
Research Article | DOI: https://doi.org/10.31579/2768-2757/087
1 Tauranga Hospital, Tauranga, New Zealand.
2 Auckland Hospital, Auckland, New Zealand.
3 Dunedin Hospital, Dunedin, New Zealand.
*Corresponding Author: Mark A Y F Pang, Middlemore Hospital, Counties Manakau District Health Board, Auckland, New Zealand.
Citation: Mark A. Y. F. Pang, Nicholas J. Fischer, (2023), Pancreatic and Duodenal Injuries: Experience at A Single Trauma Centre, Journal of Clinical Surgery and Research, 4(5); DOI:10.31579/2768-2757/087
Copyright: © 2023, Mark A Y F Pang. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 24 July 2023 | Accepted: 18 August 2023 | Published: 31 August 2023
Keywords: pancreatic injury; duodenal injury; trauma
Background:
Pancreatic and duodenal injuries are uncommon due to relative protection by their posterior anatomical position and have an incidence of less than 1% of all hospital admissions for trauma. Auckland City Hospital is a tertiary referral hospital in New Zealand with Trauma and Hepatopancreatobiliary units and admits approximately 384 patients with major trauma per year, predominantly from blunt mechanisms. This study is used to assess the incidence, diagnosis and clinical management of pancreatic and duodenal injuries in trauma patients at a single trauma centre.
Method:
A retrospective study was undertaken using data from a prospectively collected trauma registry. Inpatient notes including all patients admitted from 2007 to 2020 were reviewed. Pancreatic and duodenal injuries were graded using the American Association for the Surgery of Trauma (AAST) organ injury scale (OIS) grading system. Investigations including radiology and biochemistry and clinical management were noted.
Results:
A total of 45 trauma patients admitted to Auckland City Hospital had sustained pancreatic or duodenal injuries. Six patients had combined pancreaticoduodenal injuries, 16 had duodenal and 23 had pancreatic injuries. Grade I organ injuries were the most common in pancreatic (19/29) and duodenal injuries (9/22). Majority of patients underwent laparotomy (33/45) for associated haemodynamic instability. All organ specific indications for surgery occurred in Grade II and higher injuries. 10/45 patients were managed non-operatively, of which the majority had Grade I or II organ injuries (9/45). 3/45 patients died.
Conclusion:
The incidence of pancreaticoduodenal injuries is rare (45 patients in 13 years) and in keeping with trauma literature. In our series, haemodynamically stable patients with Grade I - II pancreatic and Grade I - II (non-laceration type) duodenal injuries did not require operative management. Endoscopic pancreatic stenting may facilitate selective non-operative management in some patients with pancreatic injury or complications.
Pancreatic and duodenal injuries are uncommon due to a relative protection offered by their posterior anatomical position and have an incidence of less than 1% of all hospital admissions for trauma [1]. Management of pancreatic and duodenal trauma is dependent on the severity of injury, which can be graded according to the American Association for the Surgery of Trauma (AAST) organ injury scale (OIS) grading system [1]. Operative management is indicated for pancreatic trauma that involves the pancreatic duct and may require pancreatic resection (Grade III – V) [2]. Duodenal haematomas can be managed non-operatively, however duodenal lacerations require surgical repair, and the method of which depends on the size and location of the defect. Primary closure using interrupted sutures is the most common approach (55-85%) [3,4]. Duodenal diversion has been used as an adjunct to primary repair. For example, pyloric exclusion which involves primary repair of the duodenum, closure of the pylorus and formation of a gastrojejunostomy [4]. Auckland City Hospital (ACH) is a tertiary referral hospital in New Zealand with Trauma and Hepatopancreatobiliary units and admits approximately 384 patients with major trauma per year (approximately 1537 patients for all traumas per year) [5]. The aim of this study was to examine all cases of pancreatic and duodenal injuries admitted to Auckland City Hospital, and to describe the diagnosis and clinical management and any long-term sequelae following these injuries.
A retrospective observational study was performed, assessing the clinical record, laboratory data, radiology imaging and reports. Patients with pancreatic and duodenal injuries were identified from the ACH trauma registry which prospectively records all patients admitted to ACH following trauma. All patients with pancreatic or duodenal injuries from 2007 to 2020 were included. The severity of injury was assessed according to the AAST OIS for pancreatic and duodenal injuries [1]. We noted the mechanism of injury, existence of concomitant injuries, diagnosis, management and complications. Patients were followed-up to assess for pancreatic and duodenal injury related complications using the electronic clinical record, which includes all presentations and correspondence for patients in the ACH and surrounding hospital catchments. Inclusion criteria included all patients with duodenal or pancreatic injuries from 2007 to 2020 admitted to ACH following trauma – confirmed by discharge diagnosis, imaging or intraoperative findings. Exclusion criteria excluded those that were thought to be duodenal or pancreatic injuries but subsequently found to have neither injuries, those with lack of notes or information in the records and those transferred from other hospitals for subsequent rehab. Data collection and simple analysis was performed in accordance with local ethical protocols.
55 patients were initially identified as having either pancreatic and/or duodenal injuries from the trauma database. In our exclusion criteria - seven patients were found to have no injuries, two patients had poorly documented notes and difficult to obtain the required information and one patient was transferred from another hospital for rehabilitation. A total of 45 patients had pancreatic or duodenal injuries during the 13-year study period (around 3.5/year). A total 23 patients had pancreatic injuries only, 16 patients had duodenal injuries only and six had combined pancreatic/duodenal injuries. Most patients were male 31/45 (68.8%) and the median age was 36 years (15 to 74). Most injuries were grade I or II (pancreatic and duodenal) [Table 1]. 23/29 (79%) patients with pancreatic injuries had serum amylase or lipase performed, of which the majority (n = 15) had elevated levels (65%).
| AAST Grade | Injury Type – (Number of patients) | |
| Pancreas n =29 | Duodenal n = 22 | |
| I | 18 | 8 |
| II | 6 | 8 |
| III | 3 | 6 |
| IV | 1 | - |
| V | 1 | - |
Table 1
Seven patients were transferred to ACH from other hospitals. Motor vehicle crash was the most common mechanism of injury (29/45) for pancreatic and duodenal injuries (Figure1). Five patients (11%) had penetrating injuries and 40 patients (89%) had blunt injuries [Figure 1]. All patients had cross-sectional computed tomography (CT). Five patients (11.1%) had magnetic resonance imaging (MRI) to ascertain if there was a pancreatic ductal injury. Four patients had an endoscopic retrograde cholangiopancreatography (ERCP). Most patients underwent laparotomy for haemodynamic instability (33/45), followed by organ specific indications including duodenal perforation or pancreatic ductal injury. For pancreatic injuries (n = 29), the majority had grade I and II injuries (n = 26) (Table 1). In total eight patients were managed non-operatively and 21 patients had an operation. Three patients underwent distal pancreatectomy for injury involving the pancreatic duct. Two patients with pancreatic duct injuries were managed with endoscopic pancreatic duct decompression using trans-ampullary pancreatic stents. No patients received octreotide.
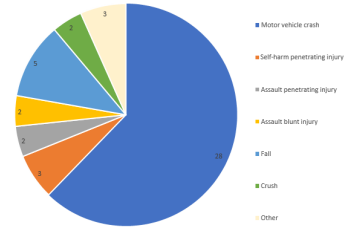
Figure 1: Mechanism of injury.
For duodenal injuries (n = 22), the majority (n = 16) had a grade I or II injury. Five patients were managed non-operatively, and 17 patients underwent an operation. Ten patients underwent primary closure of duodenal lacerations, of which four had pyloric exclusion with gastrojejunostomy procedures. One patient had a side-to-side duodenojejunostomy following a D2/3 injury (Table 2).
| Management | No. of patients | |
| Non-operative management | Non-operative management – ERCP | 2 |
| No intervention required | 10 | |
| Operative | Distal pancreatectomy | 3 |
| Bile ductrepair (+ subsequent AXIOS stent) | 1 | |
Primary repairof duodenal injury
| 10
| |
| Melecot catheter inserted into D3 perforation with a purse-string suture to createa controlled fistula + feeding NJ and draining NG placed | 1 | |
| Gastrostomy and repair of pancreatic laceration + stomach | 1 | |
| Multiple laparotomy + Side-wall duodenojejunostomy | 1 | |
| Exploratory laparotomy +/- repair of otherorgan injury | 18 | |
Table 2
12 patients (52%) had complications of pancreatic (Table 3) and seven (44%) had complications of duodenal injuries (Table 4). Three patients (10%) in our cohort with pancreatic injuries developed pancreatic collections which were drained. Three out of the six patients (50%) with combined injuries had complications (Table 4). In total three patients died, two patients with duodenal injuries and one patient with pancreatic injuries. Two patients died from sepsis and multiple organ failure (one pancreas and one duodenal), and one with duodenal injuries died from concomitant severe traumatic brain injury. (Table 3 + Table 5].
| Complications (Pancreatic injuries) | Management | Number of patients(%) n = 12 (23 patients in total) | |
| Post-operative complications | Post-operative collections by pancreatic bed | Percutaneous drainage | 1 (4.3%) |
| Ileus | Non-operative management – self resolved | 1 (4.3%) | |
| Pancreatic complications |
|
| 1 (4.3%) |
|
| 1 (4.3%) | |
|
| 1 (4.3%) | |
| Further surgery | Bowel obstruction | Laparotomy + devolving the small bowel volvulus | 1 (4.3%) |
| Bleeding | Laparotomy forcontrol of bleeding | 2 (8.7%) | |
| Wound dehiscence | Suture closure of the dehisced wound | 1 (4.3%) | |
| Death | Sepsis, multi-organ failure, adrenal insufficiency, DVT/PE | - | 1 (4.3%) |
| Other | Stress ulcer | Inpatient gastroscopy + proton pump inhibitor | 1 (4.3%) |
| DVT | Anticoagulation | 1 (4.3%) | |
Table 3
| Complications (Mixedinjuries) | Management | Number of patients (%) n = 3 (6 patients in total) | |
| Missedinjury | Missedtibia fracture | Open reduction and internal fixation | 1 (16.7%) |
| Furthersurgery | Bleeding | Laparotomy for control of bleeding | 1 (16.7%) |
| Missedretroperitoneal D3 injury at first laparotomy | Re-look laparotomy + primary repairof duodenal perforation with omental patch, pyloricexclusion and gastro-jejunal feeding tube and abdominal drains | 1 (16.7%) | |
Table 4
| Complications (Duodenal injuries) | Management | Number of patients (%) n = 7 (16 patients in total) | |
| Other | Iatrogenic injury from insertion of nasogastric tube –pneumothorax | Chest drain | 1 (6.3%) |
| Post-operative complications | Post-operative collections | Percutaneous drainage | 2 (12.6%) |
Non-operative management – resolved with antibiotics | 1 (6.3%) | ||
| Ileus | Non-operative management – self-resolved | 1 (6.3%) | |
| Death | Sepsis, multi-organ failure | - | 1 (6.3%) |
| Traumatic brain injury | - | 1 (6.3%) | |
Table 5
Pancreatic and duodenal injury is rare, occurring in less than 1% of all trauma admissions [1]. It has however been reported to have a high morbidity (36-60%) and mortality (18-23%) [6]. The pancreas is in retroperitoneum, shielded by the anterior abdominal wall and this is thought to be one of the reasons for low incidence of pancreatic injuries [4]. This may have implications of delayed diagnosis and is usually complicated by other intra-abdominal injuries [6-8]. Grading of pancreatic trauma is determined by the location of the injury and the presence of ductal damage [6]. Duodenal trauma is graded by injury thickness, extent of circumference of the lacerated lumen, and involvement of the common bile duct or ampulla [6]. Management of these injuries depend on the degree of injury. Clinical assessment and prompt diagnosis is important to minimise morbidity. A normal serum amylase has previously been reported to occur in up to 40% of patients with pancreatic trauma [1]. In our cohort, it was normal in 35% of patients, however this was limited by six patients that did not have a serum amylase or lipase measurement on admission. Having a baseline level for later comparison may still be of some value [1]. Cross-sectional imaging is necessary and surgical intervention may be required [1]. Contrast enhanced CT has a high specificity (90-95%) but low sensitivity for pancreatic ductal involvement (52-54%) [1]. Magnetic resonance imaging pancreatography (MRCP) can help with the diagnosis of ductal injuries [9]. Endoscopic retrograde pancreatography (ERP) can also identify pancreatic duct injuries, however, is more invasive and has an associated risk of morbidity. MRCP should be considered for detection of pancreatic duct injuries when a pancreatic injury is suspected on cross sectional CT imaging (sensitivity of 90-100%) [10]. ERCP has the additional benefit of allowing endoscopic treatment of a ductal injury, but this must be balanced by the associated risk of ERCP related morbidity [11]. Moreover, distal pancreatectomy is still considered the gold-standard treatment for pancreatic transection with ductal injury. ERCP and pancreatic stent placement can also be of benefit for management of complications of pancreatic injuries such as pseudocysts [11-13]. Five patients in our cohort had an MRCP to exclude ductal injuries, of which two patients were managed non-operatively after. It should be noted that even in patients with Grade I pancreatic injuries, other organs injuries were common in our cohort. As the pancreas sits in a retroperitoneal position, other intra-abdominal injuries complicated management and recovery [6-8]. For our cohort, 12/45 were managed non-operatively. This pancreatic duct fistula (distal tail) and duct stenosis (main body) was successfully managed with an endoscopic pancreatic stent placement. Grade IV and V injuries generally require operative management, with pancreaticoduodenectomy (Whipple’s procedure) being indicated if there is a massive disruption of pancreatic head [12,13]. Treatment for grade I and II duodenal haematoma can be managed non-operatively, but duodenal lacerations will require surgical repair [9,10]. Duodenal obstruction may occur with large mural haematoma formation [4]. The majority of grade II lacerations can be repaired by primary repair [4] [Figure 1], which in our cohort, all were. One patient was managed with primary repair and malecot drain insertion for decompression of D3. If the duodenum is unable to be repaired, then apancreaticoduodenectomy (Whipples’ procedure) may be indicated [4]. Weale et al noted in their retrospective study that 91 patients out of 94 had a primary repair [3]. Only three patients in their cohort had pyloric exclusion. However, the majority of patients in their series were injured from a penetrating mechanism and nearly all had AAST grade II injuries [3]. In comparison, in our series of predominantly blunt trauma, ten patients had primary closure and four of which had a pyloric exclusion, all with grade III injuries. In addition, one patient from our cohort had a side-to-side duodenojejunostomy. Complication rates for pancreatic trauma are variable and are reported to range from 26-86%, depending on severity [12,13]. The most common complication cited is a pancreatic fistula (10-35%) [1,10] which can be managed with drains [11-13], although persistent fistulas may benefit from endoscopic pancreatic duct stenting [12]. Other complications include post-traumatic pancreatitis, intra-abdominal abscess, and pseudocyst formation [1,11-13]. Three patients (10%) in our cohort with pancreatic injuries developed pancreatic collections which were drained. Only two patients in our cohort developed pancreatic fistula (7%). Søreide et al [10] noted the risk of mortality with grade I pancreatic injuries with no other injuries was < 5> 50% and mortality risk 20-50% [10]. Our overall mortality rate was 3 patients out of 45 (7%), and only two of these patients died as a result of complications attributable to pancreaticoduodenal injury (4%). Krig et al [2] have noted in that in their retrospective study of 473 patients – mortality rate was 15% and that deaths, whilst uncommon, occur late and due to multiorgan failure and sepsis which is in keeping with our data [2]. This study is limited by its retrospective data and that pancreatic and duodenal injuries are rare, even in trauma centres, and thus the actual number of cases were low (45 cases in 13 years). Three patients were transferred from regions outside of our ability to follow them up, thus it is possible that late complications in these three patients were missed.
Pancreatic and duodenal trauma is rare, in keeping with other current trauma literature [1]. Serum amylase/lipase may initially be normal in patients with pancreatic injuries. Based on our findings, haemodynamically stable patients with Grade I-II pancreatic and Grade I and non-laceration type Grade II duodenal injuries who have no other indication for surgical exploration can be successfully managed non-operatively. Endoscopic pancreatic stenting may facilitate selective non-operative management in some patients with pancreatic injury or complications.
ACH – Auckland City Hospital
AAST – American Association for the Surgery of Trauma
OIS - Organ injury scale
CT – Computed tomography
ERCP – Endoscopic retrograde cholangiopancreatography
MRCP – Magnetic retrograde cholangiopancreatography
No ethics approval was necessary as discussed with Auckland Hospital Research office as this study is based off an audit and it did not require any ethics approval.
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
The authors declare that they have no competing interests. This manuscript is not under consideration for publication elsewhere.
This manuscript did not have any sources of funding.
MP collected the data, analysed, reviewed the results and drafted the manuscript. NF designed the study, assisted with reviewing the data results and revised the draft. Both authors approved of the manuscript before submissions.
Not applicable.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
