
case report | DOI: https://doi.org/10.31579/2690-1897/210
Department of Surgical Gastroenterology, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Puducherry, India.
*Corresponding Author: Biju Pottakkat, Professor of Surgical Gastroenterology, 4th floor, Superspeciality block, JIPMER, Puducherry.
Citation: Satyaprakash R. Choudhury, Biju Pottakkat, Sankar Narayanan, Kalayarasan Raja, Sakthivel H, et al, (2024), Parenchymal Preserving Approach with Hepatotomy and Lesionectomy Using Surfacing Technique for Deep-Seated Liver Lesions, J, Surgical Case Reports and Images, 7(7); DOI:10.31579/2690-1897/210
Copyright: © 2024, Biju Pottakkat. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 05 August 2024 | Accepted: 22 August 2024 | Published: 28 August 2024
Keywords: parenchyma preserving; hepatotomy; lesionectomy; metastatectomy; deep-seated liver lesions
Though anatomical resections are considered the standard of care for primary and secondary liver tumors, non-anatomical resections are preferred in specific scenarios mainly for preserving the normal liver parenchyma [1]. The fundamental principle behind this non-anatomical resection is the preservation of functional liver volume without any compromise on tmor margins. Comparable overall and recurrence-free survivals are being reported in favor of non-anatomical resections, more so in low-grade neuroendocrine tumors and colorectal liver metastases [2,3]. The basic understanding of a non-anatomical resection is to excise the lesion along with a rim of surrounding liver parenchyma, ensuring a negative margin all around. This is usually in the form of a wedge resection resulting in a three-dimensional defect. In lesions located away from the surface, the purpose of this wedge excision is purely for technical feasibility. This may result in a significant parenchymal loss despite the small size of the lesion. Furthermore, when resections are being considered the gold standard for any primary or metastatic liver lesions, because of the location and fear of loss of parenchyma due to wedging, non-operative therapies especially radiofrequency ablation are employed [4]. The available state-of-the-art equipment has ensured stringent monitoring in the peri-operative period, promoting complex liver resection with oncological precision. Here, we describe a new approach in surgical resection for deep-seated liver lesions by a hepatotomy followed by lesionectomy. In this technique, intraoperative ultrasonography (IOUS) is an imperative component guiding the resection plane. Following lesionectomy, the hepatotomy was approximated using intermittent sutures.
A 65-year-old gentleman initially diagnosed as metastatic neuroendocrine tumor involving the head of the pancreas underwent staged resection. The first resection was pancreaticoduodenectomy followed by right hepatectomy for multiple metastatic lesions involving segments 5,6, and 7. On a routine follow-up at two years, ultrasonography revealed a lesion in segment 3. Additionally, a contrast-enhanced computed tomography (CECT) and 99mTc-Hynic-TOC scan were performed. The lesion was enhanced in the arterial phase with a positive uptake of the 99mTc-HynicTOC scan, confirming the diagnosis of a metastatic neuroendocrine lesion. Subsequently, after the 3-D reconstruction using the Myrian XP platform (for precise mapping of the lesion and assessing remnant liver volume), the patient was planned for a parenchyma preserving lesionectomy. After adequate mobilization of the liver, the lesion was located with the help of intraoperative ultrasonography (IOUS). The depth of lesion from the surface and the relationship with surrounding vasculature were noted as shown in Figure 1.
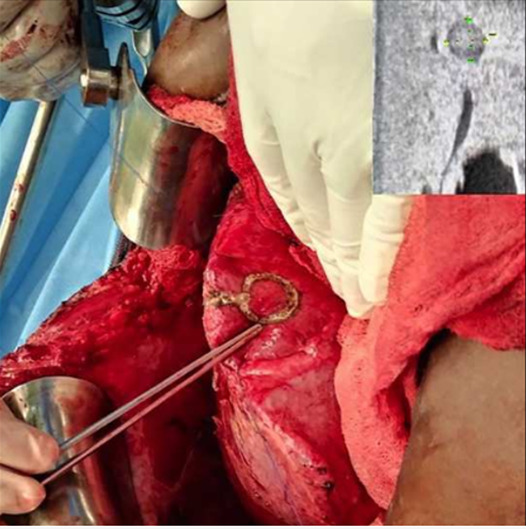
Figure 1: Initial marking of the extent of the tumor using Intra-operative ultrasonography.
The plane of hepatotomy on the superior surface of segment 3 and the area of the liver corresponding to the lesion on the inferior surface of segment 3 was marked with the help of IOUS. The hepatotomy was started from the nearest surface, and IOUS was used frequently to avoid major vessels on the hepatotomy plane. The liver parenchymal transection was performed using the Cavitron Ultrasonic Surgical Aspirator (CUSA) and bipolar electrocautery as shown in Figure 2.
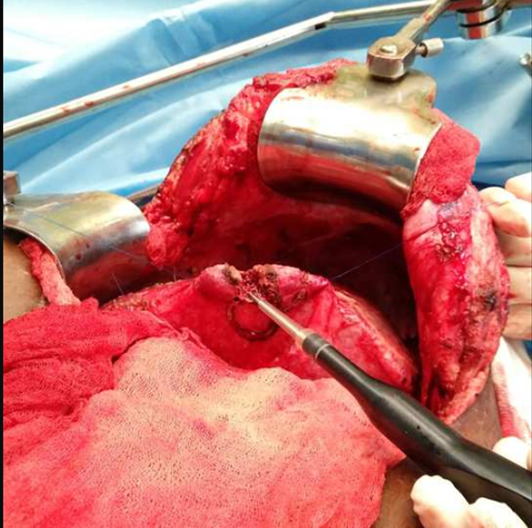
Figure 2: Initial hepatotomy using CUSA (Cavitron Ultrasonic Surgical Aspirator).
After the initial hepatotomy until the lesion's superior border, a curvilinear path opted to surf onto one side of the lesion. This opened up a new surface wherein the lesion became superficial which is shown in Figure 3.
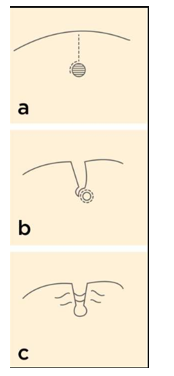
Figure 3: Depiction of the surfacing technique. A. Initial hepatotomy after reaching the superior border of the lesion takes a curvilinear path.
Authors wish to name this technique 'surfacing'. The feeding vessels were ligated and divided. After reaching the distal-most margin, the lesion could be resected easily in a hemispherical plane as a wedge as shown in Figure 4
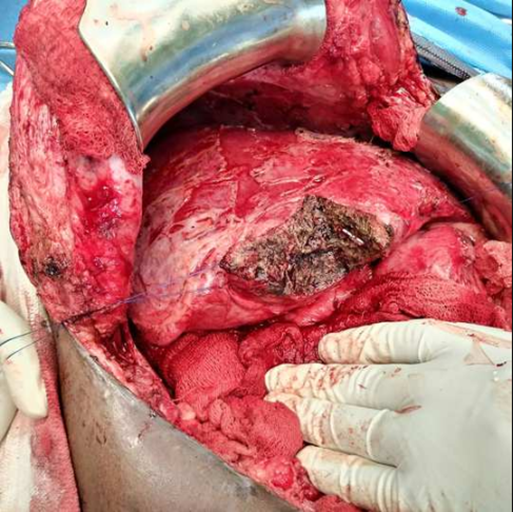
Figure 4: Completed lesionectomy following ligation of vascular pedicle
The hepatotomy plane was approximated with interrupted sutures to prevent any possible bile leak and bleed from the raw area as shown in Figure 5. The biopsy showed a well differentiated neuroendocrine tumor with negative margins. Patient had an uneventful recovery and was discharged by post-operative day 7.
Parenchyma preserving liver resection is an alternative strategy aimed to increase the FLR. They may vary from non-anatomical resections (enucleations, sub-segmentectomies, and wedge) to anatomical resections like monosegmentectomy, bisegmentectomy, central hepatectomy). Multiple studies have confirmed their safety and efficacy with comparable overall and recurrence-free survival rates. These conservative approaches preserve the functional liver volume, where otherwise extended resections may not be possible or in bilobar disease or patients requiring redo resections. Our patient had already undergone a right hepatectomy in the past, and hence the most feasible option was to excise it locally with a negative margin. The initially described technique of cherry-picking became a popular form of non-anatomical lesionectomy [3]. Their description involves IOUS localization of the lesion followed by division of the glissonian capsule. Following this, a sonography guided digital dissection was employed to enucleate the tumor. The authors also prefer employing the cherry-picking technique using electric scissors, electrocautery, or CUSA for multiple lesions located closely within the same area of the liver. Following excision, and hemostasis was achieved by energy sources or by suture ligation. The raw area was left open, while the possibility of bilioma or hematoma might mandate re-exploration. Deep-seated lesions pose a challenge as most of them may require a segmentectomy or a lobectomy. In such scenarios, local ablative therapies are employed in managing deep-seated lesions [4]. In lesions within the parenchyma but close to the surface, wedge resections are preferred. However, this again results in loss of normal parenchymal volume disproportionate to the tumor volume. IOUS helps in this situation to localize the tumor and guide resection with a negative margin. Torzilli et al. have pioneered IOUS in liver resections for tumors in difficult locations [5]. Our technique is similar to the one used in deep-seated brain tumors and brain abscesses. The brain parenchyma above the lesion is divided to approach rather than excised. Subsequently, the lesion is enucleated with a small margin [6]. The findings of intra operative ultrasound are critical in deciding the type of resection. The techniques like the mesohepatecomy, mini-mesohepatectomy, and liver tunnel are recommended only after confirming the presence of intercommunicating veins or inferior right hepatic vein [7,8]. Another critical point of concern is the margin status and is now agreed on 1 mm as the minimum desired negative margin. Viganò L et al. published a report on the tumor detachment from the vascular structures during metastasectomy for colorectal liver metastasis. The authors have classified the margin as parenchymal and vascular. When hepatic or portal pedicles are in contact with the tumor, it is resected off while taking care to preserve the vascular structure. Although they found R1 parenchymal positivity has high recurrence rates, interestingly, the R1 vascular margin has outcomes equivalent to that of R0 rates [9]. Our technique differs from the cherry-picking technique by starting with a hepatotomy, surfacing on one side of the lesion, lesionectomy, while preserving and controlling the major pedicles supplying the lesion. With instruments like CUSA, intra-parenchymal operations can be performed with greater precision.
Our technique is useful in patients for whom major hepatectomies have already been done, and when there not enough remnant volume. It can also be used to resect multiple lesions in bilobar disease, thereby not only preserving the liver parenchyma but also ensuring a negative margin with a serial ultrasonogram assessment. With the reconstruction platforms like Myrian XP exact future liver remnant can be assessed and multiple hepatotomies can be performed along the anatomical and nonanatomical planes sparing portal pedicles and hepatic veins. The essential step of creating an additional surface near the lesion makes it surfaced. However, the present technique is difficult to apply for lesions located in segment 4A or posteriorly near the hepatic venous confluence with the inferior vena cava.
Statement of Ethics
Please address the following aspects in your Statement of Ethics.
Study approval statement: This study was reviewed and approved by JIPMER ethics committee with number - JEC/89019.
Consent to publish statement: Informed consent was obtained from the patient.
Conflict of Interest Statement
The authors have no conflicts of interest to declare.
This study was not supported by any sponsor or funder.
Author Contributions
Concept; Manuscript editing; clinical advisor - Prof. Biju Pottakkat.
Raw data collection, Initial manuscript writing - DR Satyaprakash Ray Choudhury.
Idea and editing of supplementary files (Figures and tables), Initial manuscript drafting- DR Sankar Narayanan.
Manuscript editing; clinical advisor - DR Kalayarasan Raja.
Subsequent editing and submission process - DR Sakthivel H.
Subsequent editing and submission process - DR Sai Krishna
Data Availability Statement
The data of the article is available in the department database and can be provided on request.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
