
case report | DOI: https://doi.org/10.31579/2692-9392/121
Handicap International – Humanity and Inclusion, Kathmandu, Nepal
*Corresponding Author: Aastha Poudel, Handicap International – Humanity and Inclusion, Kathmandu, Nepal
Citation: Aastha Poudel (2022) Pelvic Floor Dysfunction in Right Hemiplegic Female in Rural Nepal. J. Archives of Medical Case Reports and Case Study, 5(4); DOI:10.31579/2692-9392/121
Copyright: © 2022 Aastha Poudel, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 March 2022 | Accepted: 18 April 2022 | Published: 25 April 2022
Keywords: pelvic floor; right hemiplegic
Pelvic floor dysfunction i.e., Pelvic Organ Prolapse (POP) and Urinary incontinence (UI) is seen to be more prevalent in rural part of Nepal and majority of these conditions are seen in females of reproductive age. Pelvic floor dysfunction negatively impacts female's quality of life and if it is associated with female with disability, it increases the severity of their physical, mental, and social well-being and can hinder their full and effective participation in society. Thus, educational programs regarding sex education should be conducted focusing on vulnerable population to increase awareness, advocacy about their sexual and reproductive rights including causes and risk factors of POP and UI.
More than 1 million Nepali females suffer from Pelvic Organ Prolapse (POP), the majority of these patients are of reproductive age group and its prevalence in rural part of Nepal is 36.2%. [1,2] Lack of appropriate reproductive health services, heavy household and farm work during and immediately after pregnancy, malnutrition and smoking (50% of the cause of prolapse) are the leading causes for the prolapse in Nepal [1]. Urinary incontinence (UI) and POP concomitantly occurs with each other as both are mainly due to the weakness of pelvic floor muscle [3]. The suffering caused by the reproductive health problems is seldom shared by the women because of embarrassment, social taboos, fear of abandonment and isolation [2] Stroke is a leading cause in long term disability [4]. Localized damage to the brain such as infarction or hemorrhage mostly causes Pelvic floor muscle weakness, reduces the elasticity of the vaginal perineum muscles aggravating the risk for UI and POP. Several studies concluded that pelvic floor muscle training for UI in female stroke patients significantly increases the activity of pelvic floor muscles, decrease in urinary incontinence by 75 % [5].
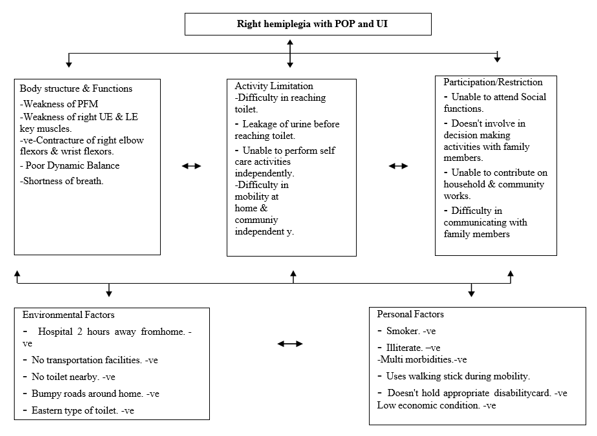
Female living in low and middle income countries are often confronted with low decision- making power about health care and them facing disability adds up barriers in seeking reproductive health services due to embarrassment, their reliance on family in every sectors, lack of disability friendly transportation that limits their access for health care, lack of accessible information about reproductive health, sex education [6]. In this case study, we report about the case of a 48 year female, with right hemiplegia, presented to us in our physiotherapy department of present in Jiri Hospital, Jiri after referral from a Organization of Person with Disability (OPD) called Community Service Association of the Disabled and Blind (CSADB).
A 48year female, chronic smoker with diagnosis of Right hemiplegia for 15 years was presented in our department for rehabilitation on mobility. Her caregiver mentioned she experiences fall while performing daily activities like walking, bathing, picking up objects and also had difficulty speaking fluently. She was diagnosed with incomplete uterine prolapse 6 months ago, but was denying of having any symptoms regarding it. After regular counseling, she admitted having urine leakage while coughing (conducting strenuous activities), difficulty in holding urine before reaching the toilet, difficulty in toilet accessibility, standing and walking for more than 30 minutes. She is dependent on her family members for her activities of daily living and holds a yellow color disability card provided by Nepal government. She is P3L3 and had normal vaginal delivery for all her babies. Due to poor financial condition, lack of access to transportation, embarrassment and lack of self-motivation she delayed seeking health care for POP and UI.
On Observation, the patient’s right side of the body was shifted towards left, her right elbow, wrist and fingers were flexed.
On Sensory, light touch and pin prick on all the key dermatomes of the body was intact, she was able to maintain static and dynamic sitting balance but had difficulty in maintaining dynamic standing balance. Rhomberg’s test for proprioception was positive. Reflexes on both left and right side of the body was normal except babinski sign positive for right foot.
On Motor

The patient had typical hemiplegic gait (decreased swing phase, fast walker). Outcome tools
ICIQ (International Consultation of Incontinence), POP -SS (Pelvic Organ Prolapse Symptom Score) and WHODAS 2.0 (World Health Organization Disability Assessment Schedule 2.0)
were used to assess the severity of incontinence, prolapse and functional dependence of the patient respectively. The patient scored 18 on ICIQ (increased severity) 6 on POP-SS, 90% functional dependence on WHODAS score respectively.
The patient and her caregiver was counseled regarding her condition (urinary incontinence, genital prolapse), its complications, surgical and non-surgical treatment, behavioral modifications (Cessation of smoking, avoid triggers that causes constipation, cough, limit access barriers to toilet) [3,7]. Based on which a patient centered treatment plan was prepared and administered in consultation with the patient and her caregiver which includes Task specific circuit gait training with auditory feedback [8,9]. Pelvic floor muscle training that includes Education of pelvic floor muscles and its functions, recognition training, pelvic floor muscle exercise [ 3,5]. Bladder training (scheduled voiding, urge suppression techniques). All the intervention were demonstrated to both caregivers and patient. Since, patient condition was degraded in terms of activity limitation, participation after having multiple morbidities like COPD, POP and UI later, new disability card of blue color was provided. As she and her caregiver weren’t aware about the provisions given by Nepal Government for disability card holder which had led them to seek delay in health care earlier, Thus, advocacy regarding it was provided. Low economic condition was one of the reason for her to not reach hospital before. So, Transportation fare from her home to the hospital was given after the coordination with Organization of Person with Disability.
The most widespread reproductive health problems in rural part of Nepal is Pelvic floor dysfunction (POP and UI ) with over 1 million of female suffering from this disease.[1,2] Lack of access to skilled attendants during delivery, frequent conceiving, lack of nutritious food, burdens of patriarchy , heavy lifting during and after pregnancy makes it more prevalent [1,2,10].Smoking is said to be one of the leading cause of POP as it triggers chronic cough leading to increase in abdominal pressure and ultimately aggravating the risk for POP. Since our patient is chronic smoker which could be one of the factor causing her Pelvic floor dysfunction [1]. Prevalence of Pelvic floor dysfunction was seen maximum in the age group of 40-49 years (67.3%) which matches our patient’s age i.e. 48 years, excessive stretching, tearing, high parity, multiple deliveries, advancing age are the reasons for these age group to be more prone to having Pelvic floor dysfunction [10]. Greater than 47% of women with Uterine Prolapse waits at least 15-30 years before seeking treatment because of the sensitivity of the condition and shyness of genital exposure, fear of abandonment by their husband and embarrassment [11]. Stroke has shown to be the largest cause of severe disability and has a greater disability impact. It causes weakening of PFM and hypersensitivity of the bladder, reduces elasticity of the vaginal perineum muscle making UI and POP more prevalent (37%) after stroke [4,5]. Stroke patients find difficulty in maintaining continence because of functional impairments such as hemiparesis, impaired mobility, added on top of that reduced toilet accessibility leads to Functional Urinary Incontinence (FUI). Repeated coughing associated with dysphagia and aspiration after stroke exacerbates the risk of Stress Urinary incontinence (SUI). Hence, this might be the reason for our case to have SUI, FUI and prolapsed symptoms [3,11].
Pelvic floor dysfunction are stigmatized in rural Nepal, women with these problems are looked as impure, has low decision making power about health care and women having disability adds up to the barriers in seeking reproductive health services due to lack of economic independence, lack of disability accessible transportation or mobility devices, lack of accessible information as well as accessible health facilities and lack of awareness of available services provided by Nepal Government [12].
As our patient is right hemiplegic and had difficulty in ambulation which was one of the factor leading to functional Urinary Incontinence. So, Task specific circuit gait training with auditory feedback was administered. Practicing specific task related to gait and balance in a circuit manner improves both mobility and gait by improving step length and cadence [13].
Lifestyle modifications like avoiding triggers that increases intra-abdominal pressure such as constipation, obesity, chronic cough should be eliminated which includes cessation of smoke, reducing alcohol intake was also advised? [3]
Behavioral modifications such as timed voiding, bladder retraining with pelvic floor muscle training and supportive devices (pessaries) are recommended as first line of treatment in Pelvic floor dysfunction. Pelvic floor muscle training to stroke patients is difficult due to reduced sensation and insufficient recognition of Pelvic floor muscle. So, use of sensory ball on the surface improves recognition of Pelvic floor muscle by providing the adaptation of stimulated region by rubbing the pelvic floor [5].
Pelvic floor dysfunction adversely affects female’s quality of life and if this disease associates with female with disability, it adds up negative impacts on their physical, mental, and social
Well-being. Thus, educational/awareness raising programs regarding sex education, causes and risk factors of POP and UI, available reproductive health services (surgical and nonsurgical management) should be conducted focusing on vulnerable population to increase awareness, advocacy about their sexual and reproductive rights.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
