
Case Report | DOI: https://doi.org/10.31579/2641-0419/341
Department of Cardiology, National centre of cardiology (CNC) Nouakchott Mauritania.
*Corresponding Author: El Abasse Zeine, Department of Cardiology, National centre of cardiology (CNC) Nouakchott Mauritania.
Citation: El Abasse Zeine, El Haj Ahmed NE, Sid M’Hamed Ethmane, Ahmed Ebba (2023), Particularity of Coronary Artery Aneurysm Management. J. Clinical Cardiology and Cardiovascular Interventions, 6(7); DOI:10.31579/2641-0419/341
Copyright: © 2023, El Abasse Zeine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 26 October 2023 | Accepted: 07 November 2023 | Published: 13 November 2023
Keywords: Coronary artery ectasia; coronary artery aneurysm; pathophysiology; diagnosis and management
Aneurysmal dilation of coronary arteries is observed in up to 5% of patients undergoing coronary angiography. Due to their poorly elucidated underlying mechanisms, their variable presentations, and the lack of largescale outcome data on their various treatment modalities, coronary artery aneurysms and coronary ectasia pose a challenge to the managing clinician. This paper aims to provide a succinct review of aneurysmal coronary disease, with a special emphasis on the challenges associated with its interventional treatment.[1]
Coronary artery ectasia likely represents an exaggerated form of expansive vascular remodeling in response to atheroslerotic plaque growth with atherosclerosis being the most common cause. Although, it has been described more than five decades ago, its management is still debated.
We diagnosed 13 patients admitted for acute coronary syndrome, in whom coronary angiography revealed thrombotic occlusion of aneurysmal arteries.[2] double platelet antiaggregation and anticogulation therapy were associated.
we found that anticoagulation treatment combined with platelet anti-aggregation treatment accelerated the disappearance of the thrombus, enabling visualization of the artery so that a decision could be made whether or not to undergo angioplasty. the aim of this article is to investigate in literature how acute coronary syndrome can be managed in aneurysmal arteries.
Aneurysmal dilation of coronary arteries is found in up to 5% of patients undergoing coronary angiography [1]. The presence of coronary aneurysm or ectasia has been associated with poor long-term outcomes irrespective of the presence of concomitant atherosclerotic coronary artery disease [3–4]. Clinical presentations range from incidental finding on cardiac imaging to acute coronary syndrome [5]. Treatment options include medical management, surgical excision, coronary bypass grafting (CABG), and percutaneous coronary interventions (PCI). However, due to the lack of randomized trials or societal recommendations, the management of these patients poses a clinical dilemma to the clinician. The aim of this paper is to provide a concise overview of the pathophysiology, classification, clinical presentation, assessment, and management strategies of aneurysmal coronary disease.
Bougon first described abnormal dilation of coronary arteries in 1812 [6]. In 1953, Trinidad et al. [7] published the 49th case of “aneurysm of the coronary artery” in the published reports. Since then, many publications have brought forth a deeper understanding of this entity. Interestingly, until recently, 2 terms have been used interchangeably to indicate the presence of aneurysmal dilation of coronary vessels: coronary artery aneurysm (CAA) and coronary artery ectasia (CAE) [8]. This has often led to incertitude, as these synonymously used terms actually refer to 2 different phenotypes. Therefore, arbitrary criteria have been suggested to differentiate between these 2. By these criteria, a focal dilation of coronary segments of at least 1.5 times the adjacent normal segment is described as CAA, whereas the term CAE is used to define similar, but more diffuse, lesions [9,10]. CAAs are then divided to saccular aneurysms if the transverse diameter exceeds the longitudinal diameter, and to fusiform aneurysms in the opposite case. Subclassification of CAA and CAE based on morphological or intravascular imaging factors has also been suggested.
We diagnosed 13 patients admitted for acute coronary syndrome, in whom coronary angiography revealed thrombotic occlusion of aneurysmal arteries.double platelet antiaggregation and anticogulation therapy were associated.
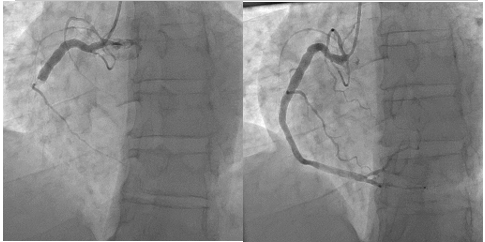
We found that anticoagulation treatment combined with platelet anti-aggregation treatment accelerated the disappearance of the thrombus, enabling visualization of the artery so that a decision could be made whether or not to undergo angioplasty. the aim of this article is to investigate in literature how acute coronary syndrome can be managed in aneurysmal arteries.

Before and after anticoagulant treatment combined with double antiaggregation

Before and after anticoagulant treatment combined with double antiaggregation
Before and after anticoagulant treatment combined with double antiaggregation

Before and after anticoagulant treatment combined with double antiaggregation
The pathogenesis of CAA is not well understood. However, there is compelling evidence of particular associations between certain risk factors and CAAs:
1. An individual genetic susceptibility to the formation of CAA, especially in patients with congenital CAA has been suggested [11].
2. The strong association between CAA and coronary artery disease implies a possible common underlying etiology [12,13].
3. There is a high prevalence of noncoronary aneurysmal disease in patients with CAA and vice versa, suggesting another mechanism distinct from atherosclerosis that causes generalized arterial dilation [14,15].
4. Certain vasculitic and connective tissue diseases have a proven interrelation with CAA (e.g., Kawasaki disease, Marfan, and so on) [16].
5. Local wall injury following intracoronary manipulation (angioplasty, stenting, brachytherapy, and so on) has been shown to provoke the formation of CAA. However, notable differences seem to exist between these interventions, with CAAs being more frequently reported following brachytherapy due to the late effect of adaptive remodeling, and drugeluting stent implantation due to the impaired intimal healing effects of the antiproliferative agents [17,18–19]. Notably, there have been fewer published reports of CAA formation following second- and third-generation stent implantation [20,21]. Whether this represents a reporting bias versus a true improvement with newer stents remains unknown. There has been, nevertheless, a concerning number of reports of CAA following PCI with biodegradable stents [22–23].
6. Post-infectious CAAs have been reported and are believed to be the result of direct wall invasion or immune complex deposition [24].
An uncommon, but an important, subset of aneurysms to allude to is the category of aortocoronary saphenous vein graft aneurysms (SVGAs). These aneurysms have distinctive characteristics compared with native coronary aneurysms:
1) they often present very late following bypass grafting. In a systematic review of 168 cases, 68.5% presented >10 years after CABG;
2) they are significantly larger than CAAs; 3) they usually progress over time; and 4) not uncommonly, they present with mechanical complications (e.g., compression of adjacent cardiac or venous structures, or rupture) [25].
Most CAAs are clinically silent and are only detected incidentally during coronary angiography or computed tomography. However, clinical symptoms can develop due to one of the following reasons:
1) the presence of concomitant obstructive atherosclerotic disease can result in both effort angina or acute coronary syndrome;
2) local thrombosis in the lumen of large aneurysms may lead to distal embolization and myocardial infarction (MI) [26,27].
3) massive enlargement of some CAAs and SVGAs can result in compression of adjacent structures [25,28]
4) aneurysm rupture, albeit rare, can cause acute cardiac tamponade [25,27]
5) stressinduced myocardial ischemia due to microvascular dysfunction has been documented even in the absence of significant coronary stenosis [29].
Coronary angiography has been diagnostic modality of choice until newer modalities like coronary Magnetic resonance angiogram (MRA) and coronary computed tomography angiogram (CTA) has become available. Angiography shows disturbances in blood flow filling and washout, which are associated with the severity of ectasia. Angiographic signs of turbulent and stagnant flow include delayed antegrade dye filling, a segmental back flow phenomenon, and local deposition of dye in the dilated coronary segment. Coronary MRA has been shown to be equal to quantitative coronary angiography with the additional advantage of being a noninvasive technique [30, 31]. Coronary MRA may offer further valuable information, when complemented with coronary flow data, about the possibility of thrombotic occlusion of the aneurysmal vessels. Additionally MRA, being a noninvasive, non-radiating technique, can be used efficiently for follow up of these patients. Coronary CTA is another noninvasive modality used to diagnose CAE [32]. Coronary CTA can be suggested as a technique of choice for the follow up of patients because of improvements in terms of radiation dose with the current protocols. Intra vascular ultra sound (IVUS) is an excellent tool for assessing luminal size and characterizing arterial wall changes. IVUS correctly differentiates true from false aneurysms caused by plaque rupture. Emptied plaque cavities may appear angiographically as CAE and the distinction is of clinical importance, as false aneurysms may lead to acute coronary syndromes [33].
Management
Management is similar to that of CAD with few exceptions. It includes medical, angioplasty with stent and surgical modalities.
Medical Management
It is a controversial area as there is lack of evidence based medicine. Aspirin was suggested in all patients , because of coexistence of CAE with obstructive coronary lesions in the great majority of patients and the observed incidence of myocardial infarction, even in patients with isolated coronary ectasia [34]. The role of combined antiplatelet therapy, with the addition of adenosine diphosphate inhibitors, has not yet been evaluated in prospective randomized studies. It has been shown that plasma levels of P-selectin, beta thromboglobulin and platelet factor 4 are elevated in isolated CAE patients when compared with control participants who have angiographically normal coronary arteries, suggesting an increased platelet activation [35]. Based on the significant flow disturbances within the ectatic segments, chronic anticoagulation with warfarin as main therapy was suggested [36]. However, this treatment has not been tested prospectively, and could not be recommended unless supported by further studies and until then should be based on risk versus benefit [39].
Medications such as ACE inhibitors, statins may be useful in affecting the disease progression. Based on the association of ACE gene polymorphism and CAE, ACE inhibitors could be useful in the suppression of CAE progression, but this is yet to be proven [37]. Because elevated MMP-3 levels likely contribute to the development of coronary aneurysms, this matrix-degrading enzyme may represent an important therapeutic target. Statins could be beneficial by inhibiting MMP-3 activity, corticosteroids, IL-4 and by suppressing MMP expression [38, 39]. Administration of nitroglycerin and nitrate derivatives may induce angina pectoris in patients with CAE and should be avoided [40].
Percutaneous Intervention (Pci)
In patients with coexisting obstructive lesions and symptoms or signs of significant ischemia despite medical therapy, PTCA can be done. Polytertafluoroethylene (PTFE)- covered, balloon-expandable stent has been shown to be an effective device for the percutaneous management and for exclusion of coronary aneurysms [41].
Surgery
In the symptomatic patient not suitable for PCI, surgical excision or ligation of the CAE combined with bypass grafting of the affected coronary arteries can be the procedure of choice [43]. Good outcomes has been demonstrated after these procedures [42].
Prognosis
Long-term prognosis and outcome in patients with CAE is unknown. In the CASS registry no difference in survival was observed between patients with or without CAE [1]. Several studies thereafter failed to show a mortality difference between CAE and CAD and concluded that CAE is a variant of atherosclerosis that confers no additional risk [43, 44, 45].
Coronary artery ectasia incidence ranges from 1.2%-4.9%. It is a complex pathophysiological process involving the interaction of various pathways, in turn leading to excessive positive remodeling resulting in ectatic vessels. The prognosis is determined mainly by the severity of the coexisting obstructive CAD. Currently, there are no guidelines for treatment of CAE. Management is similar to that of CAD with few exceptions. Overall, management is hampered by lack of evidence. We need prospective studies and registries to further our knowledge in the management of this disorder.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
