
Research Article | DOI: https://doi.org/10.31579/2768-2757/110
North Manchester General Hospital, Department of Urology, Delaunays Road, Manchester, M8 5RB, United Kingdom.
*Corresponding Author: Anthony Kodzo-Grey Venyo, North Manchester General Hospital, Department of Urology, Delaunays Road, Manchester, M8 5RB, United Kingdom.
Citation: Grey Venyo AK, (2024), P63 Expressing Adenocarcinoma of The Prostate Gland, A Rare Neoplasm Which Tends to Pose Diagnostic Dilemma Sometimes: Review and Update, Journal of Clinical Surgery and Research, 5(4); DOI:10.31579/2768-2757/110
Copyright: © 2024, Anthony Kodzo-Grey Venyo. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 05 April 2024 | Accepted: 25 April 2024 | Published: 01 May 2024
Keywords: p63 expressing prostate cancer; prostate biopsy; histopathology examination; immunohistochemistry staining; ultrasound scan; computed tomography scan; magnetic resonance imaging scan; diagnostic dilemma; biological behaviour; further studies
It has been documented that prostate cancer is the world's leading cause of cancer and also the second commonest cancer in men which does tend to pose challenges in its diagnosis. It has been iterated that immunohistochemistry studies utilising tumour markers like high molecular weight cytokeratin, p63 aid in the diagnosis of prostate cancer. It has been known for some time that the absence of immunohistochemistry staining of prostate lesion for p63 and high molecular weight cytokeratin and presence of p504s in the biopsies indicate malignant lesions. Nevertheless, it had also been pointed out as well as documented that some rare cases of adenocarcinoma of prostate variants do demonstrate evidence of the tumour cells exhibiting p63 immunohistochemistry staining and this does pose a diagnostic dilemma that may make the unfamiliar pathologist mis-diagnose such a malignant tumour as a benign prostate lesion. p63-positive adenocarcinoma of the prostate gland is a major diagnostic pitfall. There is a danger of interpreting malignant glands as benign and arriving at a false-negative diagnosis. This can be prevented by the understanding of the pattern of immunohistochemistry staining expression related to this variant of prostate cancer. The major points that favour the diagnosis of carcinoma in these cases include: non-basal p63 staining and negative HWMCK and positive p504s staining. The biological behaviour of this particular rare variant of prostatic carcinoma is not certain and requires to be studied further into more detail. Considering the rarity of p63 expressing prostate cancers and the fact that most clinicians including pathologists, urologists, and oncologists would not have encountered a case of p63 expressing prostate cancer before in order to update all clinicians regarding this rare tumour, the ensuing article has been extensively written and divided into two parts: (A) Overview which has discussed general overview aspects of p63 expressing neoplasms and (B) Miscellaneous Narrations and Discussions from Some Case Reports, Case Series, and Studies Related to Primary p63 Expressing Adenocarcinomas of the Prostate Gland. A high-index of suspicion as well as knowledge of the histopathology examination features as well as immunohistochemistry examination features of this rare tumour is required from all clinicians. Knowledge of the treatment options, biological behaviour as well as outcome following treatment of the tumour has been extensively discussed as updating information. The update has clearly pointed out that further studies are required to determine the role of p63 overexpression in prognostication.
It has been iterated that with regard to men, carcinoma of the prostate gland represents the second most common cancer, after lung cancer. [1] It had also been documented that carcinoma of the prostate gland is also the world's leading cause of cancer [1] as well as that carcinoma of prostate gland is associated with advanced age, genetics factor smokers, obese individuals, and due to endogenous factors. [2] Prostate-specific antigen (PSA) levels are essential in elderly patients to identify the risk of prostate cancer. Though it is not very specific, high levels are concomitant with prostate cancer. Diagnosis of prostate cancer purely on the foundation of the clinical and morphological features is difficult. Here comes the role of the tumour markers and immunohistochemical markers. [3] Immunohistochemical markers such as p63, high molecular weight cytokeratin (HMWCK), and p504s aid in the appropriate diagnosis of prostatic cancers.
p63, an analogue of p53, is a tumour suppressor gene which encodes for isotypes which either act as p53-dominant negatives or transactivate p53 reporter genes, whose presence aids apoptosis and reduces the progression of cancer. [4] It comprises 15 exons and codes for 6 different mRNA isoforms which have a common DNA-binding domain. [3] [5] p63 is required for nourishing a basal-cell population, maintaining a prostate epithelial stem cell population, and is also essential for prostate development. [4] Markers like p53 and p63 are expressed on the nuclei of the normal basal cells. Usually, adenocarcinomas are devoid of basal cells, whereas benign lesions are encircled by the same. Hence, prostate adenocarcinoma can be differentiated from benign prostate lesions and hyperplasia by the absence of p63 staining in the basal cells in prostate carcinoma. Hence, p63 and HMWCK, and basal-cell immunohistochemistry markers turn out to be beneficial to distinguish benign and malignant conditions. [6] [7] Yet, there are few adenocarcinomas which retain the basal cells and have partial p63 and HMWCK staining, and there are a small number of Benign prostatic hyperplasia (BPH) and adenocarcinoma mimickers which don't express the basal-cell makers. [7]. Considering that p63 expressing adenocarcinomas of the prostate gland are rare, it would be envisaged that majority of clinicians working globally including Urologists, Oncologists, and pathologists may so far not have encountered this type of kidney neoplasm before. In view of this the ensuing article on primary p63 expressing carcinoma of the prostate gland has been written in two parts: (A) Overview which has discussed general overview aspects of p63 expressing neoplasms and (B) Miscellaneous Narrations and Discussions from Some Case Reports, Case Series, and Studies Related to Primary p63 Expressing Adenocarcinomas of the Prostate Gland.
To review and update the literature on primary p53 expressing carcinomas of the kidney.
Internet data bases were searched including: Google; Google Scholar; Yahoo; and PUBMED. The search words that were used included: p63 expressing adenocarcinoma of prostate; p63 expressing prostatic cancer; p63 expressing primary malignant neoplasm of prostate gland; and p63 expressing primary prostatic malignant neoplasm. Forty-four (44) references were identified which were used to write the article which has been divided into two parts: (A) Overview which has discussed general overview aspects of p63 expressing neoplasms and (B) Miscellaneous Narrations and Discussions from Some Case Reports, Case Series, and Studies Related to Primary p63 Expressing Adenocarcinomas of the Prostate Gland.
A] Overview [8]
Definition / general statement [8]
Essential features [8]
The essential features of p63 expressing prostate cancer tumours had been summated as follows: [8] [9] [10]
Epidemiology
Laboratory tests [8]
Prognostic factors
The factors of prognostication, had been summated as follows: [8]
Microscopic (histologic) description
The microscopy histopathology examination features of p63 expressing prostate cancer had been summated as follows: [8]
Immunohistochemistry staining
The immunohistochemistry staining features of p63 expressing prostate cancers had been summated as follows: [8]
Positive stains
Negative stains
The negative immunohistochemistry staining features of p63 expressing prostate cancers had been summated as follows: [8]
Molecular / cytogenetics description
The molecular and cytogenetics study features of p63 expressing carcinoma of the prostate gland had been summated as follows: [8]
Differential diagnoses
The differential diagnoses of p63 expressing prostate cancer had been summated as including the ensuing: [8]
[B] Miscellaneous and Discussions from Some Case Reports, Case Series, And Studies Related to P63 Immunonogistochemistry Expressing Carcinoma of The Prostate Gland
Osunkoya et al. [9] stated that aberrant diffuse immunohistochemistry expression of p63 in prostate carcinoma cells is a rare and poorly understood phenomenon.
Osunkoya et al. [9] studied 19 cases of prostate cancer with aberrant diffuse expression of p63 which were diagnosed based upon pathology examination of specimens of prostate needle biopsy and they reviewed the subsequent radical prostatectomies in 6 cases. They reported on 19 out of 21 cases, and they reported that 100perecentage of the cancer nuclei had stained intensely for p63, with 70perecentage staining in the remaining 2 cases. Two additional radical prostatectomies with aberrant p63 staining with no needle biopsies available for review were also analysed by
Osunkoya et al. [9]. On the hematoxylin and eosin-stained slides, 19 out of 21 cases that amounted to 90.5% of the cases had demonstrated a distinctive morphology composed predominantly of glands, nests, and cords with atrophic cytoplasm, hyperchromatic nuclei, and visible nucleoli. Osunkoya et al. [9] also reported the following results:
Giannico et al. [10] stated that prostatic adenocarcinoma with aberrant diffuse expression of p63 (p63-PCa) had been a recently described variant of adenocarcinoma of prostate gland. Giannico et al. [10] undertook a study to investigate the clinical and pathological features of p63-PCa at radical prostatectomy (RP). Giannico et al. [10] reviewed 21 cases of p63-PCa diagnosed based upon needle biopsy at subsequent RP. Giannico et al. [10] undertook immunohistochemical analysis for PIN4 and Ki-67 in all RP cases. Giannico et al. [10] reported the following results:
Giannico et al. [10] summated that they had recommended that these tumours should not be assigned a Gleason score and their favourable findings at RP should be noted.
Baydar et al. [11] iterated that prostate carcinomas exhibiting aberrant diffuse-nuclear p63 expression were extremely rare, and there was only 1 article in the literature reporting a series of 21 such cases by the time of publication of their article in 2011. Baydar et al. [11] iterated that they had documented an additional case of p63-positive prostatic adenocarcinoma in a 60-year-old man, whose diagnosis was difficult. They reported that the patient was found to have an elevated serum prostate-specific antigen (PSA) level at a general health check-up and he was then referred to the hospital. His serum PSA was 4.2 ng/mL. He underwent digital rectal examination and transrectal ultrasound scan which did not demonstrate a lesion. He underwent trans-rectal needle biopsy of the prostate gland and pathology examination of the biopsy specimens identified atypical, small prostatic glands which were suspected for adenocarcinoma at 2 cores. Nevertheless, immunohistochemistry staining studies of the biopsy specimens had demonstrated nuclear p63 expression within the suspicious glands. Repeat biopsy of the prostate lesion upon pathology examination had demonstrated only high-grade prostatic intraepithelial neoplasia. In the third transrectal biopsy, finding of the same atypical glands demonstrating perineural invasion had facilitated the diagnosis of malignancy. The patient underwent a radical prostatectomy. Five different small tumour foci were identified within the prostate after pathological evaluation, one of which was p63 positive staining and the others p63 negative staining. The largest of the classic p63-negative tumours had shown a TMPRSS2-ERG translocation by fluorescent in situ hybridization while the p63-positive tumour did not. Baydar et al. [11] had iterated that this subtype (p63-positive prostate adenocarcinoma) should be listed among the recognized rare variants of adenocarcinoma of the prostate gland.
Khalid et al. [12] stated the following:
Khalid et al. [12] reported a 76-year-old Chinese man, who had attended the clinic with a manifestation of swelling over his right buccal mucosa with on and off pain and numbness at his right chin in December 2017. His symptoms had commenced two months preceding his attendance at the clinic. It was found upon his examination that clinically his buccal mucosa was smooth, and a well-defined firm mass could be palpated over his normal overlying buccal mucosa (see Figure 1). He was completely edentulous with no restriction of his mouth opening.

Figure 1: Intraoral photograph showing smooth, well-defined, firm mass over the right buccal mucosa with normal overlying mucosa. Reproduced from: [12] Under the Creative Commons Attribution License.
The patient was documented to be a known case of end-stage prostate cancer. He was initially diagnosed with adenocarcinoma of the prostate gland in June 2014 via pathology examination of specimens of his trans-urethral resection of his prostate (TURP) gland. The Gleason score of his prostate cancer was 4+5 = 9, and his serum prostate-specific antigen (PSA) was high (65 ng/mL). he had an isotope bone scan in July 2014 which had demonstrated multiple bone metastases involving his left 4th rib, 4th lumbar spine, sacrum, and left pubic bone but which had not involved his mandible. He was treated with androgen deprivation therapy (Lucrin) until December 2015, and his treatment was followed by seven months of antineoplastic agents (Abiraterone acetate) from December 2016 to July 2017 due to his persistent high baseline of serum PSA value >100 ng/mL. His prostate cancer disease had progressed and the patient was treated with non-steroidal antiandrogen (Enzalutamide) from July 2017. His serum PSA value did not respond to the treatment he had. By October 2017, his serum PSA level was 120 ng/mL, which had coincided with his first clinical symptom of numb chin syndrome. He underwent a cone-beam computed tomography (CBCT) scan which had demonstrated erosion of bone within the anterior part of his ascending ramus and retromolar region (see Figure 2). An incisional biopsy of the lesion was then undertaken for pathology examination.

Figure 2: CBCT image showing erosion of bone at the anterior part of right ramus of mandible and retromolar region. Reproduced from: [12] Under the Creative Commons Attribution License.
Pathology examination of the haematoxylin and eosin (H&E) slides of his biopsied lesion demonstrated tumour islands that consisted of central cells with hypo-chromatic and vacuolated nuclei, pale eosinophilic cytoplasm, and this had exhibited pleomorphism. The peripheral basal tumour cells were found upon pathology examination to be spindle-shaped and appeared hyperchromatic (see Figure 3), with areas of extensive comedonecrosis visualised. The central tumour cells had exhibited immunohistochemistry staining positivity for PSA (see Figure 4A) and cytokeratin (CK; weak). The peripheral basal tumour cells were noted to have exhibited immunohistochemistry staining positivity for PSA, CK (weak), and p63 (scattered) (see Figure 4B). Both the central tumour cells and the basal tumour cells had exhibited negative staining for CK7 and CK20. Considering the H&E and immunohistochemistry manifestation of the case, a diagnosis of adenocarcinoma metastasis from the prostate was reported.

Figure 3: Photomicrograph shows a tumour island consisting of central round cells and peripheral spindle (magnification x100, stain A&E). Reproduced from: [12] Under the Creative Commons Attribution License.

Figure 4: Photomicrographs showing (A) immunopositive cytoplasmic staining of tumour cells with PSA (magnification x100) and (B) scattered immunopositive staining of tumour cells with p63 (magnification x100). Reproduced from: [12] Under the Creative Commons Attribution License.
The attending oncologist was informed of the metastatic finding. Following this, the patient underwent a computed tomography (CT) scan and isotope bone scan (see Figure 5A and 5B) which demonstrated
multiple bone metastases to his sternum, ribs, ilium, femur, and vertebrae as well as his mandible. Subsequently, patient received chemotherapy treatment. Nevertheless, three months later, unfortunately, the patient died as a sequel of hi tumour.

Figure 5: Bone scan images (A) anteroposterior view and (B) posteroanterior view showing multiple distant bone metastases to the mandible, sternum, ribs, ilium, femur and vertebrae. Reproduced from: [12] under the Creative Commons Attribution License.
Khalid et al. [12] made the ensuing educative summative iterations:
Khalid et al. [12] made the ensuing conclusions:
Ferronika et al. [13] stated the following:
Ferronika et al. [13] reported that they had utilised a cross-sectional study during two years between 2009 and 2010, and they had investigated a total of 79 paraffin embedded tissues of benign prostatic hyperplasia, PIN prostatic intraepithelial neoplasia, low and high Gleason score prostate cancer by means of immunohistochemistry staining studies. Ferronika et al. [13] also analysed the associations between cytoplasmic p63 and ALDH1A1, as well as with pathological diagnosis, by undertaking Chi-Square test using SPSS 15.0. Links of both markers with cell proliferation rate (KI-67) and apoptotic rate (cleaved caspase 3) were also analyzed by Kruskal-Wallis test. Ferronika et al. [13] summated their results as follows:
Dhillon et al. [14] stated the following:
Fonseca-Alves et al. [38] reported that in their study, p63 immunohistochemistry staining expression was investigated in 90 canine PCs and 20 normal prostate tissues (NT). Fonseca-Alves et al. [38] also reported that the p63 expression pattern in luminal or basal cells was confirmed in a selected group of 26 PCs and 20 NT by immunohistochemistry and/or Western blotting assays. They had compared eleven canine PC samples aberrantly expressing p63 (p63+) in secretory cells with 15 p63 negative (p63-) cases in the context of several molecular markers (high molecular weight cytokeratin-HMWC, CK8/18, CK5, AR, PSA, chromogranin, NKX3.1, PTEN, AKT and C-MYC). Fonseca-Alves et al. [38] summarised their results as follows:
Fonseca-Alves et al. [38] made the ensuing conclusions:
Wu et al. [6] reported a case of adenocarcinoma of prostate gland that showed diffuse aberrant p63 expression within the secretory cells and they reviewed the literature and differential diagnosis. Wu et al. [6] made the ensuing iterations:
Tan et al. [5] described a rare group of prostate adenocarcinomas that had exhibited an aberrant expression of p63, a protein strongly which is expressed in prostatic basal cells and absent from usual-type acinar prostate cancers. Tan et al. [5] stated the following:
Tan et al. [5] made the following conclusions:
Torres et al. [39] stated the following:
Torres et al. [39] compared a total of 8 p63-expressing prostate carcinomas at radical prostatectomy to 358 usual-type adenocarcinomas by gene expression profiling performed on formalin fixed paraffin embedded tumour tissue using Affymetrix 1.0 ST microarrays. Correlation between differentially expressed genes and TP63 expression was performed in 5239 prostate adenocarcinomas available in the Decipher GRID. For validation, ETS2 in situ hybridization was undertaken on 19 p63-expressing prostate carcinomas and 30 usual-type adenocarcinomas arrayed on tissue microarrays (TMA). Torres et al. [39] summarised the results as follows:
Lokesha et al. [1] iterated the following:
Lokesha et al. [1] reported an 87-year-old, diabetic, as well as a known hypertensive gentleman who had manifested with incomplete voiding, increased urinary urgency, and frequency of micturition, together with bilateral pitting type of oedema which was confined to his feet and dull and deep generalized pain within his lower abdomen which appeared following his voiding of urine. The result of his serum PSA level had significantly increased to 213.3 ng/ml. Upon digital rectal examination, a Grade 3 prostate enlargement and hard prostate were felt. He underwent trans-rectal prostate biopsies which were obtained for histopathology examination. Pathology examination of his prostate biopsy tissue cores demonstrated a tumour which had comprised of back-to-back arranged small glands without basal-cell layer. The epithelial lining had demonstrated enlarged hyperchromatic nuclei with prominent nucleoli (see figure 6 and 6 b).

Figure 6: (a and b) Hematoxylin and eosin staining of the prostatic tissue exhibiting tumour composed of back-to-back arranged small glands without basal cell layer and epithelial lining showing enlarged hyperchromatic nuclei with nucleoli [200 × magnification] Reproduced from [1] under the Creative Commons Attribution License.
Immunohistochemistry staining study analysis was undertaken to evaluate the biopsy for the presence of basal cells with HMWCK and p63. A positive tumour marker p504s was also undertaken.
To the surprise of the authors, the nuclei of the tumour cells had exhibited positivity with p63 causing confusion [see figures 7 a and b]. The HMWCK study demonstrated negative staining within the cancerous glands [see figure 8] and p504s was diffusely and strongly positive [see figures 9 a and b].

Figure 7: (a and b) Photograph of the prostatic tissue [1b showing a magnified image] where nuclei of the tumour cells demonstrate p63 positivity [immunohistochemistry, 100 × magnification].

Figure 8: Glands of the tumour cells demonstrating negativity for high molecular weight cytokeratin [100 × magnification].
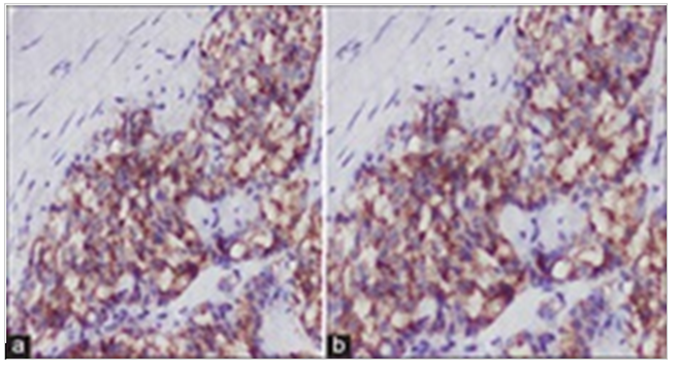
Figure 9: (a and b) Glands of the tumour cells [4b showing a magnified image] showing diffuse positivity for p504s molecular marker [100 × magnification].
Lokesha et al. [1] stated that upon review of literature, it was evident that a rare variant of adenocarcinoma of the prostate gland called p63-positive prostatic carcinoma could exhibit p63 overexpression within the nuclei of the malignant glands. They also found out upon review of the literature that this tumour entity could be distinguished from benign glands by the
fact that the expression of p63 is not basal in nature and the glands had exhibited negative reaction with HMWCK. A positive p504s staining also supports the malignant diagnosis. Lokesha et al. [1] iterated that in concordance with the immunohistochemical and histopathological findings, the case was confirmed to be a diagnosed case of p63-positive adenocarcinoma of prostate gland. The patient was managed mainly by means of chemotherapy, injection pamorelin (11.25 mg, intramuscular), tablet finast, tablet silodac, and tablet tabi for a month. Currently, the patient at the time of publication of his case had been undergoing regular follow-up assessments and he was asymptomatic.
Lokesha et al. [1] made the ensuing educative discussions:
Lokesha et al. [1] made the ensuing conclusions:
- Nil
Acknowledgements to:
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
