
Research Article | DOI: https://doi.org/10.31579/2642-973X/008
*Corresponding Author: Osamu Yamamura, Department of Neurological Sciences .China
Citation: Pu Liu, Qu Jian. (2019). Parkinson's disease: Role of Acupuncture Study a Randomized Study of Fatigue Behavior. Brain and Neurological Disorders. 2(1); DOI: 10.31579/2642-973X/008
Copyright: © 2019 Pu Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 31 December 2018 | Accepted: 17 January 2019 | Published: 23 January 2019
Keywords: acupuncture, fatigue, Parkinson's disease, randomized controlled trial
Fatigue is a common and disabling problem in patients with Parkinson's disease (PD), and there is currently no satisfactory treatment. As acupuncture has been reported to be effective in fatigue related to other conditions, we sought to evaluate its efficacy in PD.
Fatigue is one of the commonest nonmotor symptoms in Parkinson's disease (PD) and has negative impact on quality of life (Barone et al., 2009; Friedman, Abrantes, & Sweet, 2011; Skorvanek et al., 2013). In one of the first studies on fatigue in PD, 15–33% of patients rated it as their most disabling symptom, and more than half rated fatigue among their three worst symptoms (Havlikova et al., 2008). There is currently no satisfactory treatment of PD‐related fatigue (Franssen, Winward, Collett, Wade, & Dawes, 2014).
Acupuncture has been shown to be effective in the treatment of fatigue related to other conditions, in particular, cancer‐related fatigue (Molassiotis et al., 2012; Sood, Barton, Bauer, & Loprinzi, 2007). Apart from a recent study (Kluger et al., 2016) its role in PD‐related fatigue has not been explored. The aim of this randomized, controlled pilot study was to evaluate the efficacy of a 5‐week course of acupuncture in the treatment of fatigue in PD.
This was a randomized, patient and assessor‐blinded, controlled pilot study assessing the efficacy of acupuncture in patients with PD‐related fatigue.
Subjects and setting
Participants attending the Parkinson's disease Clinic of National Neuroscience Institute‐Tan Tock Seng Hospital, Singapore who met the following inclusion and exclusion criteria were recruited. The inclusion criteria were [1] diagnosis of PD based on criteria developed by Gelb, Oliver, & Gilman (1999) which is adopted by the National Institute of Neurological Disorders and Stroke, US National Institute of Health, [2] age 21–85 years old, [3] presence of moderately severe fatigue as defined by a score of ≥10 on the General Fatigue domain of the Multidimensional Fatigue Inventory (Smets, Grasen, Bonke, & De Haes, 1995), and [4] no acupuncture treatment in the past 6 months.
The exclusion criteria were [1] significant cognitive, language or psychiatric illnesses which prevents the subject from understanding instructions and participating in the study, [2] needle phobia, [3] comorbidity with a bleeding disorder, [4] known anemia with hemoglobin level <10>
Screening and Randomization
Opportunistic screening of patients attending the Parkinson's Disease Clinic of National Neuroscience Institute‐Tan Tock Seng Hospital, Singapore was conducted. After informed consent, eligible patients were randomized in a 1:1 fashion without stratification to real or sham acupuncture using permuted blocks. Allocation to treatment group was managed by an interactive web response system using computer‐generated lists organized by a statistician who is independent of the study. Only the two treating acupuncturists had access to the interactive web response system. All other study team members were blind to group assignment.
Treatment consisted of twice‐weekly sessions at least 3 days apart for 5 weeks, giving a total of 10 sessions of acupuncture. Acupuncture was performed with the patient supine on a acupuncture table. The retractable noninvasive sham and invasive acupuncture needles developed by Jongbae Park (Park Sham Device, PSD) were used in this study (Park, White, Stevinson, Ernest, & James, 2002). Both real and sham needles have a fine needle body and copy handle and look exactly the same. However, the retractable needle has a retractable shaft and blunt tip. When pressed onto the skin, it telescopes into the handle and the blunt tip stays on the skin instead of penetrating it. The plastic tube with adhesive foot‐plate is placed on the skin to hold it in place. The real needle, on the other hand, has a normal sharp tip which allows it to pierce the skin. Both needles are 70 mm long. The Park Sham needle has been well validated as an inactive and credible placebo control in clinical acupuncture trials.
Primary outcome measure
The primary outcome measure was the change in General Fatigue domain score of the Multidimensional Fatigue Inventory (MFI) from baseline at 5 weeks. The MFI is a 20‐item self‐reporting tool that measures five dimensions of fatigue: General Fatigue, Physical Fatigue, Reduced Activity, Reduced Motivation, and Mental Fatigue. Each subscale contains four items, which are scored on a five‐point Likert scale.
In a previous study of prevalence of fatigue in PD using the MFI, the mean General Fatigue score was 15.2 with a standard deviation of 3.0 (Skorvanek et al., 2013). Assuming a 20% reduction in MFI score in the acupuncture group compared to control, a two‐sided sample comparison of means requires 16 participants per group with significance level at 0.05 and power of 0.8. Hence, a total of 32 participants need to be recruited. Assuming a drop‐out rate of 20%, the number of participants needed will be 40. The effect size of 20% was chosen on the premise that anything less than this is not likely to be clinically significant.
Group demographics and characteristics
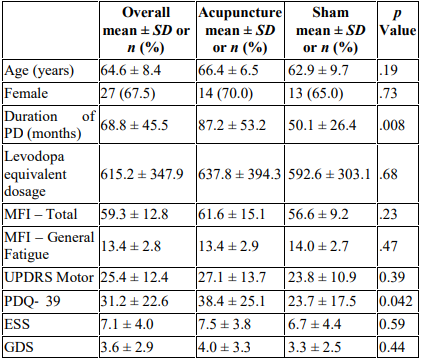
p‐ values that are in bold shows statistical significance.
Assessment of blinding
Patients were queried at Week 5 point regarding what group they thought they were in, and there were no between‐group differences in patients’ perceptions of group assignment consistent with effective blinding (chi‐square, p = .32).
The results of this pilot study show that a 5‐week course of acupuncture treatment, real or sham, was effective in improving fatigue in a cohort of patients with PD. Furthermore, this improvement was maintained up to 4 weeks after completion of treatment. Apart from improved UPDRS Motor scores, real acupuncture group had no significant impact on scores of quality of life, mood, and excessive daytime sleepiness compared with sham acupuncture. In fact, there was a trend toward greater reduction in fatigue scores in the sham group (p = .09). To evaluate whether the improvement in fatigue is clinically meaningful, we looked at the minimal important difference of the MFI. The minimal important difference is defined as “the smallest difference in score in the domain of interest which patients perceive as beneficial and which would mandate, in the absence of troublesome side effects and excessive cost, a change in the patient's management” and is particularly useful in patient‐reported outcome measures (Jaeschke, Singer, & Guyatt, 1989). Unfortunately, no data exist on the minimal important difference of the MFI in PD. Hence, we can only extrapolate from data involving patients with rheumatological conditions, and in this group of patients, the minimal important difference for the MFI‐Total is 11.5 (Nordin, Taft, Lundgren‐Nilsson, & Dencker, 2016). Using this result, 40% of real acupuncture and 60% of sham acupuncture patients in our study had clinically meaningful improvements in fatigue.
Acupuncture (real and sham) is safe and effective in reducing fatigue in a cohort of patients with PD. Given the current absence of satisfactory treatment of fatigue, there is a potential role for the use of acupuncture in the treatment of PD‐related fatigue, even if its mechanism of action is largely placebo.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
