
Case Report | DOI: https://doi.org/10.31579/2641-0419/357
Department of cardiology, Hospital University Center Ibn Rochd, Casablanca, Morocco.
*Corresponding Author: Zeine El Abasse, Department of cardiology, Hospital University Center Ibn Rochd, Casablanca, Morocco.
Citation: Zeine El Abasse, Zahri Soukaina, Sara abouradi, Salim Arous, Rachida Habbal, (2024), Peculiarity of Systemic Lupus Erythematosus with Cardiac Involvement in Case Report and Literature Review, J. Clinical Cardiology and Cardiovascular Interventions, 7(3); DOI:10.31579/2641-0419/357
Copyright: © 2024, Zeine El Abasse. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 11 March 2024 | Accepted: 18 April 2024 | Published: 27 April 2024
Keywords: Heart failure; congenital disorder
Abstract
Systemic lupus erythematosus (SLE, or lupus) is a condition in which the immune system attacks healthy cells and tissues throughout the body, it is characterized by aberrant activity of the immune system, leading to variable clinical symptoms.
Case: A Moroccan 54 years old women presented a progressive dyspnea associated with palpitations with a history of hyperthyroidism, a pericardial effusion of great abundance punctured, the remainder of the diagnostic workup had revealed lupus erythematosus. The echocardiography found a global hypocontractility with an ejection fraction at 25%, a dilated atrial mass and mitral regurgtitaion, moderate aortic regurgitation with an image of vegetation on the non-coronary cusp, right ventricular dysfunction. Laboratory investigations revealed bycitopenia with high inflammatory markers, a renal dysfunction test result. Immunological tests showed a high positive antinuclear antibodies ans DNA antibodies. While hospitalization the patient presented a constrictive chest pain , the electrocardiogram showed an st segment elevation in the inferior derivation in relation with a coronary spasm.Three days later the patient presented a sudden neurological deficit type of right hemiparesis with facial paralysis and aphasia, the emergency MRI objectified a cortical frontotemporal stroke, in the acute phase, patient was thrombolysed by metalysis , finally the diagnosis of vasculitis of the central nervous system (CNS) was retained with ischemic and hemorrhagic lesions in favor of lupus vasculitis of the CNS .
Discussion: Systemic lupus erythematosus (SLE) is a chronic autoimmune disorder that may affect several different organs(5) , the underlying pathophysiologic mechanism remains unknown, new autoantibodies, such as antibodies to DNA , antibodies to extractable nuclear antigens , and anticardiolipin antibodies, were recognized as causative of clinical subsets of lupus(5)
SLE is an unpredictable disease, it is characterized by alternating periods of remission and exacerbation and by a wide variety of clinical manifestations that may affect any organ. The case of our patient with SLE involved: cardiac type of lupus myopericadtitis in biventricular dysfunction with LVEF: 25%, , Normochromic normocytic anemia with positive coombs test and lymphopenia and thrombocytopenia ; lupus nephropathy satde IV ; Cerebral vasculitis.
Cytopenias are common in patients with lupus, and moderate to severe lymphopenia is associated with high disease activity and organ damage.
Up to 50% of patients with SLE have evidence of renal disease at presentation (10) Lupus end-stage kidney disease is associated with worse survival among dialysis and transplant patients.
The risk for ischemic stroke is higher in patient with SLE. Stroke affects 3–20% of patients with SLE and usually occurs within the first 5 years of the diagnosis(13,14). The main Cardiovascular diseases of SLE are valvular heart diseases associated with Libman-Sacks disease lesions, sterile vegetations, serositis associated with pericardial disease. African-American patients are at increased risk for development of myocarditis(20); low ejection fraction is detected in the majority of the patients (25)Our patient had an ejection fraction around 25% . The most characteristic valvulopathy of SLE is Libman- Sacks endocarditis (LSE), which mainly affects the left cardiac valves (22) . Non-steroidal anti-inflammatory drugs (NSAIDs) are considered as the first choice in mild cases with minimal pericardial effusion (28) Corticosteroids should be used in refractory cases with or without antimalarials. Corticosteroids in combination with immunosuppressives (25) Cyclophosphamide and intravenous immunoglobulins (IVIGs) have been shown to improve cardiac function and mortality (30), in addition to the medical treatment of Heart failure.
Conclusion: Diagnosis of SLE can be challenging and while several classification criteria have been posed, their utility in the clinical setting is still a matter of debate. Despite several agents shown to be efficacious in the treatment of SLE, the disease still poses significant morbidity and mortality risk in patients.
Systemic lupus erythematosus (SLE, or lupus) is a condition in which the immune system attacks healthy cells and tissues throughout the body, it is characterized by aberrant activity of the immune system, leading to variable clinical symptoms, The initial presentation often is like a viral syndrome, arthropathy, which may include reducible ulnar deviation, swan neck deformities, or Z-shaped thumb, is present in 2.8%–4.3% of patients(1), Cutaneous manifestations are frequent and may occur in up to 75%–80% of patients(2) , in addition to that, Systemic lupus may present in many other ways, the diagnosis should be considered when patients, particularly women of reproductive age, present with respiratory symptoms, such as cough, dyspnea, hemoptysis, or central nervous system (CNS) signs, such as headache, photophobia, or focal neurologic deficits(3), and cardiac involvement in up to 50% of cases(4)
A Moroccan 54 years old women who was a housewife and mother of two children, was admitted to the cardiological emergency room for progressive dyspnea associated with palpitations, She had a history of hyperthyroidism, and an hospitalization in the department for a pericardial effusion of great abundance punctured with withdrawal of 300cc of serohematic fluid, the remainder of the diagnostic workup had revealed lupus erythematosus for which she was put on immunosuppressant and plaquenil. On examination she was not febrile she had a heart rate at 107bpm, and a blood pressure at 130 / 80mmHg, Cardiac examination revealed a systolic mumrur at the mitral region. Pulmonary examination revealed bilateral decreased breath sounds with bilateral basal crackles. Lower limb edema was also noted, on the electrocardiogram we find a regular sinus rhythm at 107bpm, a PR fixed at 0.12sec, Normal heart axis, with negative T wave in lateral leads, the trans thoracic echocardiography found an undilated non-hypertrhophied Left ventricular (LV), seat of global hypocontractility with an ejection fraction at 25% of high filling pressures, a dilated atrial mass with a left atrium at 23cm² and a right atrium at 20cm², Moderate mitral regurgtitaion, moderate aortic regurgitation with an image of vegetation on the non-coronary cusp (Fig1), right ventricular dysfunction with pulmonary hypertension at 55mmHg and minimal circumferential pericardial effusion.
Figure 1 :
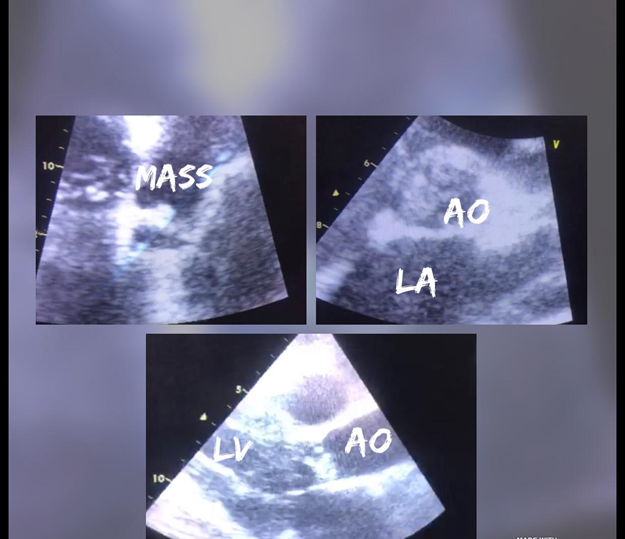
Trans thoracic echocardiography showing an image of vegetation on the non-coronary cusp
Laboratory investigations revealed bycitopenia with white blood cell count of 1.8 × 109 cells/L, platelet count of 100 × 109/L, hemoglobin 7.4 gm/dl with normal mean corpuscular volume and hematocrit, a positive Coombs test result, and high inflammatory markers (erythrocyte sedimentation
rate [ESR], 80 mm/hour [normal range, 0– 20]; C-reactive protein [CRP], 180 mg/L [normal range,0–8]; and ferritin, 323 ng/ml), infection markers positive with 6,3ng/ml of procalcitonine The patient had a renal dysfunction test result and mild derangement in liver
function enzymes. raised creatine kinase MB (CK-MB) at 16.8 ng/ml (normal range, 0.6–6.3 ng/ml) and troponin at 0.12ng/ml (normal, <0>
The blood culture showed the presence of staphylococcus aurerus, therefore the antibiotic therapy was adapted to the antibiogram, thoracic tdm demonstrated alveolar interstitial involvement and minimal pleurisy
During her hospitalization, the patient presented a constrictive chest pain radiating to the upper limbs, the electrocardiogram showed an st segment elevation in the inferior derivation the patient was loaded with 75 mg of clipidogrel and 300 mg of aspirin, and received two puffs of natispray, the course was the regression of the st segment elevation, probably related to a coronary spasm
Three days later the patient presented a sudden neurological deficit type of right hemiparesis with facial paralysis and aphasia, the emergency MRI objectified a cortical frontotemporal stroke ( Fig2) , in the acute phase, NIHSS score = 12 and the patient was thrombolysed by metalysis after elimination of contre-indications ( the valve vegetation called of libman sacks was aseptic) with monitoring of the NIHSS Score and hemodynamic constants every 15 min finally the diagnosis of vasculitis of the central nervous system (CNS) was retained with ischemic and hemorrhagic lesions in favor of lupus vasculitis of the CNS Figure 2
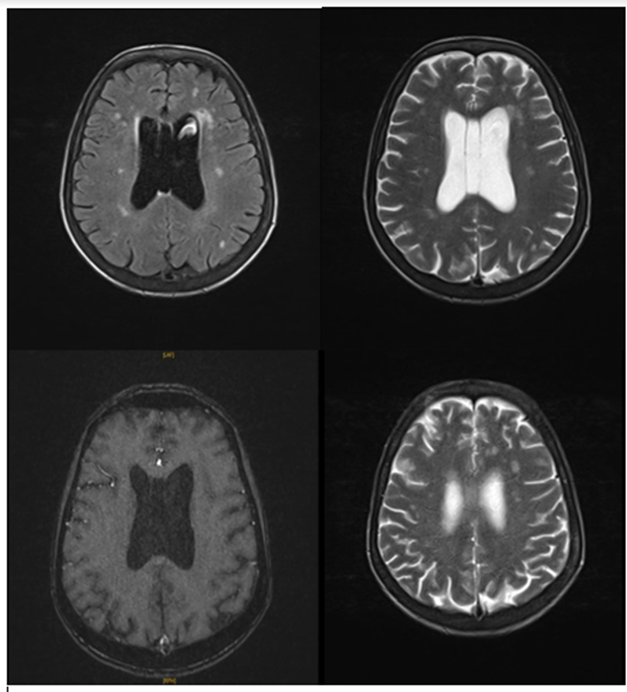
MRI image showing a cortical frontotemporal stroke
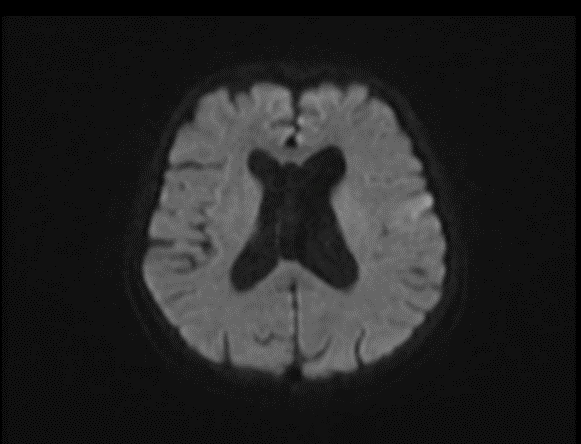
Left frontotemporal cortico-subcortical area in diffusion hyper signal.
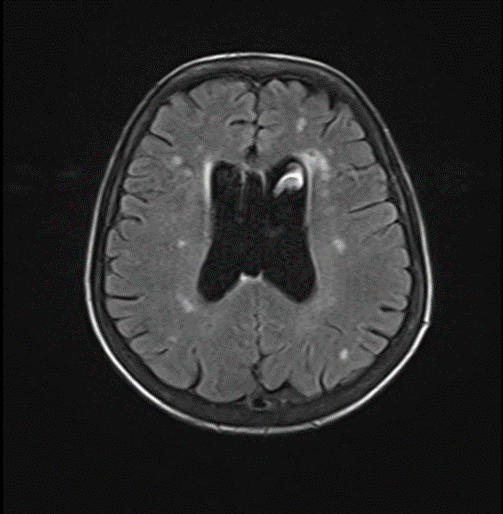
Nodular flair hyper signals of the subcortical white matter with a vascular appearance.
After multidisciplinary consultation, the patient's management consisted of:
maintaining corticosteroid therapy at a high dose of 60 mg / day with adjuvant treatment stopping plaquenil, In severe, life-threatening conditions, a bolus of solumedrol with cyclophosphamide has been indicated after management of the infectious context of endocarditis The evolution was marked by a clear improvement in the symptoms with an increase in the left ventricular ejection fraction the patient was discharged under medical treatment
Systemic lupus erythematosus (SLE) is a chronic autoimmune disorder, characterized by production of autoantibodies directed against nuclear and cytoplasmic antigens, which may affect several different organs[5]
As in many other autoimmune diseases, either the cause or the underlying pathophysiologic mechanism that triggers the autoimmune response in SLE remains largely unknown, during the following years, new autoantibodies, such as antibodies to DNA (anti-DNA), antibodies to extractable nuclear antigens (nuclear ribonucleoprotein [RNP], Sm, Ro, and La), and anticardiolipin antibodies, were recognized as causative of clinical subsets of lupus [5] Early genetic studies, driven by the observation of familial SLE aggregation and high concordance in monozygotic twins, have implicated HLA and early complement component genes [6]Genome wide association studies have identified at least 70 lupus susceptibility loci [7]
The initial presentation of lupus often mimics a viral syndrome but Systemic lupus may present in many other ways, SLE is an unpredictable disease: it is characterized by alternating periods of remission and exacerbation and by a wide variety of clinical manifestations (signs and symptoms) that may affect any organ.
we report the case of a patient with lupus erythematosus with systemic involvement:
• cardiac type of lupus myopericadtitis in biventricular dysfunction with LVEF: 25%,
• Hematologic: Normochromic normocytic anemia with positive coombs test and lymphopenia and thrombocytopenia
• Renal: with glomelus syndrome and at the puncture renal biopsy: lupus nephropathy satde IV
• Neurological: Cerebral vasculitis
About hematologic manifestations ; cytopenias are common in patients with lupus, and moderate to severe lymphopenia is associated with high disease activity and organ damage[8] Hemolytic anemia is uncommon and is usually associated with disease onset, thrombocytopenia, and African American race [9] Up to 50% of patients with SLE have evidence of renal disease at presentation [10] Lupus end-stage kidney disease is associated with worse survival among dialysis and transplant patients compared with other causes of endstage kidney disease[11]. Pleuritis is the most common respiratory SLE manifestation, affecting 30%– 50% of patients [12]. Lupus pleuritis should be diagnosed only after exclusion of other causes of pleural effusion, such as infection, pulmonary embolism, liver disease, heart disease, and cancer. Parenchymal damage is less common and may be caused by interstitial lung disease, acute pneumonitis, or bronchiolitis obliterans with organizing pneumonia.[13]
The risk for ischemic stroke is higher in patient with SLE. Stroke affects 3–20% of patients with SLE and usually occurs within the first 5 years of the diagnosis[13,14] Several mechanisms are implicated in the pathogenesis of stroke in the setting of SLE including hypercoagulable state due to antiphospholipid antibodies, cardioembolism from marantic endocarditis, enhanced atherosclerosis, and cerebral vasculitis [15]
Several studies have already demonstrated a clear association between SLE and cardiovascular disease (CVD)[16] The main CVDs of SLE are valvular heart diseases associated with Libman-Sacks disease lesions, sterile vegetations, serositis associated with pericardial disease, and venous and arterial thrombosis associated with antiphospholipid antibodies.[17] It seems that such association between SLE and CVD strictly depends on a combination of several risk factors for CVD, including dyslipidemia and, to a varying degree, hypertension, diabetes, smoking, inflammation, lipid oxidation, antiphospholipid antibodies, and renal disease and renal failure.[18] There are few case reports of acute myocarditis and heart failure as an initial SLE presentation. The therapeutic approach for myocarditis starts from standard measures with supportive care as first-line therapy, whereas anti-heart failure medications and additional treatment are prescribed on the basis of underlying etiology [19] African-American patients are at increased risk for development of myocarditis[20], In more recent post-mortem studies, after the wide use of corticosteroids in lupus therapeutics, its prevalence was estimated as 0-8%.
Typical clinical features include chest pain with tachycardia, palpitations and/or symptoms of heart failure. Our patient had palpitations and dyspnea History of recent viral infection is usually absent. Cardiac troponinsand pro-B type natriuretic peptide are often elevated [21] ECG commonly shows sinus tachycardia with widespread non-specific ST alterations and T wave changes [22] It was recently demonstrated that non-specific ST-T changes exist in 31% of newly diagnosed patients [23] Our patient presented a sinus tachycardia then a st segment elevation.
Lupus myocarditis may also present with arrythmias, conduction abnormalities and ventricular dilatation [25] low ejection fraction is detected in the majority of the patients [24]Our patient had an ejection fraction around 25
Lupus is a chronic inflammatory disorder . Diagnosis of SLE can be challenging and while several classification criteria have been posed, their utility in the clinical setting is still a matter of debate. Management of SLE is dictated by organ system involvement, and despite several agents shown to be efficacious in the treatment of SLE, the disease still poses significant morbidity and mortality risk in patients. It leads to a very poor quality of life without appropriate management.To reduce morbidity and mortality, an interprofessional team should educate and manage patients with SLE.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
