
Research Article | DOI: https://doi.org/10.31579/2641-0419/143Copyright
1Department of Paediatrics, Usmanu Danfodiyo University Teaching Hospital, Sokoto
2Department of Surgery, Usmanu Danfodiyo University Teaching Hospital, Sokoto
*Corresponding Author: Isezuo KO, Department of Paediatrics, Usmanu Danfodiyo University Teaching Hospital, Sokoto
Citation: Isezuo KO., Sani UM., Waziri UM., Garba BI., Adamu A., et al (2021) Pattern of Congenital Heart Diseases in Children with Congenital Malformations: An Echocardiographic study from a Tertiary Health facility in Sokoto, Nigeria. J. Clinical Cardiology and Cardiovascular Interventions, 4(7); Doi:10.31579/2641-0419/143
Copyright: © 2021 Isezuo KO, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 12 February 2021 | Accepted: 30 March 2021 | Published: 08 April 2021
Keywords: congenital malformations; congenital heart disease; echocardiography; pattern
Background: Children with congenital malformations (CM) may have congenital heart diseases (CHDs) which may be initially asymptomatic. These need to be recognised and managed early in order to reduce unnecessary morbidity in affected patients. We report the pattern of CHDs in children with congenital malformations who had echocardiography over a one year period in UDUTH, Sokoto.
Materials and Methods: A cross-sectional study carried out in the Paediatric Cardiology Unit from 1st January to 31st December 2019. Children presenting with CM were recruited and had echocardiagraphic screening for CHDs. Data were analysed with SPSS 23 version. Statistical significance was taken at p < 0.05.
Results: 81 children were seen with CM, comprising 42 females and 39 males (M:F=0.93:1); age range of 2 days to 13 years. Most frequent malformationswere anorectal malformations (ARM) in 28 (34.6%), Down syndrome in 17 (21.0%), multiple CM 10 (8.1%) and ocular abnormalities in 4 (4.9%). Thirty two (39.5%) of the patients with CM were diagnosed with CHD, out of which 24 (29.6%) had cardiac murmur. Most frequent CHD was atrioventricular septal defect in 9 (28.1%) followed by ventricular septal defect in 8 (25.0%) and patent arterial duct in 4 (12.5%). CHDs were found in all (100%) those with ocular abnormalities, in 76.5% of Down syndrome and in 14.3% of patients with ARM. Presence of murmur was significantly associated with CHD (χ2=18.0; p=0.001; OR=8.2; 95% C.1=2.8 – 24.1).
Conclusion: Congenital malformations, particularly Down syndrome and ocular abnormalities, are significantly associated with CHDs. Cardiac murmurs were suggestive of CHD in children with congenital malformations.
Congenital malformations (CM) are structural abnormalities or conditions that arise in the fetus conesquent to preconceptional and intragestational factors and are present at birth, but can also be diagnosed prenatally or much later in life. [1] Congenital malformations are permanent changes produced by an intrinsic abnormality in the development of a body structure prenatally. [1] Congenital malformations can potentially affect the childs health, development and survival because they can be associated with abnormalities in many body systems including congenital heart disease (CHD). [2]
Congenital heart diseases (CHD) consist of defects of the cardiac architecture which interfere with the venous drainage, septation of the cardiac segments and their sequences and regular function of the valve apparatuses. [3]
Some Congenital malformations may require emergent surgical intervention and the presence of a comorbid cardiac defect may be an anaesthetic risk. [2]Such risks may warrant delay of surgical inteventions if echocardiography is not available to rule out significant CHD. [4]These need to be recognised and managed early in order to reduce unnecessary morbidity in affected patients.
Screening such children for CHD is therefore important and those conditions more frequently associated with CHD must be recognized clinically by presence or absence of symptoms and signs of cardiac disease. The aim of the study was to ascertain the proportion and types of CHD in children with external Congenital malformations and compare with their cardiac symptoms.
Materials and Methods
This study was carried out in the Paediatric Cardiology Unit, Paediatrics department of Usmanu Danfodiyo University Teaching Hospital (UDUTH), Sokoto which is the major tertiary health facility in Sokoto State. The unit receives referrals of children with cardiac conditions from other units within the department and hospital as well as other health facilities within and outside the state and neighbouring border countries in the West African sub-region.
It was a cross-sectional study of children aged 15 years and below presenting to the Paediatric Cardiology Unit between January 2019 to December 2019. Children presenting with external Congenital malformations were recruited and had echocardiagraphic screening for CHDs.
Sampling method: Universal sampling method was used.
Inclusion criteria: All children presenting with major external congenital malformations that gave informed consent shall be recruited.
Exclusion criteria: Those who were very ill, limiting full examination for congenital and screening echo.
Case definition: Visible external congenital malformations affecting 1 or more systems OR >2 minor malformations as defined in the CDC checklist of surveillance of birth defects. [5]
The specific type of Congenital malformations which was the reason for their echo request was additionally confirmed before echocardiography by a complete physical examination.
Echocardiography: Cardiac diagnosis was done using two- dimensional and Doppler transthoracic echocardiography (TTE). Patients were examined in the supine and left lateral positions. The younger ones who were not cooperative were distracted with colourful toys and other techniques with the participation of the parents. The heart was examined through the standard parasternal, apical, subcostal, and suprasternal views using the Hewlett Packard Sonos 5500 echocardiography machine (Bloomfield CT 06002, USA) and 8MHz transducer.
The specific echocardiographic diagnosis was confirmed by 2 or 3 independent echocardiographers with complete agreement in all the cases.
Data Collection: A structured proforma was used to collect their demographic characteristics including age, gender, social status of the parents. The cardiac diagnosis at echocardiography was also recorded.
Ethical issues: Ethical approval for the study was obtained from the Ethics and Research Committee of Usmanu Danfodiyo University Teaching Hospital, Sokoto (UDUTH/HREC/2021/1023/V1) while consent was obtained from the parents of the children. Confidentiality was maintained as well as privacy.
All relevant data were entered into a proforma sheet then analyzed using SPSS statistical software version 23. Quantitative data were expressed as means and standard deviation while categorical variables were expressed as proportions. Chi-square or where necessary, Fisher’s Exact test, was used to test for statistical significance. A p-value of <0.05 was considered statistically significant.
Eighty-one children were seen with external Congenital malformations, comprising 42 females and 39 males (M:F= 0.93:1); age range of 2 days to 13 years.
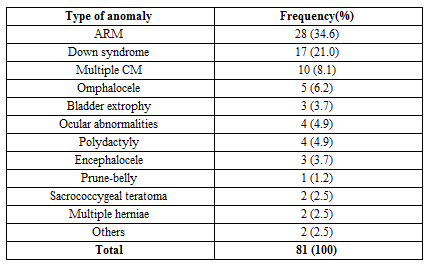
Most frequent malformations were anorectal malformations (ARM) in 28 (34.6%), Down syndrome in 17 (21.0%), multiple anomalies 10 (8.1%), isolated anomalies 22 (27.1%) and ocular abnormalities (cataract) in 4 (4.9%) (Table 1).
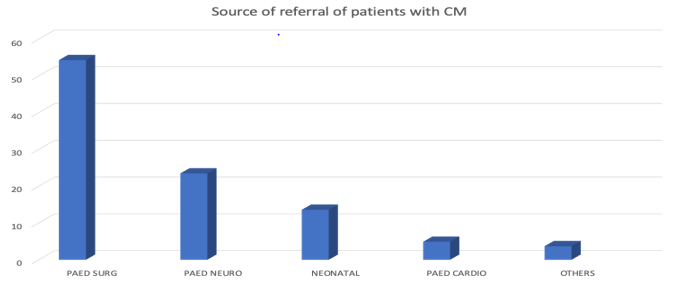
The source of referral of the cases of CM was mainly from the Paediatric surgical unit, followed by Paediatric neurology and Neonatalogy. (Figure 1)
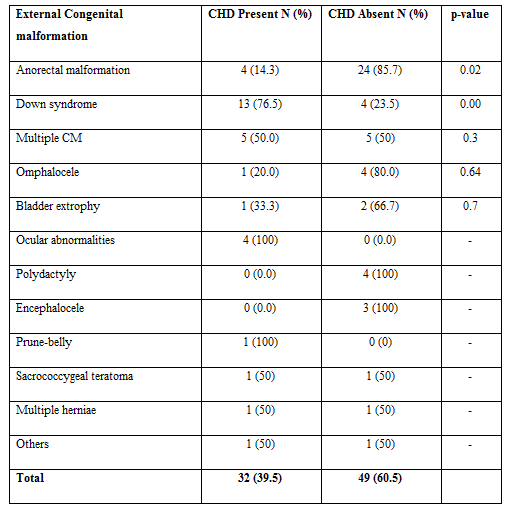
Of the 81 patients with CM, 32 (39.5%)were diagnosed with CHD while 49 (60.5%) did not have CHD. CHDs were found in all (100%) those with ocular abnormalities,in 76.5% of Down syndrome and in 14.3% of patients with ARM. Table 2 shows there was a high association of CM with CHD with ocular abnormalities and Down syndrome. For those with multiple CM, 50% had CHD, while CHD was completely absent in polydactyly and encephalocele.
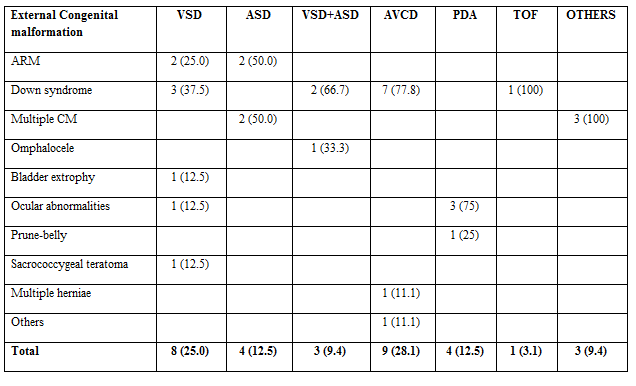
Most frequent CHD was atrioventricular septal defect9 (28.1%) followed by ventricular septal defect 8 (25.0%) and patent arterial duct 4 (12.5%). AVSD occurred predominantly in Down syndrome while PDA occurred predominantly in those with ocular abnormalities. Majority had acyanotic CHD (87.5%) while 4 had cyanotic CHD (12.5%) of which 3 had multiple CM.

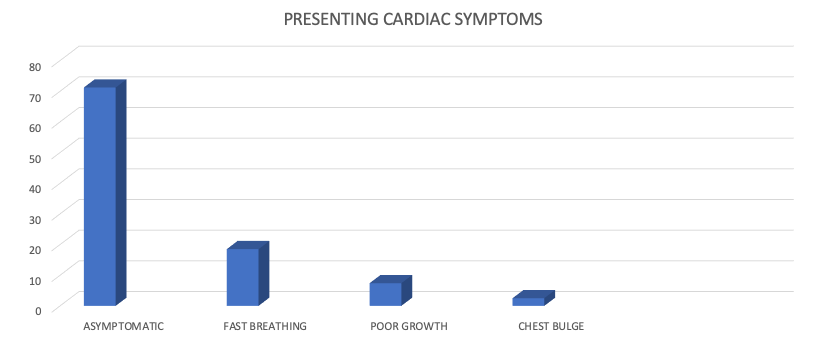
Majority 22 (68.8%) of those with CHD were asymptomatic while other symptoms detected were fast breathing 6 (18.8%), poor growth 3 (9.3%) and chest bulge 1 (3.1%).
The presence of cardiac murmur on auscultation was also examined for associationwith eventual diagnosis of CHD. Out of the total of 81 patients with CM, 24 (29.6%) had cardiac murmur. Presence of murmur was significantly associated with CHD (χ2= 18.0; p=0.001; OR=8.2; 95% C.1=2.8 – 24.1) (Table 4).
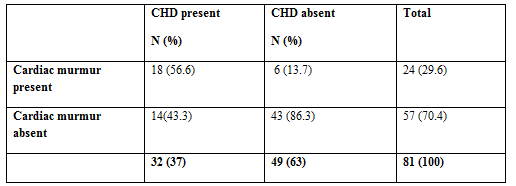
Table 2: Frequency of occurrence CHD in different CM
Most frequent CHD was atrioventricular septal defect9 (28.1%) followed by ventricular septal defect 8 (25.0%) and patent arterial duct 4 (12.5%). AVSD occurred predominantly in Down syndrome while PDA occurred predominantly in those with ocular abnormalities. Majority had acyanotic CHD (87.5%) while 4 had cyanotic CHD (12.5%) of which 3 had multiple CM.

Table 3: Showing type of CHD seen in the different types of external CM
ARM was the commonest CM presenting for echocardiography in this study and this is consistent with a report by Lawal which was an overview of studies from all over Africa where ARM has been documented to be the most common structural occuring in children. [6] This is unlike the finding in a similar echocardiographic study by Oyati et al from Zaria, Nigeria, [7] located within the same northwestern region as the study area, where cleft lip and palate was the commonest surgical anomaly (38.3%), followed by ano-rectal malformation (26.7%). In this study, cleft lip was seen only in one child co-existing with other multiple major anomalies. The relative paucity of facial clefts among our cohort could be due to the presence of a facility in the study area which is specifically dedicated to catering for congenital and acquired facial clefts. [8] Another study by Ekure [9] showed that Down syndrome as the commonest CM presenting for echocardiography accounting for more than half (53.4%) of those presenting with CM while in this study Down syndrome was the 2nd commonest indication.
CHD was detected in 39.5% of our cases similar to 35% reported by Oyati. [7] The study by Ekure also showed a much higher figure of 73% having CHD as most of their patient cohort there had recognizable syndromes associated with CHD. [9] The commonest anomaly in our study was AVSD while in the Zaria and Lagos studies, [7,9] it was ASD and VSD respectively reflecting probably the different proportions of the anomalies.
The incidence of CHD in ARM, the commonest CM in this study appeared low (14.3%) compared to other reports like that of Kamal and Azhar [10] who reported the occurrence of CHD in 24.6% patients and Hashemizadeh [10]from Turkey reported 23.7% incidence of CHD among cases of ARM. Two studies from Iran revealed similar higher incidence rate of CHD of 30% and 50.4% in newborns with ARM. [11,12] Half of the patients with ARM in this study had ASD which has also been reported as the most prevalent CHD in those with ARM in other studies as they usually have less of complex CHD. [11,12] This is of import as opined by Nasr et al who examined records to ascertain if routine echocardiography is necessary for all neonates with some CM or if appropriate patients who are not at risk could be selected without preoperative echocardiography. [13]
The commonest CHD in those with DS was AVSD which is seen associated with this anomaly in several reports. [14-16] Also, all those with ocular anomalies had CHD which wasmainly PDA which could be due to genetic causes. [17-18] Two of the ocular anomalies were cataracts which is associated with Congenital rubella syndrome of which the cardiac component is PDA. A study in Italy has reported significant association between ocular anomalies and CHD. [19]
Although, majority of the patients seen were asymptomatic, those who had detectable cardiac murmurs eventually turned out positive for CHD. However, some did not also have any murmur and were diagnosed with complex defects. Some authors have opined for routine screening for all those with CM due to observations of increased morbidity and mortality with combined malformations, [20,21] while others suggest that in emergency conditions, pre-operative echo may not be absolute if not available especially in a CM not commonly associated with CHD. [4]
Congenital malformations, particularly Down syndrome and ocular abnormalities, are commonly associated with CHDs. ARM has a relatively low incidence of CHD, which were not complex defects. Cardiac murmurs were suggestive of CHD in children with congenital malformations. However, due to significant number who were asymptomatic that were still diagnosed with CHD, it is importance that all children with CM should be screened for CHD.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
