
Research Article | DOI: https://doi.org/10.31579/2637-8892/305
1 Transilvania University of Brasov, Brasov, Romania.
2 Faculty of Health, University of Vlora, Vlora, Albania.
3 Transilvania University of Brasov, Brasov.
4 School of Medicine, University of Crete, Crete, Greece.
*Corresponding Author: Sonila Qirko, Transilvania University of Brasov, Brasov, Romania.
Citation: Sonila Qirko, Vasilika Prifti, Emirjona Kicaj, Rudina Cercizaj, Enkeleint A. Mechili, et al, (2024), Patients’ wellbeing and nursing care plans, understanding adherence and relevant factors, a scoping review, Psychology and Mental Health Care, 8(8): DOI:10.31579/2637-8892/305
Copyright: © 2024, Sonila Qirko. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 October 2024 | Accepted: 22 October 2024 | Published: 29 October 2024
Keywords: social emotional well-being; nursing care plan; adherence
Several studies across the world shows the importance of nursing care focusing on patients’ well-being. The adherence of the nursing plan to the well-being of the patients, focuses on two main variables: the nursing plan and the patient's well-being.
This review aims to present a literature review on the impact of nursing care plans on patient adherence and their socio emotional well-being.
The research constitutes a Scoping review that gives evidence from 16 studies published in the period 2015–2023, in English, including patients with chronic diseases and assessing pa-tient’s socio-emotional wellbeing and their adherence to their nursing care plan. We retrieved information on electronic databases of PubMed, Google Scholar, and Cochrane using key-words like nursing care plans, adherence, patient and wellbeing and combination of them. The review is presented following the PRISMA-ScR guidelines. Some studies included in the re-view did not result in high adherence to nursing care plans, affected by various factors such as demographic factors, plans of care, personnel who provided care, face to face and online advice, financial and insurance factors. Most patients show low levels of wellbeing if they were not adherent to nursing care plans, especially the medication adherence issues.
The research findings show that patient’s wellbeing and adherence to nursing care plan are closely related to each other as phenomena. The better the patients feel, the more they are ad-herent to care plans based on evidence. It is important to understand factors that affect non adherence to plans of care in order to reduce negative factors.
A nursing care plan is a formal process that correctly identifies existing needs and recognizes a patient’s potential needs or risk [1]. Nursing care planning, as a way of communication among nurses, their patients, and other healthcare providers, begins when the patient is admitted to the healthcare services and is continuously updated throughout in response to his/her changes in condition and evaluation of goal achievement. Planning and delivering individualized or patient-centered care is the basis for excellence in nursing practice [1].
Adherence is defined as the extent to which a person’s behavior (in terms of taking medications, following specific regimens, or dealing with lifestyle modification) coincides with medical or health advice [2]. Whereas, nonadherence is the patient’s failure to comply with the prescribed treatment regimen for his/her full recovery from such an illness or disease. According to NANDA nursing diagnoses, non-adherence to the nursing care plan is the behavior of a patient or caregiver that does not correspond with the therapeutic plan agreed upon by the individual, family or guardian, and healthcare practitioner [2]. Non adherence is associated to stressful lifestyles and environments, socioeconomic status [3], contrary cultural or religious beliefs and values, lack of social support, and financial resources, and a compromised emotional state [4]. Lack of adherence is linked with unsatisfactory clinical outcomes, increased hospitalizations, lower quality of life, and higher overall healthcare costs [5, 6].
A patient’s wellbeing is closely linked to the adherence to nursing care. The idea of maintaining a state of ‘wellness’ can be linked to a number of different benefits, including improved physical and mental health, faster recovery time from illness, higher educational attainment, greater productivity and an overall healthier lifestyle [6]. Emotional wellbeing is the ability to practice stress management and relaxation techniques, be resilient, boost self-love, and generate the emotions that lead to good feelings [7].
The scope of nursing practice is defined by a broad foundation of scientific knowledge, including the biological and behavioral sciences, combined with the ability to assist patients, families, and other caregivers in managing their own health needs [8]. Nursing Care Plans, which include diagnoses, interventions, and outcomes, continue to mature and reflect the changing times and needs of its readers, as well as the needs of those for whom care is provided [9]. The implementation of nursing interventions is essential in enhancing patient outcomes and guaranteeing the provision of exceptional patient-focused healthcare. Nursing interventions are defined as actions taken by nurses to promote health, prevent illness, and manage the physical, emotional, and social needs of patients [10].
Among the factors that influence clinical utilization of the nursing process are the issues of formulating or stating the nursing diagnosis. Nurses carried out various nursing interventions that were not based on the nursing diagnosis. They were also not evaluating the rendered care, thus the nursing process in totality was not being implemented [11]. The nurses in this context exclusively focused on the problems of the patients that are associated with medical diagnosis or treatment; hence, failing to embrace professional nursing. From the researchers’ clinical experiences, nurses follow the medical orders of doctors to the last; and at times, they are unable to provide any better care to patients who in a specific day were not reviewed by their medical doctors. Hence, the nurses do not take the initiative in patients’ care; as professionals are expected to do [12].
The body of research to support nursing plans and their positive effects on patient wellbeing is ever-increasing and gaining momentum. Nurses continue to study both independent and collaborative interventions for effectiveness and desirable outcomes such as increased positive feelings, lower hospital days, less mortality and morbidity, and fewer costs of health care provided [13,14]. Nurses and other health care staff may greatly contribute to increasing the adherence of patients to care through education, communication, reinforcement, and written advice, thus influencing the wellbeing of the patients and their quality of life [15]. This study aims to present the relation between nursing care plans and patients well-being. We have focused on the specific factors related to treatment regimens, including socio demographic, economic, and health care personnel variables, in order to find strategies that improve patients’ quality of life. A comprehensive review of 16 studies published from 2015 to 2023 provide specific information of nursing approaches that promote and enhance well-being of chronically ill patients among various settings and populations.
2.1 Protocol and registration
The current study is a Scoping review, which we considered appropriate and effective in reaching the goal of our study. According to Munn et.al. in 2022 a scoping review synthesizes evidences to identify and map the evidence on a specific topic or issue, irrespective of source [16].
This review was presented following the Preferred Reporting Items for Scoping Reviews and Meta-Analyses (PRISMA-ScR) guidelines [17].
2.2 Eligibility criteria
According to the review’s aim and objective, we set some inclusion and exclusion criteria. Inclusion criteria were:
Full articles to be presented in English language, exploring wellbeing and nursing care plan adherence especially medication adherence.
Qualitative, and/or qualitative-based, and/or descriptive, and/or quantitative, and/or cross-sectional, and/or observational studies, experimental studies.
Included patients, nurses, healthcare workers and family members.
The review excluded studies not written in English, published before 2015 for the relevance to nursing care plans implementation periods, did not include implementations of nursing care plans and did not include chronic patients.
2.3 Information sources
To find the studies needed for the review, we performed an electronic search between December 1st, 2022 to December 1st, 2023. The search was conducted through databases of PubMed presenting (69 studies), Google Scholar (2 studies), and Cochrane library (79).
2.4 Search strategy
The search strategy consisted of two concepts regarding the aim of the study: (1) Patient’s socio-emotional wellbeing, (2) factors that have an impact on adherence to nursing plan. We used keywords and combinations such as adherence to nursing care plans, wellbeing in health care, quality of life, evidence-based care plans, factors that affect the adherence, chronic patients and their adherence to nursing care plans, health care policies in improving adherence etc.
2.5 Selection of sources of evidence
Research articles part of electronic search were selected in order to evaluate the adherence to the nursing care plan for the well-being of the patients were included in this study.
In three databases we retrieved altogether 150 studies retrieved by relevant key words decided by the researchers. After removing 38 study duplicates and 40 for years of publication out of the eligibility criteria, the researchers identified the relevant articles, and full texts were assessed. The studies in the three databases were manually reviewed by two independent authors (V.P and E.K) following the inclusion and exclusion criteria. In cases of disagreements, the main reviewer assessed the articles (S.N.). For evaluation of the articles, initially they were evaluated and screened by title and after by reading the abstracts and relevance of their aims. All the charting was done by hand by the researchers.
2.6 Data items
After careful study of the selected articles, we presented characteristics of the studies as follow: the year and country of research, the aim of the study, the methodology, results and conclusions.
2.7 Critical appraisal of individual sources of evidences
We did not perform a critical appraisal of individual sources of evidences.
A collection of the information from the studies included is presented according to the country of study, patient population, type of studies, details about the adherence intervention factors such as demographic factors, socio- economic factors etc. Another set of information was about the methods of delivery and type of interventions to improve adherence to care plans according to individual problems of each patient, and a summary of the outcomes of these factors found to affect adherence to care plans. The studies included in this review had different factors mentioned that had their impact on adherence to nursing care plans.
Selection of sources of evidence
We identified a total of 150 studies in three electronic databases. After removing 38 study duplicates and 40 for years of publication we screened 72 articles by abstract and tittle, excluding 30 of them. Of 40 articles for five of them we did not find them in the full form accessible, two were reviews, four did not have nursing care plans clearly presented, 11 were published before 2015 but the articles were relatively old, and two did not include nurses in their education plans. The following PRISMA- ScR flow chart presents the information as follows:
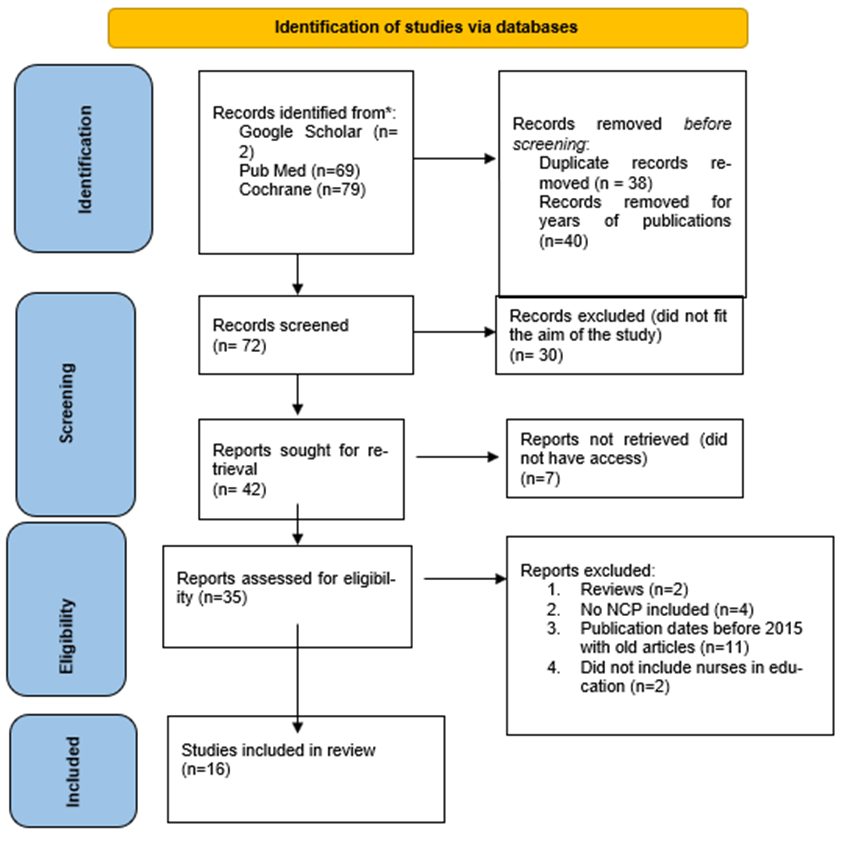
Figure 1: PRISMA-ScR
3.1 Characteristics of sources of evidence
This review included 16 articles published between 2015 and December 2023.Three studies were conducted in 2015, 2017 and 2020 respectively. Three studies were published in 2021, two studies in 2018, four in 2022 and two in 2023. The articles were conducted in various countries such as four in the USA [8,18,19,26]; two in China [21, 22], one in Poland [20],
one in Singapore [23], one in Greece [24]; one in Australia [25]; two in South Africa [27, 28]; one in the Netherlands [29]; one in Colombia [30]; and one in Belgium, Portugal and Italy [31], one in Indonesia [32]. There were four observative studies, five cross sectional studies, three experimental studies, two mix methods studies, one qualitative and one quasi experimental study in this scoping review, all presented in table 1 (annex 1).
Year, Country, Authors | Type of study | Characteristics of patients involved | Adherence level | Factors affecting the adherence | Wellbeing impact on adherence stated |
Sevilla-Cazes, et al 2018 USA | Observational Qualitative patients | 31 Chronic heart patients, males and females in home care and readmitted in hospital | Low adherence | Unclear recommendations Better care in hospitals Financial issues | Patients were in despair mental state. Transformed adherence to adaption. |
Kisielska et al 2022 Szczecin | Observational Prospective cohort | 112 patients after liver transplant | Medium level adherence | High social support, time since surgery, age, gender. | Majority had low or no depressive symptoms |
Souliotis, et al.
2022 Greece | Cross sectional | 250 patients with lung cancer
| Few patients displayed poor adherence; whereas the corresponding percentage among physicians was 12.4%. | Communication gaps between patients and physicians. Long waiting periods to meet the physicians. | None stated |
Gough K, et.al.
2022 Australia |
Experimental | 112 Women on radiotherapy | High level of adherence to the group who got nurse consultations face to face. | Adherence to the tailored specialist nurse consultations was satisfactory, while to telephone consults were less than satisfactory | Complete adherers reported significantly lower levels of psychological distress and significantly higher levels of physical, emotional and functional wellbeing before radiotherapy. |
Yoon S, Kwan YH Singapore 2023
| Qualitative | 25 patients with hypertension | Low levels | therapy-related dimension patient-related dimension healthcare team and system-related dimension cultural beliefs | Cultural factors need to be taken into consideration from health care personnel |
Panahi et.al. 2021
USA | Cross-sectional study | 796 participants | Good levels of adherence | Younger age, lifestyle, long treatment with medications in the clinic and continuity of care | Better general adherence was associated with better chronic disease management |
Ramkisson S, et.al 2017 South Africa | A cross-sectional study | 401 participants with diabetes | Poor adherence | Social support, level of anxiety, social dysfunction, age, public versus private sector | Social support endorsed better levels of well-being. |
McDowelBD, et.al
2020
USA | Cross sectional study | Women (N = 1138) who had completed treatment for Stage 0-III, ductal carcinoma breast cancer | Care coordinated by health care providers increased quality of life | The interaction between health care providers and patients, low health literacy reduced quality of life. | Better quality of life is translated in better wellbeing |
Zhang LL, et.al
2022
China
| Experimental
| 144 patients cranial trauma patients
| Better treatment adherence and compliance in home collaborative care | Type of intervention, collaboration team | Better adherence to collaborative interventions brough higher levels of wellbeing |
Li Y, et.al 2021 China | Experimental | 263 patients with breast cancer | Increased adherence to exercise | Nurse interventions | Better quality of life post intervention |
Spikes T, et.al 2020 USA
| Observational Cross-sectional study | 85 hypertensive African-American women | Low levels of adherence | Dimension of HTN beliefs were associated with medication adherence, illness perception, income | Not clear |
Teunissen DT, et al 2015 Netherlands
| Observational study
| 16 trained NP treated 103 female patients with UI. working in the same practice. | Nurse care practitioner provided care and adherence to treatment increased. | Lack of improvement of the UI and difficulties in performing the exercises | Increased quality of life from interventions of nurse practitioners |
Fords GM, et al 2017 South Africa | A qualitative approach with a descriptive phenomenological design | 10 women with HIV during prenatal period | Women with HIV were adherent to treatment | Loneliness, lack of support, concern of unborn child wellbeing | None stated |
Vargas-Escobar LM, et al. Bogota Columbia 2022 | Cross-sectional, observational-analytical study
| 151 adult patients with cardiovascular diseases 108 family members | High Self care agency increased adherence to treatment | family functioning, type of care received | None stated |
Seys et al
2018 Belgium, Portugal, Italy | Cross sectional
| 257 COPD patients and 284 health care professionals | High adherence in groups with care plans provided
| Education provided by team of health care providers, implementation of a care pathway | Reduced readmission rates brought better quality of life |
Jujuk Proboningsih et al
2023 Indonesia | Quasi experimental | 50 patients with hypertension | High adherence in intervention group | The experimental group received guided modules, and fear ad forgetfulness were factors that had impact on adherence | Chronic care model nursing interventions increase adherence |
Table 1: Characteristics of the studies
3.2 Factors affecting adherence
After a careful review of the articles included, we separated them into 12 categories found to be important. The categories are as below: socio demographic factors, economic factors, communication, well-being, quality of life, health insurance, type of support, health care personnel, consulting, family roles and health care policies. A more detailed description is provided in table 2.
| Factor Category | Specific Factors | Influence on Adherence and Well-Being |
| Socio demographic factors | Gender [8], Race and Gender, Social Support and Depression [19], Marital Status [21], Age [21, 26, 30], Lower Education [21, 24-26, 30] | Patients with Low levels of education present lower adherence levels. Social support, depression, and marital status significantly impact adherence. Age and gender are also influential factors. |
| Economic factors | Financial family Support [27, 30] | Economic support from family improves adherence to nursing care plans. |
| Communication | Communication Between Health Personnel and Patients [24, 25, 27, 29, 32] | Proper communication improves adherence, while communication barriers lower adherence. |
| Well-Being | Emotional Well-Being [18], Depression and Anxiety [20, 23, 25, 28, 29] | Emotional well-being and depression and anxiety treatment are crucial for improving adherence. |
| Quality of life | Nursing Care Affects Quality of Life [20], Implementation of Nursing Care Pathways [22, 31] | Nursing care improves quality of life, and nursing care pathways are associated with higher adherence levels and lower readmission rates. |
| Health insurance | Health Insurance and Health Systems [26, 28] | When patients have good health insurance and health systems are efficient adherence to nursing care plans and treatment is higher. |
| Support | Social and Family Support [27], Working with Families [27] Nurses, nurse practitioners and health care collaborators [25,29] | Good social and family support help to achieve better well-being and higher adherence. Health care personnel plays an important role in adherence to treatment plans. |
| Consulting and interventions | Face to face compared to telephone advise [19,25] Home interventions [22,31, 32] | When patients are advised face to face and at home their adherence is higher, on the contrary over the phone consults show lower adherence to the treatment plans. Guided modules improved adherence levels. |
| Family roles | Family functions [28,30] | Family roles, and hope for the future of children increase adherence, particularly in HIV women and chronic patients with cardio vascular diseases. |
| Health care policies | Intervention policies [18, 24, 27, 28, 30] | Policy interventions enhance communication among patients and nurses, and help families to be included in care plans. |
Table 2: The review studies divided by categories by specific factors
We also studied the positive and negative factors that affect adherence to nursing care plans among chronically ill patients. The information is presented in table 3.
| Factor Category | Studies | Specific Factors | Influence on Adherence and Well-Being |
Socio demographic factors
| [8, 19, 21, 24-26, 30] | Higher education Economic stability Access to health care insurance | Lower education Lack of social support |
| Communication | [24, 25, 27, 29, 32] | Effective communication between healthcare providers and patients Clear communication about treatment plans and instructions Supportive nursing care plans and evidence-based practices | Communication barriers |
| Well-Being | [18, 20, 23, 25, 28, 29] | Positive emotional states Hope for the future | Mental health disorders (e.g., depression, anxiety) |
| Health care provider role | [25,29, 32] | Involvement of healthcare providers (e.g., nurse, nurse practitioner) | Lack of involvement or support from healthcare providers |
Home care interventions Family Functioning | [22,31] [28,30] | Home care interventions based on nursing care plans supported by family members Implementation of nursing care pathways | Family conflict or lack of support |
| Health care policies | [18, 24, 27, 28, 30] | Policy interventions improving communication between patients and healthcare personnel Investments in healthcare systems to improve quality of life Accessible and comprehensive healthcare services | Lack of policy interventions addressing communication barriers Inadequate healthcare system infrastructure Fragmented healthcare system |
Table 3: Specific positive and negative factors that impact adherence to nursing care plans
4.1 Summary of evidence
The 16 studies included in this scoping review examined patients’ adherence to treatments and care plans and the factors that influenced this process. The studies revealed positive and negative factors that greatly affect the adherence to health care plans, including health care work settings, patients’ conditions, loss of family roles, lack of family support, and lack of communication from the team, type of insurance, instruction methods, etc. Results showed that patients are not keen on following nursing care plans, including medication treatment, exercise, diet and nutrition and other aspects of disease treatment.
We found a relationship between gender and adherence to therapeutic recommendations to be unequivocal in one of the studies where women were more adherent than men, [15, 25], but on the contrary when it came to young women with chronic diseases, they were mostly non adherent. Some research authors have demonstrated lower adherence to treatment recommendations after organ transplantation among men emphasizing that type of pathology plays a significant impact on adherence to treatment plan. This may be because men think that they do not need lots of medication, they can be strong and neglect the plan of care [34-36].
The level of adherence to care plans strongly influences the patients’ wellbeing [12, 14, 20, 22], especially the patients with chronic diseases who are less adherent and have higher levels of emotional distress [19].
On the contrary to these findings, a study by Williams et al., concluded that symptoms of depression and bipolar diseases do not have an impact on the adherence to treatment of patients with Hepatitis C, because psychotropic medication helps them adhere to the treatment [33]. Among adults, depressive symptoms have been correlated with poor adherence to anti-epileptic medications, oral medications for cancer and controller medications for persistent asthma [40-42].
One of the findings in the review was that the care plans should focus on the preservation of the family caregiver role, as the patients who are not adherent to care plans have a hard time to perform this role [6]. Similar results came from Marsicano in 2015, stating that the focus of the care plan is on the supportive care rendered by family members, significant others, or caregivers responsible for meeting the physical/emotional needs of the patient. With limited access to health care for many people, most diseases are diagnosed and managed in an outpatient setting, so including the family in alleviating the caregiver-lost role of the patient is important [35].
Similar to this conclusion, the review from Rubin BK, 2018, stated that family members wanted to get involved in the care of their family, wishing to work closely with nurses and doctors, in order to improve treatment adherence by implementing nursing care plans This can meliorate significantly patient experience with the healthcare system and increase their satisfaction of the services received [37].
Lack of education and cultural and socio-economic issues that affect the quality and adherence to nursing management of young women with gestational diabetes, and this need to be addressed in order to optimize care for women. Women are less adherent to diabetes treatment because of their low educational level and not understanding the nursing instructions and continuation of care [18]. These findings are in the same line with the review conclusions of Gast et. al., stating that low levels of education have a negative impact on the level of adherence to treatment of diseases, expensive medications etc. [38].
We noticed in this review that the type of consultations such as the ones face to face [20], advice given by nurses play a better role in helping patients adhere to the plans of care, while when the advice is provided by tele-health other health care professionals [14], offer lower levels of adherence. On the same line with these findings the review from Marques conducted in 2021 concluded that when caregivers and patients work together as a team face to face, many problems that come from improper communication are resolved [39].
One interesting finding in this review was the role of home care model provided by agencies with low and high level of care [6, 25]. Home care without clear instructions and not covered by state insurance agencies reduced the adherence to nursing care plans. This for the fact that no progress on the improvement of the diseases created more frustration and low adherence to the patients. While, the less financial burden creates the plan of care, the odds to follow this plan are higher. On the other hand, the review from Wilder. M, in 2021 found that Structural determinants of health inequities, such as employment, income, and education, were not significantly associated with medication adherence [ 43].
The support offered by health care professionals especially from nurses found in several studies of the review [14, 20, 22]. The patients stated that the higher the support from peer sessions guided by nurses and nursing coordination increased the adherence to treatment care plans. The same results are revealed by Amineh R. in 2020 stating that information on care plans should be done through a model of co-construction between the patient and the health professional. Well supported and educated patients were able to understand their condition and treatment resulting in higher adherence compared to those who lacked support and information [44].
This study has its strength and weakness. This is the first review that presents studies exploring factors that influence adherence to nursing care plans and their effect in wellbeing amongst heterogenous populations with various health problems. The data revealed were rich and settings were different in different countries from undeveloped to developed ones. The study followed the Preferred Reporting Items for Scoping Reviews -ScR guidelines to collect and evaluate the included studies, but we only used some electronic databases. Critical appraisal could not be performed because of the heterogenicity of the data and methods used. Populations included in the study were from different parts of the world and countries with significant changes in their factors affecting the adherence to nursing care plans especially medication adherence.
The review followed PRISMA-ScR guidelines, but this review has its limitations. It is not registered in a protocol on the web. We excluded studies in languages other than English and included only quantitative studies. The studies included explored only the perspectives of patients, but not the nurses’ opinions or data which would provide further detailed information on this topic.
In total, 16 studies were consulted regarding patients’ well-being and their adherence to nursing care plans according to their individual characteristics. A normal complex process that includes emotional, physical, spiritual, social, and intellectual responses and behaviors by which individuals, families, and communities incorporate an actual, anticipated, or perceived loss into their daily live activities. The nurses play an active role in improving adherence to treatment plans thus helping to increase the quality of life and level of wellbeing. Among factors that have a significant role in improving or worsening the adherence to treatment plans are socio demographic factors, role of families in providing support, type of communication, health care policies etc. Improving communication among health care teams and family, providing peer and family support, providing care supported by health care policies will improve adherence rates and increase quality of life in patients with chronic diseases.
none
“Conceptualization, SN. and VP.; methodology, SN.; formal analysis, S.N.; investigation, E.K.; resources, RC.; data curation, VP.; writing—original draft preparation, S.N.; writing—review and editing, S.N. V.P; visualization, V.P.; supervision, L.R.; All authors have read and agreed to the published version of the manuscript.”
“This research received no external funding”
“Not applicable”
Not applicable.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
None
“The authors declare no conflicts of interest.”
,
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
