
Research Article | DOI: https://doi.org/10.31579/2641-0419/210
1 Department of cardiology, Nepal Mediciti, Lalitpur, Nepal
*Corresponding Author: Ranjit Sharma Nepal Mediciti hospital, 44700 Bhaisepati, Lalitpur, Nepal.
Citation: Ranjit Sharma, Anish Hirachan, Milan Gautam, (2021) Patterns of Coronary Artery lesion in a Patient with Chronic Obstructive Pulmonary Disease, Presenting with an Acute Coronary Syndrome. J. Clinical Cardiology and Cardiovascular Interventions, 4(14); Doi:10.31579/2641-0419/210
Copyright: © 2021 Ranjit Kumar Sharma, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 August 2021 | Accepted: 16 August 2021 | Published: 20 August 2021
Keywords: acute coronary syndrome; pulmonary disease; chronic obstructive pulmonary disease
Background: This study was designed to evaluate the patterns of coronary artery disease in patients with chronic obstructive pulmonary disease (COPD) presenting with the acute coronary syndrome (ACS).
Methods: This was a prospective, observational study, conducted on 69 patients with chronic obstructive pulmonary disease, presenting with acute coronary syndrome undergoing coronary angiogram from September 2017 to March 2021. All patients had undergone coronary angiogram; severity and morphology of lesion as well as the severity of calcium were analyzed.
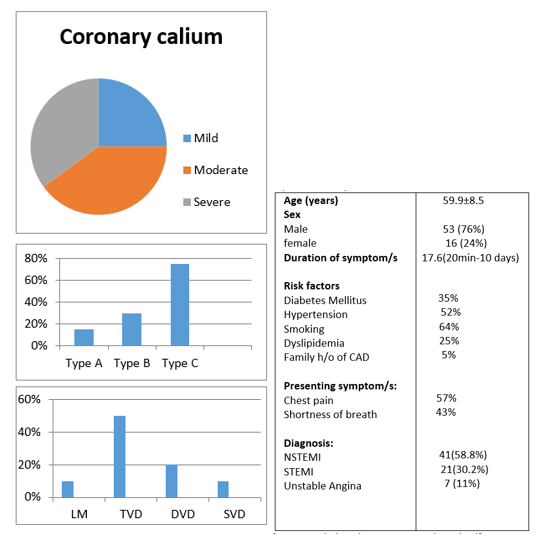
Results: The study showed that 69 patients with COPD who presented with ACS, 58.8% of patients were presented with NSTEMI, 30.2% STEMI and Unstable angina 11%. The average time of presentation after the onset of the symptom was 17.6 hours. 64% of patients were a smoker. Coronary involvement 10% of patients had LM, 50% TVD, 30% DVD, and 10% had SVD. Type a coronary lesion was seen in 5%, Type B in 20%, and Type C in 75% of patients. Mild Coronary calcium was seen in 25%. Moderate calcium was in 40% and severe calcium in 35%.
Conclusions: COPD patients presenting with ACS, associated with increased severity of coronary calcium and coronary lesions.
Acute coronary syndromes (ACS) and chronic obstructive pulmonary disease (COPD) are leading causes of death and disability worldwide [1]. World Health Organization data show that around 17.7 million cardiovascular disease deaths worldwide in 2015 (31% of all-cause mortality), of whom 7.4 million were due to coronary artery disease [2]. At the same time, COPD is the fourth leading cause of mortality globally, affecting more than 210 million people [3]. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) defines COPD as a disease characterized by persistent and usually progressive airflow [4]. Several pathological mechanisms underlie the relationship between COPD and ischemic heart disease [5]. First, COPD and ischemic heart disease share common risk factors, of which smoking and increasing age are most important [6]. Moreover, the prevalence of other cardiovascular risk factors such as diabetes and hypertension seems to be higher in COPD patients compared to healthy individuals [7].
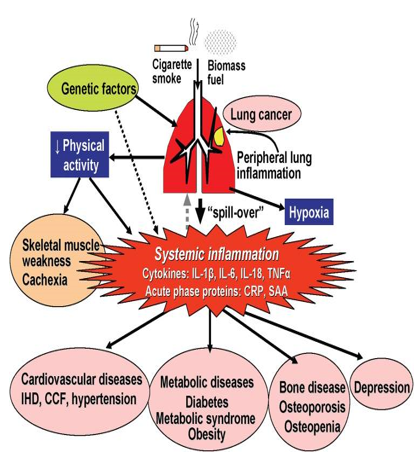
Atherosclerosis is a lipid-related chronic inflammatory disease in which immune mechanisms play a pivotal role [8]. The lesions are filled with large numbers of immune cells. Similarly, chronic obstructive pulmonary disease (COPD) is characterized by an intense inflammatory process in the airways, parenchyma, and pulmonary vasculature. Systemic inflammation, because it plays a central role in the pathogenesis of atherosclerosis and COPD, could be a pathophysiological link between them [9]. However, there is still no consensus in the literature because COPD was considered to be a predictor of CAD and increased cardiovascular risk in some studies, whereas other studies did not [10]. However, the open question is whether COPD and cardiac disorders are linked beyond these risk factors. Altered, persistent, and low-grade systemic inflammation likely plays a role: raised inflammatory markers, such as C-reactive protein and different cytokines, have been repeatedly related to atherosclerosis and subsequent ischemic heart disease (IHD), HF, and AF [11]. Such inflammatory markers are raised in many patients with COPD. Furthermore, exacerbation frequency in COPD relates to higher levels of inflammation and a higher risk of MI [12]. The most established hypothesis explaining the interaction of COPD and ACS is the inflammation model. The inflammation model hypothesizes that the local airway inflammation in COPD "spills over" into the systemic circulation and the coronary arteries, promoting coronary plaque development, perhaps explaining why CAD is highly prevalent in COPD [13]. Another potential contributor to the association between COPD and ACS is the dysregulation and over-activation of the sympathetic nervous system. COPD patient’s exhibit reduced heart rate variability, increased norepinephrine turnover, and increased plasma levels of renin, all signs of increased sympathetic nervous system activity, also known to be harmful in CAD [14].
It is a retrospective, single-center study, performed at Nepal Mediciti Hospital, Nepal. All the COPD patients who presented with acute coronary syndrome from September 2017 to March 2021 were enrolled in this study. All 69 patients with COPD, presenting an acute coronary syndrome were taken to the catheterization lab for a coronary angiogram. The severity and morphology of the lesion as well as severity of calcium were analyzed. Calcification was identified as readily apparent radiopacities within the vascular wall at the site of the stenosis and was classified as none/mild, moderate (radiopacities noted only during the cardiac cycle before contrast injection), and severe (radiopacities noted without cardiac motion before contrast injection generally compromising both sides of the arterial lumen) [15].ACC/AHA classification of coronary lesions is a system used to classify coronary arterial calcific plaque burden. It is classified as [16]
1. Discrete (<10>2.Concentric 3.Nonangulated segment <45>4.Smooth contour 5.little or no calcification 6.less than totally occlusive 7. Not ostial in location 8. No major branch involvement 9.Absence of thrombus
1. Tubular (10-20 mm) 2.Eccentric 3.moderate tortuosity of proximal segment 4.Moderately angulated, 45-90º 5.Irregular contour 6.Moderate to heavy calcification 7.Ostial in location.
8. Bifurcation lesions requiring double guidewires 9.Some thrombus present 10. This can be subclassified into two subcategories
A total of 69 COPD patients presenting with acute coronary syndrome were included in the study. The average age was 59.9 ± 8.5 with the youngest being 32 years and the oldest being 88 years old. Most of the patients were male 76%.
The commonest symptom was chest pain 57% followed by shortness of breath in 43%. The diagnosis was made base on a clinical symptom, electrocardiography findings, and cardiac biomarkers. Most of the patients 41(58.8%), were presented with NSTMI, followed by 21(30.2%) STEMI and 7(11 %) Unstable angina. Among the risk factors, smoking was the commonest and found in 64% of patients followed by hypertension 52% and diabetic 53%. Angiography showed 10% of patients had LM, 50% TVD, 30% DVD, and 10% of patients had SVD. ACC/AHA classification of coronary lesions is a system used to classify coronary arterial calcific plaque burden. Based on this classification Type a coronary lesion was seen in 5%, Type B in 20%, and Type C in 75% of patients. Based on angiographic findings coronary calcium was classified into mild, moderate, and severe. Mild Coronary calcium was seen in 25%. Moderate calcium was in 40% and severe calcium in 35%.
Several pathological mechanisms underlie the relationship between COPD and ischemic heart disease. ACS and COPD have shared risk factors that may contribute substantially to the relationship between the diseases; the most important are smoking and high age. Even passive smoking increases the risks of both ACS and COPD. There is substantial evidence that inflammation plays a key role in the development of both COPD and CAD.
Igor LM et al found that in patients with suspected CAD, comorbid COPD was associated with increased severity and extent of coronary lesions, calcific plaques, and elevated calcium score independent of the established risk factors for CAD (4). In addition, the more severe the COPD, the greater the severity of coronary lesions and calcification present. Roversi et al reported that 88.1% of the patients had coronary lesions (CAD), and 71.3% of obstructive coronary lesions (≥50% of the vessel) occurred in patients with COPD. The prevalence of proven CAD in patients with COPD is known and ranges from 47% to 60% [17]. Similar findings were found in our study and showed that most of the patients presented with NSTEMI about 58.8% and with multivessel involvement. Tripel vessel disease was almost 50%.
Baty F et al reported that the frequent occurrence of stenosis, severe lesions, and markedly calcified coronary plaques, especially in the global Initiative for Obstructive Lung Disease stages III group and also reinforces that the inflammatory processes of COPD do not participate only in the formation of atherosclerotic plaques but also in their progression [18,19]. Similar findings were found in our study Type A coronary lesion was seen in 5%, Type B in 20%, and Type C in 75% of patients.
Williams et al found higher Coronary calcium in COPD patients and associated dyspnea and reduced exercise capacity, data coincident with our study where patients with COPD had higher and more frequent Coronary calcium [20]. In our study, Severe calcium was found in 35% and moderate in 40%.
Study limitations
There are several limitations of this study. First, it is a single-center retrospective study. Second IVUS and OCT were not used to interrogate the coronary lesion.
In COPD patients presented with ACS is associated with increased severity and extent of coronary lesions, calcific plaques, and elevated calcium scores, independent of the traditional risk factors for established CAD. The more advanced the COPD, the greater the coronary lesions and calcification.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
