
Case Report | DOI: https://doi.org/10.31579/2768-2757/058
1 Oman Medical Specialty Board, Oman
2 Sultan Qaboos University Hospital, Oman
3 Sultan Qaboos University Hospital, Oman
*Corresponding Author: Sawab Al Hosni, Oman Medical Specialty Board, Oman
Citation: Sawab Al Hosni., Yahya Al Badaai, Shebl A, (2022). Parathyroid Carcinoma in A Young Patient with End-Stage Renal Disease: A Case Report from Oman. Journal of Clinical Surgery and Research. 3(5); DOI: 10.31579/2768-2757/058
Copyright: ©2021 Sawab Al Hosni, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 September 2022 | Accepted: 26 September 2022 | Published: 16 November 2022
Keywords: parathyroid carcinoma; thyroid carcinoma; endocrine surgery; parathyroid adenoma; parathyroid surgery
Parathyroid carcinoma is an extremely rare malignancy, accounting for less <0.005% of all cancers and <1% of parathyroid disorders. Pre-operatively, it can be suspected from the tumor size, which usually exceeds 4cm, as well as a high parathyroid hormone (PTH). However, histopathological features confirm the diagnosis. The main objective of treatment is en block resection of the tumor, with excision of the ipsilateral thyroid. We describe a young female with end-stage renal disease (ESRD) who got diagnosed with parathyroid carcinoma. Ultrasound (US) and Sestamibi scans were both suggestive of parathyroid adenoma. Post-operatively, histopathological diagnosis of the specimen revealed parathyroid carcinoma. We introduce this case that was initially suspected to be parathyroid adenoma until histopathological diagnosis revealed parathyroid carcinoma. Patients with ESRD and hypercalcemia with sky-high PTH may have the suspicion for parathyroid carcinoma masked as those lab results can commonly get attributed to the ESRD.
The first case of parathyroid carcinoma to appear in the literature was in 1909 by De Quervain, in which the diagnosis was attributed to the macroscopic characteristics of the lesion [19]. Today, it is known that parathyroid carcinoma is an extremely rare malignancy, accounting for less than 0.005 Percent of all cancers and less than 1 Percent of parathyroid disorders [13] , [8]. It is most commonly found to be sporadic, but cases have also been reported associating parathyroid carcinoma with familial primary hyperparathyroidism as hyperparathyroidism-jaw syndrome and in multiple endocrine neoplasia type one [3]. Parathyroid carcinoma can be suspected preoperatively from the size of the tumor, which usually exceeds 4 cm, as well as a high level of PTH. However histopathological features confirm the diagnosis [9]. The main objective of treatment is en block resection of the tumor with negative margins. Excising the ipsilateral thyroid lobe may be necessary to perform this, however, it has not been proven to improve survival in patients with parathyroid carcinoma [23]. The aim of this report is to present the management of case that is rarely diagnosed and which might help guide future studies on the same topic.
A 27-year-old lady was referred from her Nephrologist to the Head and Neck clinic for parathyroidectomy in view of hypercalcemia and sky-high PTH level of around 366 pmol/L. The only clinical complaint she had was diffuse bone pain. Her background medical history also includes ESRD secondary to adult polycystic kidney disease (ADPKD) in which she has been on hemodialysis (HD) for 7 years prior to presentation. Her physical examination revealed a 2cm lesion in the left thyroid region with no cervical lymphadenopathy. Laboratories’ investigations reveled a sky-high PTH level of 366 pmol/L (normal range 1.6-6.9 pmol/L), a high albumin-adjusted calcium level of 2.64 mmol/L (normal range 2.15-2.55 mmol/L), high alkaline phosphatase of 497 U/L (normal range 35-104 U/L), normal vitamin D of 116 mmol/L (normal range 50-125 nmol/L) and high phosphate of 2.07 mmol/l (normal range 0.81-1.45 mmol/L). US of the neck showed a well-defined fairly rounded lesion in relation to the lower pole of the left thyroid gland measuring 2cm in diameter and with obvious increased vascularity (Figure 1a). In addition, a well-defined ovoid-shaped hypoechoic nodule, with mild increased vascularity, was seen in the right thyroid lobe measuring about 0.8 x 0.46 cm. There were no suspicious lymph nodes (Figure 1b).
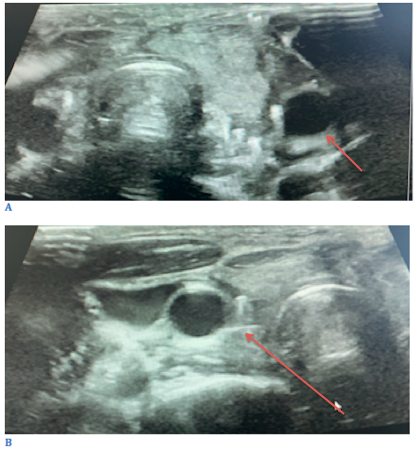
Figure 1
A technetium 99m Sestamibi scan was done which showed homogenous uptake by the thyroid glans, with an intense focal uptake in the left lower lobe. The findings were suggestive of a parathyroid adenoma (Figure 2).
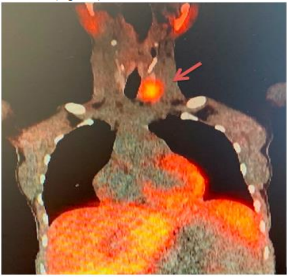
Figure 2
In view of the US findings, fine-needle aspiration cytology (FNAC) was performed for the thyroid nodule. Diagnosis was a benign follicular nodule. Bone densitometry scan was also done and revealed the patient’s bone mineral density to be below the expected range for her and gender. Intra-operative findings revealed a large left superior parathyroid lesion and prominent remaining parathyroid glands.
She underwent a total parathyroidectomy and a right hemithyroidectomy for the right thyroid hypoechoic nodule. Intraoperative frozen section confirmed the parathyroid tissue from all four glands. Histopathological diagnosis of the specimens reveled the left superior parathyroid carcinoma (3 x 1.6 x 1.3 cm). Sections prepared revealed encapsulated tumor tissue with a thick capsule. The tumor is composed of chief cells with some oncocytic and transitional cells. The cells are arranged predominantly in a diffuse pattern. A rim of thyroid tissue is focally seen compressed. There are fibrous bands within the neoplasm with foci of hemosiderin-laden macrophages. Capsular invasion and lymphovascular emboli are identified. There is focal pleomorphism, infrequent mitotic activity, and no tumor necrosis. The neoplastic cells are positive for GATA-3, Cam-5.2, PGP-9.5, and parathyroid H. BCL-2 is weakly expressed. The cells are negative for CDC73. About 5% of tumor cells are Ki67-positive. Resection margins were negative. The rest of the parathyroid glands showed parathyroid glandular tissue with chief cell hyperplasia. The right hemi-thyroid was negative for malignancy (Figure 3).
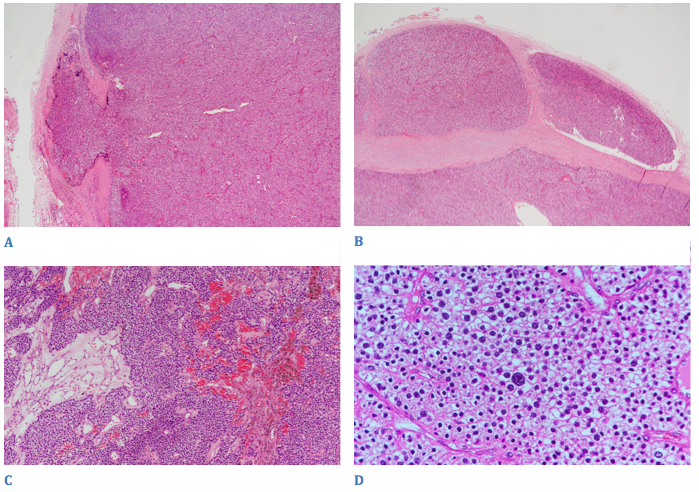
Figure 3
Clinical characteristics of patients on hemodialysis who happen to develop parathyroid carcinoma vary widely and have still not been understood completely (Zivalijevic et al. 2021). In the literature, there are 36 cases published to date of patients on hemodialysis who have been diagnosed with parathyroid carcinoma (24; 10, 15); The mean age of those patients at diagnosis is 49.4 years. The age of the patient in our study is 27 years. Up to our knowledge, there are only two cases in the literature of patients in their 20s with ESRD who were diagnosed with parathyroid carcinoma (Tseng et al., 1999 and Srouji et al., 2004). Furthermore, of the 36 cases reported, the majority of them were females (22 cases) (24 and our report is presenting another female case to the literature. This may propose that parathyroid carcinoma in ESRD has a female preponderance. However, further studies are required to claim this finding true. If parathyroid carcinoma is suspected, dissection of the central neck nodal compartment should be done [17]. Frozen section can be utilized to identify metastasis to lymph nodes, but because it has been associated with a high false-negative rate, it should not overtake clinical judgment. Usually, the recurrent laryngeal nerve can be preserved to maintain its function, however, if the tumor abuts or invades the nerve, it may require resection [5]. Chemotherapy has not been shown to have a role in the treatment of parathyroid carcinoma [7,2]. Some reported studies have shown effectiveness of monotherapy using dacarbazine or combination therapy, while other studies showed no response [16; 1]. The decision to go for adjuvant chemotherapy should be tailored to the individual, with appropriate counseling about the lack of supporting evidence. Likewise, adjuvant radiotherapy has not been shown to be effective in the treatment of parathyroid carcinoma [12]. Similar to adjuvant chemotherapy, the decision to treat with adjuvant radiotherapy should be individualized and discussed in a multidisciplinary team [5].
In the index case, CT staging has shown no local or distant metastasis; therefore, the decision was made to not treat with adjuvant chemotherapy or radiotherapy and keep the patient on close follow up and surveillance.
Parathyroid carcinoma is a rare entity and is challenging to diagnose. Patients with ESRD and hypercalcemia with sky-high PTH may have the suspicion for parathyroid carcinoma masked as those lab results can commonly get attributed to the ESRD itself. Moreover, it is important to note that the young age of the patient should not dismiss the possibility of parathyroid carcinoma.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
