in Enneking zones I and II.However, this first MRI was not able to assess the integrity of the coxo-femoral and sacro-iliac joints with confidence (fig. 3).
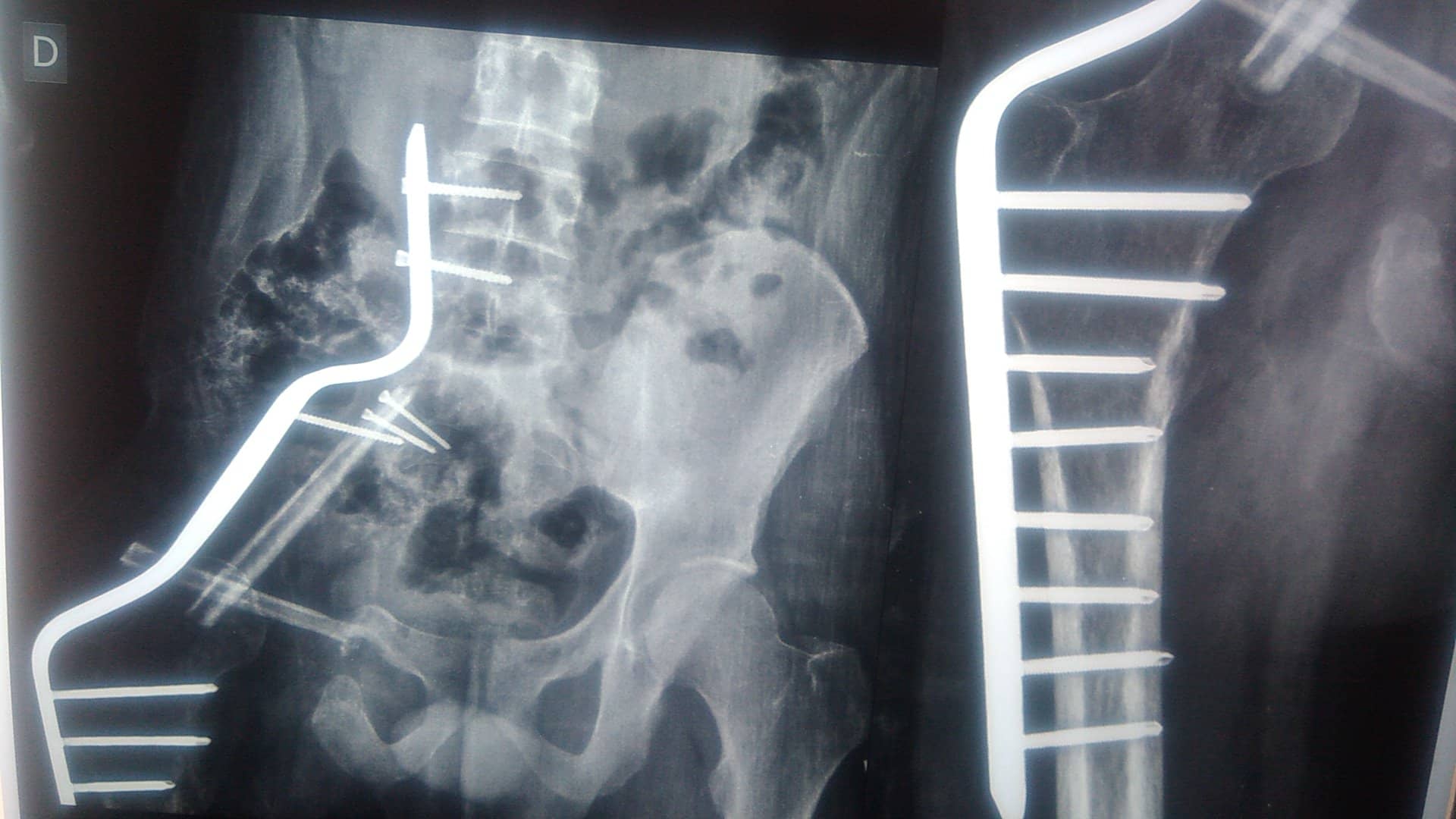
The spreading investigations were all negative. A surgical biopsy of the lesion was made and the diagnosis of osteosarcoma was histologically confirmed. The patient underwent neoadjuvant chemotherapy. A second MRI assessment was then made, showing a mild regression of the tumour with no extension to joints. A large surgical resection of the whole right pelvic bone was then performed. The reconstruction was made using a vascularised fibular graft and stabilized by a customized long lombo-femoral (fig. 4,5).


The post-surgery was simple and the wound healed at conventional delay (fig. 6). Figure 7 shows the post-operative plain radiograph (fig. 7).


A pelvi-crural cast was crafted and maintained for 6 weeks. The radiological control at 1 year follow-up showed an ongoing bone graft healing process (Fig.8). Functional outcome was average with the patient being able to walk using 2 crutches.

A large number of musculoskeletal tumors can affect the pelvis. Several studies have reported bone sarcomas as the most common lesions, followed by soft tissue sarcomas and metastatic lesions. The most frequently observed pelvic sarcoma is chondrosarcoma, followed by osteosarcoma [8]. Ten to 15% of all primary bone tumors are located in the pelvic bone of which chondrosarcoma in adults, Ewing's sarcoma in children, and osteosarcoma in adolescents represent the most common histological subtypes [9] Pelvic resections are challenging and complex. They are technically difficult due to sometimes the size of the tumor is very large, and anatomically it closes to pelvic viscera and neurovascular structure. Previously, hemipelvectomy was the standard surgical treatment for primary pelvic sarcomas. Recently,with advancements in surgical techniques and chemotherapy and radiation therapy, limb salvage procedures have also emerged as viable modalities. Di Caprio and al. [10] compared in their meta-analysis conservative procedures to amputation. They found that the decision making was mainly based on the patient’s age, the size and the localization of the tumour. Another study of the Italian and the Scandinavian Sarcoma Groups found that high doses neoadjuvant chemotherapy allow a conservative surgical treatment in 90% of cases but increased liver and renal toxicity [11]. Progressively, pelvic amputation became a rare indication. Furthermore, life quality and function scores were significantly poorer with amputation compared to conservative procedures [12, 13], with similar results regarding tumour resection .Davis and al. [14] reported a series of 36 patients among whom 12 underwent amputation. Shortform-36 (SF-36) score was lower in this group compared to patients who underwent conservative procedures (45 versus 71.1, p=0.03).
Though limb salvage surgery remains difficult and challenging, various methods were used to reconstruct the hemipelvis after periacetabular reconstruction resection, including ischiofemoral arthrodesis or pseudarthrosis, iliofemoral arthrodesis or pseudarthrosis [15],massive allograft [16, 17],autoclaved autograft [18], allograft prosthetic composite [19], custom-made endoprosthesis combined with hip arthroplasty [20], modular saddle prosthesis [21] or modular hemipelvic endoprosthesis. Each reconstruction modality has its own risks and benefits [22].
As reported in the early series of Ennekingand al [23], O’Connor and al [24], Capanna and al [25] and Campanacci and al [6], patients requiring wide muscle resection with nerve sacrifice underwent arthrodesis.Ilio-femoral, ischio-femoral, femoro-obturator and femoro-sacral arthrodesis have been used. The choice depended on the resection zone in the classification of Enneking and Dunham.In the present case, the patient underwent a lombo-femoral arthrodesis. We did not use a saddle or stemmed prostheses for reconstruction because those were very expensivein our country.
The principle of arthrodesis after pelvis resection is to achieve solid union between proximal femur and the remaining pelvis (iliofemoral, ischiofemoral, or sacrofemoral) using plate, screw, or wire. In the present case, we used a customized plate fixes proximally in the 4th and 5thlombar vertebral body and in the femur distally.
The treatment of this pathology is associated to a high rate of complications and a significant declining of quality of life regardless the surgical technique .A high rate of revision is observed in these patients [26]. The two most common post-operative complications are wound infection (with an incidence of 10 to 47%) and local recurrence of the tumour (with an incidence of 28 to 35%) [27,28]. Han et al. showed that surgical margin was the factor most closely related to the local recurrence [29].Our case showed no local recurrence until last follow up. It was probably due to we can achieve wide margin during surgery
Functional results depend on the extent of resection and the method of reconstruction [30]. The disadvantage of arthrodesis includes loss of the hip joint function. Fusion rates of femoropelvic arthrodesis are <50%, in most patient, a stable and painless pseudoarthrosis develops, but with a comparable functional result to that of the alternative reconstruction options [31]. Higher non-union rates were reported with patients undergoing chemotherapy and/or radiation therapy [6, 15]. Until last follow up, functional result of our patient was average with disappearance of pain and resumption of walking using 2 crutches.
Primitive pelvic bone tumours represent a challenging pathology for surgeons. Acetabular resections disturb the continuity of the pelvic ring and require a reconstruction. In order to improve functional outcome after this delabrating surgery, multiple techniques have been reported. Current data shows that complication rate is high and quality of life is significantly compromised regardless the reconstruction procedure used. Since complication in surgery of pelvis tumor is quite high, approach in the management of pelvis tumor needs multidiciplinary team.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
