
Case Report | DOI: https://doi.org/10.31579/2694-0248/023
Department of Orthopaedics, Grant Government Medical College, Mumbai, Maharashtra, India
*Corresponding Author: Jayesh Mhatre, Department of Orthopaedics, Grant Government Medical College, Mumbai, Maharashtra, India.
Citation: Neetin Mahajan, Jayesh Mhatre, Ravikumar dadhaniya, Pritam Talukder (2022). Peculiar Periprosthetic Fracture Involving Trochanteric Region Along with Shaft of Femur in a 68-Year Male Treated with Locking Plate Fixation and Additional Augmentation with Cable – A Case Report And Review of Literature. J. Clinical Orthopedics and Trauma Care, 4(1); DOI:10.31579/2694-0248/023
Copyright: © 2022 Jayesh Mhatre, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 December 2021 | Accepted: 29 December 2021 | Published: 10 January 2022
Keywords: spinal tuberculosis; modern era; percutaneous pedicle screw
Tubercle bacilli has been known to live in symbiosis with mankind since centuries. Tubercle bacilli mainly causes pulmonary disease but extra pulmonary manifestations are fairly common with spine being the most common site
Periprosthetic fractures continue to increase in frequency. This is due, in part, to the increasing number of primary and revision arthroplasties performed annually and to the increasing age and fragility of patients with such implants [1]. All types of periprosthetic fractures can present unique and substantial treatment challenges. In each situation, the presence of an arthroplasty component either obviates the use of, or increases the difficulty of, standard fixation techniques. In addition, these fractures often occur in elderly patients with osteoporotic bone making stable fixation with traditional techniques even more problematic. The difficulty in management of periprosthetic fractures regardless of location is evidenced by the array of treatment options described in the literature without a clear consensus emerging on the most appropriate method [2]. Treatment of the most common periprosthetic fractures, those of the femoral shaft and those of the femoral supracondylar region, has focused on open reduction and internal fixation (ORIF) or revision arthroplasty procedures with or without supplementary autologous or allogeneic bone grafting [2, 3]. Most recently, treatment strategies to accelerate weight bearing have suggested benefits about mortality. Successful application of these strategies can be extrapolated to periprosthetic fractures in other anatomic locations but must also consider the fracture location relative to the arthroplasty component, the implant stability, the quality of the surrounding bone, and the patient’s medical and functional status [4, 5]. Given the predominance of low-energy injury mechanisms associated with periprosthetic fractures, associated injuries are relatively uncommon. Of course, careful assessment is required to avoid missing the occasional associated injury. The purpose of this paper was to show the outcome of peculiar Vancouver type- A1 with B2 periprosthetic femoral fracture treated with open reduction and internal fixation, using a locking compression plate and cable augmentation, in an older patient.
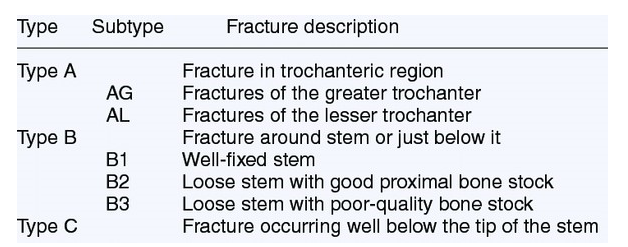
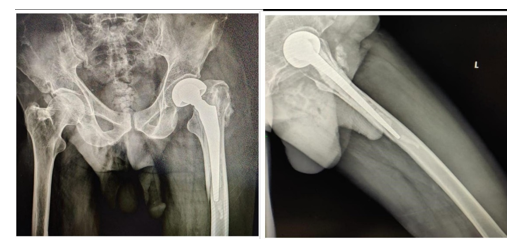
A 68-year-old male was unfortunate to sustain trauma due an accidental fall from a height. The patient referred left groin and thigh pain along with pain over his left wrist, clinical examination showed inability to actively move the legs and pain on passive movement along with pain and swelling over his left wrist, patient also had severe stiffness of his right elbow which was operated previously for distal humerus fracture in outside hospital. The radiographic studies showed a fracture of the greater trochanter and femoral shaft, in cemented hemi arthroplasty and comminuted left distal ulna and radius fracture. The bone lesions over hip were outside the classified definition with two different fracture types, Vancouver type- A1 (greater trochanter) and -B2 (periprosthetic femoral fracture) in a same occurrence (Figure 1).
Surgical procedure:
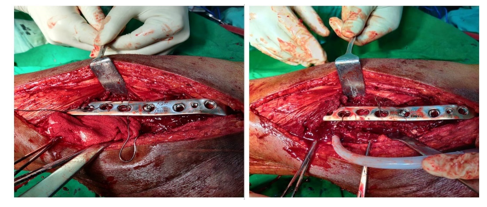
The fractures were treated with open reduction and fixation (Figure 2) with a proximal femur locking compression plate (LCP®), with a combination of 3.5 mm nonlocking and locking screws. The greater trochanter fracture was fixed with two cortical (non-locking) screws to gain bi-cortical purchase and a single locking screw to achieve uni-cortical purchase of the fragments. The femoral stem was not perforated because of the previous implant and cement in the peri-implant femoral cavity. Thus, the fractures sites were augmented with circumferential cable (three cerclage wires) in three screw position in which there was hindrance to pass screws due to pre-existing. The cerclage wire augmentation was also suited in this case due to spiral orientation of the femoral shaft fracture line; the distal plate was fixed with locking screws. The surgery was performed in the lateral decubitus without the use of a pneumatic tourniquet, and duration of surgery was 3 hours with blood loss of 300 cc. the surgery went uneventful, for left distal ulna and radius fracture suave kapandji procedure was done to salvage wrist joint function, with an attempt to reduce multiple surgeries over the wrist for which patient was non-complaint and No complications were reported in the perioperative course or during the hospitalization period. The postoperative course showed no problems with respect to the hips. The patient was submitted to an intensive rehabilitation protocol included early mobilization and walking with two crutches as patient had difficulty in holding walker due to fracture of left wrist and stiffness of his right elbow joint. At 3-months follow-up, the patient presented stable hip and the radiographs showed signs of bone union of the fractures. He reported moderate pain, and some limitation of ordinary activity. At 9-months follow-up, the patient presented an asymptomatic hip and sense of satisfaction with surgery outcome. The follow up radiograph showed union at the sites of fracture. The patient was clinically able to walk without any pain and without any external support.

Periprosthetic femoral shaft fractures are increasing in frequency because of the increasing number of patients with hip arthroplasties. The incidence of periprosthetic femur fracture after primary hip arthroplasty has been considered to be less than 1%, but has been reported to be as high as 2.3%5.A recent survivorship analysis on 6,458 primary cemented femoral hip prostheses revealed a fracture incidence of 0.8% at 5 years and 3.5% at 10 years. Another series of 354 hips in 326 patients all treated with the same uncemented, straight, collarless tapered titanium stem and followed for a mean of 17 years showed a cumulative incidence of periprosthetic fracture of 1.6% at 10 years that increased to 4.5% at 17 years [6]. The rate of fracture was low in the first 8 years after THA then increased into the second decade. In a comparison to the rate of aseptic loosening, the cumulative occurrence of periprosthetic fracture became equivalent to aseptic loosening at 17 years indicating the relative importance of periprosthetic fracture in the long term [6].
After revision arthroplasty, the incidence of periprosthetic femoral shaft fractures climbs to between 1.5% and 7.8%.The risk further increases after an increasing number of revision surgeries. The lapsed time period from an index primary hip arthroplasty to periprosthetic femur fracture averages 6.3 to 7.4 years46, and is reduced to an interval of 2.3 years after a third revision procedure. Risk factors for periprosthetic femoral shaft fractures about hip arthroplasty femoral stems are related to the age of the patient, gender, index diagnosis, presence, or absence of osteolysis, presence or absence of aseptic loosening, primary or revision status, the specific type of implant utilized, and whether cemented or non-cemented technique was utilized. Identifying risk factors can both improve patient counselling and potentially improve efforts at fracture prevention. Age, although commonly cited as a risk factor for periprosthetic femur fracture, is not clearly an independent risk factor. Coexisting medical comorbidities, osteoporosis, increased activity level, and fall risk also contribute. A recent report revealed a doubled risk of fracture in patients with higher medical comorbidities. Furthermore, the number of years after arthroplasty must be considered as each year after arthroplasty has been associated with a 1.01 additional risk ratio per year. Although a higher proportion of periprosthetic femur fractures among female patients (52% to 70%) has been reported in many series, associated osteoporosis and a higher percentage of procedures being performed in female patients makes gender less clear as an independent risk factor. Accordingly, reports that account for such biases indicate no or even reduced risk for females. The index diagnosis leading to arthroplasty may also be a risk factor with rheumatoid arthritis (RA) and arthroplasty for hip fracture each being identified as having increased risk ratios
for fracture: RA having an increased ratio of 1.56 to 2.181, and hip fracture having a reported risk ratio of 4.4. Patients with periprosthetic femur fractures have increased mortality. In multiple recent series, 7% to 18% of patients with periprosthetic fractures died within 1 year following surgical treatment.6, 18,302 In one study, this mortality rate approached that of hip fracture patients (16.5%) treated during the same time period and was significantly higher than the mortality of patients undergoing primary joint replacement (2.9%). Data from the New Zealand National Registry indicated the 6-month mortality after revision THA associated with periprosthetic fracture (7.3%) was significantly higher than in a matched cohort undergoing revision for aseptic loosening (0.9%). Although current surgical treatment guidelines, commonly suggest open reduction and internal fixation (ORIF) solely for fractures with a stable femoral stem in our patient we considered the osteosynthesis of the fractures as the most optimal treatment route [7]. The implantation of long revision hip prostheses is a prolonged and major operation for an older patient with pre-existing health condition and other co-existing injuries, which can contribute to higher risk of medical and prosthetic complications, and difficulties at early rehabilitation and physiotherapy [8, 9]. Modern internal fixation is frequently achieved with locking plates, which provide relative fracture stability, and do not impede the periosteal blood supply to the fractured bone10. Patients treated with ORIF had a significant shorter skin-to-skin surgical time and fewer perioperative blood transfusions. There were more complications reported in the revision arthroplasty cohort compared to patients that were treated with ORIF [11]. In the other hand, open reduction and internal fixation utilizing locking compression plates (LCP®) might be an effective treatment with a reduced surgical time and less complex procedure in a typically elderly patient with multiple comorbidities. Rigid fixation for periprosthetic femoral fractures with screws and plates is challenging due to interference of a pre-existing femoral stem [11]. In our case, it was not possible to perforate the implant, and bi-cortical fixation of the stem was obtained cerclage wire passing through screw holes of the locking plate. The distal part of the plate was fixed with at least eight cortices as recommended by other authors. encerclage wires associated with metallic plate can reduces stress shielding, increases the probability of fracture consolidation, makes the system more stable, reduces complications, and improves patient quality of life due to a shorter functional recovery, compared to internal fixation with a simple plate.
In older patient with multiple injuries where early mobilization is of essence along with definitive fixation, the use of locking plates is a valid treatment of atypical Vancouver A1-B2 periprosthetic femoral fracture combination. The key-points to a successful outcome are anatomical fracture reduction, stable fixation, early mobilisation and appropriate implant, and the preservation of the hip joint avoiding the risk of prosthesis dislocation. Our patient showed favourable outcome and we conclude that in similar cases, combination construct which was used by us can provide optimal results.
Conflicts of interest
All authors declare that there are not any competing interests.
Funding
There is no source of funding.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
