
Case-Report | DOI: https://doi.org/10.31579/2641-0419/074
Department of Pediatrics School of Medicine Louisiana State University Health Sciences Center 1501 Kings Highway Shreveport, LA 71103
*Corresponding Author: Shabih Manzar, MD, 1501 Kings Highway Shreveport, LA 71103 Telephone: 318-626-1623 Fax: 318-698-4305
Citation: Hilary A. Smith., Manzar S., (2020) Patent Ductus Arteriosus, Hypotension, and Fluid Bolus in a Preterm Infant. J. Clinical Cardiology and Cardiovascular Interventions, 3(7);Doi:10.31579/2641-0419/074
Copyright: © 2020 Shabih Manzar, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 28 July 2020 | Accepted: 07 August 2020 | Published: 14 August 2020
Keywords: hypotension; patent ductus arteriosus; preterm infant; fluids
The incidence of patent ductus arteriosus (PDA) is about 50-55% in term neonates while it varies in preterm infants, depending upon the gestational age and associated respiratory pathology. Hypotension in preterm infants is common. When it occurs with a PDA, it is often difficult to treat. The minute to minute changes in the hemodynamic status is difficult to monitor clinically, therefore the dilemma is restricting versus liberalizing fluids. We present a case in brief, followed by the discussion on how one should approach such a situation.
This male infant was born at 265/7 weeks of gestation to a 29-year-old G2P0010 mother. The pregnancy was complicated by class B diabetes, omphalocele, and a two-vessel cord. Antenatal screen was negative for any chromosomal abnormalities (FISH and microarray negative). Mother received cerclage for short cervix. She presented to the labor unit complaining of leaking fluid. She received antibiotics, steroids, and magnesium sulphate. On examination the following day, the fetal heel was found to be protruding from the cervix. Mother was taken for cesarean section due to fetal malpresentation and omphalocele.
At delivery, the infant was immediately intubated and omphalocele was covered with sterile gauze. He was dried, stimulated, and bulb suctioned. Apgar scores were two and five at one and five minutes, respectively. Upon arrival to the NICU, he was placed on the high frequency oscillator ventilator. On day four of life, he developed a loud murmur and was noted to have low blood pressures. Echocardiogram showed mildly decreased left ventricular (LV) systolic function with ejection fraction (EF) of 50-55%, a small to moderate patent ductus arteriosus (PDA) with left to right shunt (peak gradient across shunt <10 mmHg), and a patent forman ovale (PFO) versus a small secundum atrial septal defect (ASD) with left to right shunt. Hypotension management was started.
It has been estimated that the incidence of patent ductus arteriosus (PDA) in term infant is about 55% in first 24 hours and 57 per 100 000 live births after the second week of life. [1,2] In preterm infants the incidence is dependent upon the gestational age and associated respiratory pathology. It is estimated that about 55% of infants who weigh <1000 g would have a symptomatic PDA. [3] Medical and surgical management of a hemodynamically stable PDA in neonates remains controversial. Failure of ductal closure has been associated with increase in bronchopulmonary dysplasia and increase mortality. [4,5] Furthermore, management of concomitant hypotension is a clinical challenge. The usual trend among clinicians is to give a fluid bolus for hypotension. However, with a PDA, this might be detrimental.
Hypotension is difficult to define in preterm infants. A wide variation in normal ranges has been described. [6] The use of gestational age as a measure of mean blood pressure is discouraged. 7 The indication for fluid rescue in hypotensive preterm infant lies in the complete clinical assessment. [8] What is the respiratory status (e.g. requiring persistent mechanical support)? Are there any signs of heart failure? Is there a large left-to-right ductus shunt with evidence of hemodynamic compromise on echocardiogram? Are there any signs of ductal steal phenomenon whereby descending aortic blood flow is compromised? Is there any oliguria or rising serum creatinine concentration?
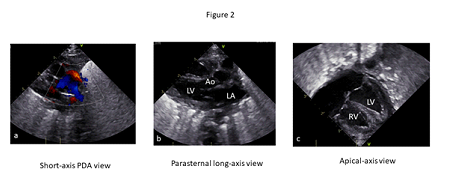
As noted in (figure 1), there were no definite signs of severe pulmonary overload in this infant. The chest x-ray showed right upper lobe atelectasis and pulmonary interstitial emphysema without significant haziness. However, (Figure 2a) demonstrates a significant PDA with left-to-right shunt and (Figure 2b) shows a dilated left atrium suggesting pulmonary overflow. In the same picture (Figure 2c), however, a low left ventricular diastolic volume is noted. In summary, with the mixed echocardiographic findings, one cannot make a concrete decision regarding the need for a fluid bolus.

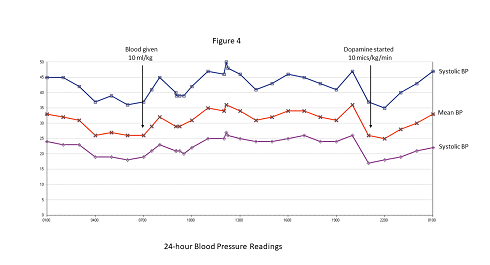
The next step should be to look for systemic signs of hypoperfusion. This infant had edematous extremities with a capillary refill time of less than two seconds. The blood gas showed a pH of 7.28, pCO2 of 53 mmHg, pO2 of 60 mmHg, HCO3 of 22 mmol/Land -0.9 base excess. Serum creatinine was 0.7 mg/dL with normal electrolytes levels. The fluid assessment showed an appropriate input and output (Figure 3). For persistently low blood pressure, the infant received a blood transfusion (hemoglobin of 12 g/dL before transfusion) followed by a dopamine infusion (Figure 4). No extra fluid boluses were given.

In every situation, a fluid bolus should not be given without a complete clinical assessment. Ewer et al [9] have concluded in their study that unless there is clear evidence of hypovolemia, clinicians should exercise caution when prescribing volume expansion. They showed that aggressive fluid bolus administration of or greater than 30 mL/kg is associated with increased mortality in neonates of 27-28 weeks' gestation.
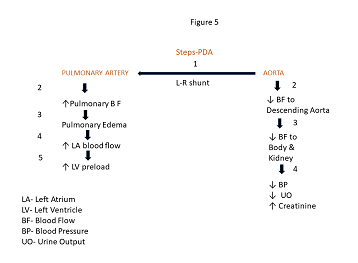
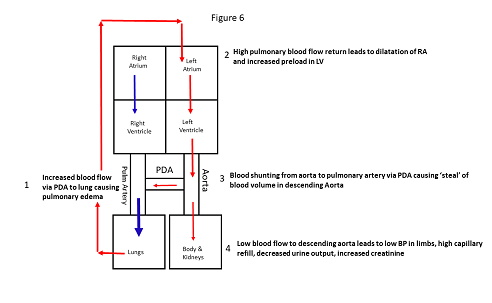
In conclusion, when encountered with hypotension in a preterm infant with concomitant PDA, one must look at many factors to decide on the fluid chase. (Figure 5 and 6) summarize these steps. A comprehensive assessment of the respiratory status, perfusion, and urine output should be coupled with an echocardiogram, blood gases, serum creatinine, and electrolytes.
None
None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
