
Research | DOI: https://doi.org/10.31579/2640-1053/120
19-D, Transymuna colony, Rambagh, Agra (U.P).
*Corresponding Author: Surabhi Gupta, 19-D, Transymuna colony, Rambagh, Agra (U.P)
Citation: Surabhi Gupta. (2022). Pattern of Bacterial Infections in Cancer Patients -Experience from a Tertiary Cancer Center. Cancer Research and Cellular Therapeutics. 6(4); Doi:10.31579/2640-1053/120
Copyright: © 2022 Surabhi Gupta, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 16 May 2022 | Accepted: 26 May 2022 | Published: 06 June 2022
Keywords: bacterial infections; cancer patients; tertiary cancer center
It is a general belief that cancer patients are more prone to infections, particularly bacterial infections. Firstly, disease itself present an immuno-compromised status, secondarily chemotherapy and radiotherapy further suppress the immunity level which is further overburden by poor nutritional state and poor hygienic conditions in these patients. With the invent of better diagnostic modalities and many technological advancement in treatment delivery, the mortality rates have fallen over the past years, but infection remains a primary or associated cause of death, with bacteria most commonly accounting for infection-associated mortality, followed by fungi.
The management of the infections is based on the use of appropriate empirical antimicrobial therapeutic agents with a comprehensive understanding of pathogens which are the commonly encountered in cancer patients in day-to-day practice and also understanding of antibiotic sensitivity patterns. Though the empirical use of antibiotics has reduced the mortality in patients but has also led to the menace of multidrug-resistant bacteria.
It is a general belief that cancer patients are more prone to infections, particularly bacterial infections. Firstly, disease itself present an immuno-compromised status, secondarily chemotherapy and radiotherapy further suppress the immunity level which is further overburden by poor nutritional state and poor hygienic conditions in these patients. With the invent of better diagnostic modalities and many technological advancement in treatment delivery, the mortality rates have fallen over the past years, but infection remains a primary or associated cause of death, with bacteria most commonly accounting for infection-associated mortality, followed by fungi [1].
The management of the infections is based on the use of appropriate empirical antimicrobial therapeutic agents with a comprehensive understanding of pathogens which are the commonly encountered in cancer patients in day-to-day practice and also understanding of antibiotic sensitivity patterns. Though the empirical use of antibiotics has reduced the mortality in patients but has also led to the menace of multidrug-resistant bacteria [2].
Multidrug-resistant bacteria are commonly encountered among immuno-compromised patients. So it is necessary to be aware with the ever changing spectrum of infection and sensitivity pattern so that judicial and effective use of these drugs can be done with successful control of infections among cancer patients.
This present study aims to evaluate the common types of bacterial infections and their antibiotic susceptibility spectrum in cancer patients undergoing chemotherapy for solid tumors.
This study was undertaken to monitor the types of pathogens commonly found in cancer patients undergoing anticancer treatment and their antibiotic sensitivity and resistance patterns.
This study was conducted in department of radiation oncology and total 100 patients, who were admitted for chemotherapy in department from 1 may 2021 to 31st July 2021 were enrolled. Different samples were taken according to patient’s presentation. These samples were collected in our department and were sent to microbiology department for culture and sensitivity. Demographic and clinical data of patients were collected including age, sex, site of malignancy, site of infection, type of bacterial isolates, antibiotic sensitivity pattern and details of anthropometry, comorbidities, haematological examination results, and any procedures (urinary catheterization, central or peripheral IV cannulation, endotracheal intubation, and ventilator management) were collected. The collected data were entered into Microsoft Excel and analyzed and results obtained are represented in the form of graphs and tables.
Inclusion criteria
1. Histopathological confirmed case of solid malignancy
2. Patients undergoing only chemotherapy
3. Age > 18 yrs.
Exclusion criteria
1. Patients receiving immunotherapy or radiotherapy
2. Patient with any immunosuppressive status
Microbiological investigations
The clinical samples like pus, urine, vaginal swab, sputum, blood and stool received from suspected cases of infection and accordingly were stained for microscopical examination and inoculated onto blood agar, chocolate agar and macConkey’s agar (HiMedia) and incubated aerobically at 35 ᵒC for 24 to 48 hrs. Blood Culture is done by FX 40 (Bactec). Positive cultures were sub cultured onto blood agar, chocolate agar and Mac Conkey’s agar and incubated aerobically at 350C for 24hrs. Identification of the bacterial growth and antimicrobial susceptibility testing of the isolates were interpreted as sensitive, resistant and Intermediate using the latest/ Clinical and Laboratory Standard Institute (CLSI) Guidelines. Antibiotics used for Gram Positive Bacteria were Penicillin-G, Amoxicillin, Carbenicillin, Ticarcillin, Cefoxitin, Amoxy-clavulanic Acid, Ampicillin-Sulbactam, Piperacillin/Tazobactam, Cefepime, Cefuroxime, Cefaclor, Cefodoxime, Ceftriaxone, Chloramphenicol, Ciprofloxacin, Levofloxacin, Ofloxacin, Erythromycin, Azithromycin, Clarithromycin, Doxycycline, Tetracycline, Clindamycin, Teicoplanin, Cotrimoxazole, Linezolid, Vancomycin , and for Gram Negative Bacteria are Ampicillin, Piperacillin/Tazobactam, Amoxicillin/ Clavulanic Acid, Ampicillin Sulbactam, Cephalothin, Cefaclor, Cefpodoxime, Ceftriaxone/Sulbctam, Cefotaxime, Ceftazidime, Cefepime, Cefoperazone/Salbactam, Doxycycline, Tetracycline, Nitrofurantoin (urine), Ciprofloxacin, Levofloxacin, Moxifloxacin, Chloramphenicol, Amikacin, Gentamicin, Cotrimoxazole, Meropenem, Imipenem and for Pseudomonas are Amikacin, Meropenem, Piperacillin, Piperacillin/Tazobactam, Cefepime, Tobramycin, Cefftazidime, Polymyxin-B, Aztreonam, Ciproflaxacin, Levofloxacin, Gemifloxacin . In urine sample we are using CLED Agar. In vaginal swab, the first swab is used to make a smear on clean grease-free glass slide for bacterial differentiation by Gram-Stain Examination and the second swab is used for the bacterial culture on blood agar and Mac Conkey’s agar.
A total 100 admitted patient were enrolled for the study. Data were collected prospectively and analyzed. Following results were obtained.
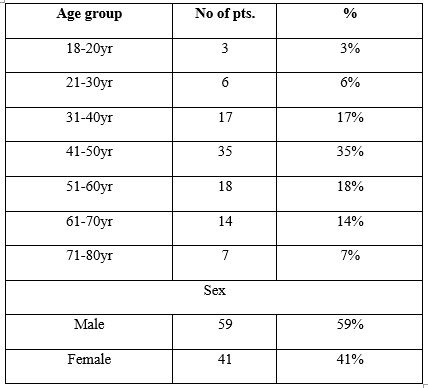
Figure no.1
Only patients of solid malignancies were taken in this study. Maximum number of patients belonged to head and neck cancer (53%) followed by carcinoma cervix (23%) and carcinoma breast (8%).
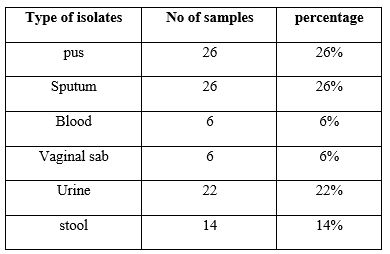
Figure No.2
Overall, 91% organism were gram negative bacteria.
Infection is a common complication of cancer and cancer treatment and certain types can be life-threatening if not found and treated early several factors increase the risk of infection in patients with solid tumors, and the presence of multiple risk factors in the same patient is not uncommon. These include obstruction (most often caused by progression of the tumor), disruption of natural anatomic barriers such as the skin and mucosal surfaces. Infection is commonly encountered among cancer patients, leading to disturbances in the treatment regimen, prolonged hospitalization, increased cost of health care, and reduced survival. Important infections like bloodstream infections and pneumonia were major contributors to mortality in oncology patients. The previous studies have reported 36% mortality due to sepsis in cancer patients [3]. Pneumonia, sepsis, influenza, and parasitic infections have been documented among the deceased cancer patients [4]. In our study, most common site of infections seen was head and neck cancer cases (53%) followed by carcinoma cervix cases (23%), this may be attributed to poor oral, skin and genital hygiene. Carcinoma breast patients (8%) presented as large fungating mass. Carcinoma lung cases (5%) presented with lower respiratory tract infection.Maximum numbers of patients (35%) were of 41-50 years age group with male predominance. In our study, 91% of the infections were associated with gram-negative organisms and only 9% were due to gram positive organisms. It is in contrast to the earlier reports from developed countries, where the incidence of infections caused by gram-positive bacteria is higher. In most of the studies from developed countries, around 70% of the infections are caused by gram-positive bacteria [5]. On the contrary, most studies conducted in developing countries have recorded that majority of infections were caused by gram-negative organisms [6]. Epidemiology of infections in cancer patients has changed across the globe overtime. In the study conducted by Siddaiahgari et al., Pseudomonas spp. was the most common causative organism of bloodstream infection, causing 36% of the bloodstream infections. E. coli accounted for 46.3% of the urinary tract infection. Characterized Gram-negative bacteria have predominated the scene as a major cause of infections in cancer patients in the last 20 years across the globe in many countries. Among gram-negative bacteria, Klebsiella pneumoniae, Pseudomonas aeruginosa, and Acinetobacter baumannii have been increasingly associated with cancer patients [7]. The findings of a study conducted by Yadegarynia et al. in Texas showed that pneumonia was the most common infection seen in both the groups of patients with solid organ tumours (26%), as well as in patients with haematological malignancies (38%) [8]. In our study, soft tissue and skin infections (26%) and respiratory tract infections (26%) were more common compared from other studies other studies. The epidemiology of most of these infections is changing with resistant organisms [MRSA, Pseudomonas aeruginosa, extended spectrum beta-lactamase (ESBL)-producing organisms] being isolated more often than in the past [9]. A study done in New Delhi by Batra et al. noted 80% ESBL production rates among the gram-negative bugs [10]. In our study also, among gram negative bacteria ESBL status was known in 55% of growth, out of which ESBL producing microbes were 69.09%, while ESBL non-producing were 30.9%In gram positive bacterias, 33.33% were MRSA type. In a study conducted by Sirisharani Siddaiahgari, the overall rank order of the most common pathogens was Pseudomonas spp. (26.2%) > Enterococcus spp. (11.66%) > S. aureus (11.44%) > E. coli (11.34%) > Klebsiella spp. (10.59%) >Acinetobacter spp. (9.95%) > Coagulase-negative Staphylococcus (CoNS) (6.52%)> Streptococcus spp. (3.42%) > Enterobacter spp. (3.1%) > Burkholderia spp. (2.35%) [7]. This was not the case in our study, where rank order was Klebsiella spp. (41%) > Escherichia coli (38%) >Pseudomonas spp. (12%) > > Staphylococcus aureus (9%). In the study conducted by Siddaiahgari et al., Pseudomonas spp. was the most common causative organism of bloodstream infection, causing 36% of the bloodstream infections. E. coli accounted for 46.3% of the urinary tract[7]. In our study, klabesilla pneumoniae was the most common microbes in pus sample (37.03%), stool (50%) and sputum samples (57.69%). E. coli was common organism in urine (66.66%), vaginal swab (57.14%) and blood culture (40%). Pseudomonas auregenoa was commonly found in sputum(26.08%) ,pus (18.51%)and stool (7.14%),while staphylococcus aureus was seen in vaginal swab(14.28%) ,pus (11.11%) and sputum (8.69%). In our study, we also correlated malignancy site wise organism correlation and found that Head and neck carcinoma patients were harboring klebsiella pneumoniae (49.05%) commonest followed by Pseudomonas aeruginosa (20.75%). In Ca breast pattern was klebsella pneumoniae (50%) followed by staphylococcus aureus (25%). In ca cervix case-E. coli (69.56%)> klebsiella pneumoniae (26.08%).In ca lung cases-E coli and klebsiella pneumoniae infections were similar(40
Implementation of judicial infection control practices would help in improving this dreaded situation. It is of necessary to restrict the use of antibiotics in all clinical practices. To successfully prevent, identify, and treat infections, knowledge of the changing epidemiology of infections is essential, that may lead to a personalised and cost-effective treatment with improving prognosis, and ensuring the judicial use of antibiotics.
Nil
There are no conflicts of interest
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
