
Research | DOI: https://doi.org/10.31579/2693-4779/101
1 Institute of Tropical Medicine “Pedro Kourí” (IPK), Havana, Cuba.
2 Center for State Control of Medicines, Medical Equipment and Devices (CECMED), Havana, Cuba.
3 Departamento de Ciencias Farmacéuticas, Facultad de Ciencias, Universidad Católica del Norte, Antofagasta, Chile.
*Corresponding Author: Gabino Garrido, Departamento de Ciencias Farmacéuticas, Facultad de Ciencias, Universidad Católica del Norte, Angamos 0610, Antofagasta, Chile.
Citation: Rosario Gravier Hernández, Erik Pérez García, Olga Castaño Araujo, Angélica Reyes Pérez, Daisy Agete Estrada. (2022) Oxidative stress in hemodialysis patients infected with HIV. Clinical Research and Clinical Trials. 6(2); DOI: 10.31579/2693-4779/101
Copyright: © 2022 Gabino Garrido. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 May 2022 | Accepted: 03 June 2022 | Published: 10 June 2022
Keywords: oxidative stress; hemodialysis; Human Immunodeficiency Virus; Chronic Kidney Disease; antioxidant
Background: HIV-infected population presents the impaired renal function as a risk factor for death, and comorbid conditions are related in some traits to oxidative stress (OS).
Objetive: To analyze the influence of OS in Human Immunodeficiency Virus Infection (HIV) and chronic kidney disease (CKD) by comparing the redox status between HIV patients with and without CKD and HIV hemodialysis patients.
Methods: A comparative longitudinal study of the hemodialysis process was developed. The study included 96 individuals divided into four groups namely, supposedly healthy volunteers, patients with HIV infection without renal illnesses, patients with HIV infection and chronic renal disease, and HIV(-) with chronic renal disease. Indexes evaluating redox, hematological, hemochemical, immunologic, and virological aspects were determined. These indexes were also assessed before and after hemodialysis.
Results: Viral load, uric acid, creatinine, and urea concentration were significantly (p<0.05) lower after hemodialysis. The two HIV infected groups were significantly different (p<0.05) regarding redox indexes of damage and antioxidant status compared to the group of supposedly healthy volunteers. Significantly increased values (p<0.05) of malondialdehyde, advanced oxidation protein product (AOPP), and peroxidation potential (PP) and significantly lower values glutathione (GSH) (p<0.05) were found after hemodialysis in both groups. In the case of HIV patients, increased values of superoxide dismutase were also found. HIV infected patients under HD tretament exhibited significantly (p<0.05) higher values of AOPP and PP and lower values of GSH than HIV(-) hemodialysis patients after hemodialysis.
Conclusion: Oxidative stress occurs in both HIV and CKD conditions, and it is also increased after hemodialysis intervention. Otherwise non-viral control could influence on oxidative status in HIV/CKD patients, that´s why ART affectivities should be monitoring using HIV progression markers. Redox indexes should be diagnosed in HIV hemodialysis patients for treatment and management adjustment.
OS: Oxidative stress
HIV: Human Immunodeficiency Virus Infection
CKD: Chronic kidney disease
ART: Antiretroviral therapy
HD: Hemodialysis
SHV: Supposedly healthy volunteers
HIV/CKD: Chronic kidney disease
nHIV/CKD: Chronic kidney disease non-HIV patients
IRT: Nucleoside reverse transcriptase inhibitors
PI: Protease inhibitor
GSH: Reduced glutathione
MDA: Malondialdehyde
PP: Peroxidation potential
HPO: Total hydroperoxide
SOD: Superoxide dismutase activity
CAT: Catalase activity
AOPP: Advanced oxidation protein products
Introduction
Kidney-related diseases are common in patients with different comorbidities and affect many people worldwide (Lameire et al., 2013). Patients infected with Human Immunodeficiency Virus (HIV) are more vulnerable to chronic kidney disease (CKD). Its main consequences include the loss of renal function, which leads to end-stage renal disease; an increased risk of cardiovascular disease; a significant increment in morbidity and mortality; and a decrease in health-related quality of life (Cohen, Kopp, & Kimmel, 2017).
General population, and especially HIV-infected people, presents the impaired renal function as a risk factor for death. Acute kidney injury is frequent in HIV and is commonly the result of sepsis, dehydration, and drug toxicities. Furthermore, HIV itself increases the risk of CKD (Islam, 2012). CKD is one of the most important non-infectious comorbidities of HIV infection. In addition, antiretroviral therapy (ART) contributes to the development of CKD in HIV patients due to antiretroviral toxicity. The risk of CKD relates not only to the use of specific ART but also to an individual's comorbid conditions and aging influencing in some traits by oxidative stress (OS) (Heron, Bagnis, & Gracey, 2020; Wearne, Davidson, Blockman, Swart, & Jones, 2020).
Increased OS has been implicated in a wide range of diseases and suggested as a cofactor during the course of HIV Infection course involved in many aspects of disease pathogenesis (Anthony & Ashok, 2011; Coaccioli et al., 2010; Palipoch & Koomhin, 2015). OS results from an imbalance between oxidant and antioxidant production favoring the oxidation process. Sustained OS contributes to cell and tissue damage, which is mediated by redox circuits and attempts to cellular structure and function. It could be a component in the pathophysiology behind a multitude of diseases as an origin or a consequence factor (Al-Dalaen & Al-Qtaitat, 2014). Also, oxidized biomolecules accumulation takes place in patients with chronic renal failure. OS and subclinical inflammation are crucial factors for renal failure development (Daenen et al., 2019; Krata, Zago ˙zd ˙zon, Foroncewicz, & Mucha, 2018; Silva Í et al., 2021).
High levels of OS have already been found in the early stages of CKD, which increase in parallel with the progression of the disease, and are further exacerbated in hemodialysis (HD) patients (Liakopoulos, Roumeliotis, Gorny, Dounousi, & Mertens, 2017). Oxidative disequilibrium is a common hallmark in renal disease. OS could be both a potential cause and a consequence of renal function alteration. The kidney has a high metabolism that is extremely vulnerable to oxidative damage, and OS can cause/accelerate disease progression. It may also be partly responsible for complications associated with the disease, such as hypertension, anemia, atherosclerosis and related cardiovascular disturbances, neurological disorders, impaired immunity, and hemostatic abnormalities (Pedraza-Chaverri, Sánchez-Lozada, Osorio-Alonso, Tapia, & Scholze, 2016). For this reason, OS has become an important diagnostic and prognostic factor and is a target for CKD prevention/treatment.
OS has a critical role in both, pathophysiology of several kidney diseases and many of associated complications. OS-related mediators and inflammation, in patients with renal failure are related to the underlying disease itself. Redox imbalance appears in the early stages of CKD mainly identifying tissular damage, goes forward exacerbating renal failure, and further deteriorates by the HD process per se (Ebert et al., 2021; Liakopoulos et al., 2017; Silva Í et al., 2021; Tomás-Simó et al., 2021). They are chronically exposed to the high-grade OS during regular dialysis performance requiring the presence of a central venous catheter and the use of bio-incompatible dialyzers and bloodlines (Epifânio, Balbino, Ribeiro, Franceschini, & Hermsdorff, 2018; Liakopoulos et al., 2017). During HD, massive repeated blood exposure to dialyzer membranes and dialysate trigger activation of complement factors, platelets and polymorphonuclear white blood cells, and subsequently ROS production, within minutes after initiation of HD sessions. In addition the dysfunction of the mitochondrial respiratory system, which is prominent in CKD patients and further impaired in HD patients, might be the cause of ROS generation. Also the enhanced oxidative status that characterizes HD patients has been associated to poor dietary intake of exogenous antioxidants, accumulation of oxidative products, and loss of antioxidant molecules during HD(Liakopoulos et al., 2017).
Although biochemical evaluation of oxidative status might be relevant for the prognosis and therapeutic approach of HIV/HD patients, few articles about the topic are reported. To analyze the influence of OS in HIV and CKD by comparing the redox status between HIV patients with and without CKD and HIV hemodialysis patients.
Design, protocol, and patient management
A comparative longitudinal study was designed to recruit non-HIV and HIV/AIDS infected individuals. All the patients were selected from the HIV patients consult at the Institute "Pedro Kourí" (IPK) Hospital. They all signed a written informed consent to participate in the study after a verbal explanation of its methods and risks. The work was accomplished by a multidisciplinary team, including clinical physicians in HIV/AIDS handling. Protocols were previously reviewed and approved (CEI-IPK) by the Institute "Pedro Kourí" Committee for Research on Human Subjects. The proposal considered the principle of the Declaration of Helsinki concerning the Ethical Principles for Medical Research Involving Human Subjects. The protocol was also approved by the Determinant Program of the Cuban Ministry of Health.
Patients' inclusion
Non-probabilistic convenient inclusion was used according to the assistance of patients to the HIV-specialized clinic in the Hospital. The recruitment criterion for HIV infected patients were HIV-1 antibodies confirmed by Western Blot. Patients with CKD were classified following the criteria of K-DOQUI 2002 (National Kidney Foundation, 2002). HD patients included had glomerular filtration rates ≤ 15 mL/min and had been receiving HD for less than 3 years. All HD patients were receiving HD in the IPK Hospital, lasting 4 hours, with blood flow greater than 250 mL/min and dialysate flow of 500 mL/min. HD was performed with medium flow polysulfone membrane filters F-series High-performance steam, with a surface area matched to the body surface area of each patient. As exclusions criteria were considered: smokers, history of drug use (including vitamins, iron, or antioxidant supplements), pregnant and lactating women, co-infections, and patients with other pathologies. Ninety-six subjects ranging from 30-50 years of age were enrolled sequentially. The individuals were divided into four groups: 24 supposedly healthy volunteers (SHV), 24 HIV infected patients with viral control without renal illnesses (HIV), 24 HIV infected patients with chronic kidney disease (HIV/CKD), and 24 chronic kidney disease non-HIV patients (nHIV/CKD). All HIV patients were evaluated at the clinical site. Anthropometry and laboratory tests were developed for each subject included in the study.
Patients were evaluated through different aspects: diet and supplemental intake history, anthropometric data (weight, height), and clinical lab results. Demographic and age data were extracted from SIDATRAT (software package 2008). Subjects were stratified according to gender, age, ethnicity, viral load, and CD4+ T lymphocyte subset count. The lab variables of HD patients were assessed before and after the HD session.
Treatments
The antiretroviral (ARV) schedule consisted of a triple-drug variant distributed free, including two nucleoside reverse transcriptase inhibitors (IRT) and one protease inhibitor (PI) stated according to current national guidelines. The ARV drugs recommended in the combinations were oriented at the following doses per day: lamivudine 150 mg, abacavir 600 mg, lopinavir 800 mg/ritonavir 200 mg, atazanavir 300 mg/ritonavir 100 mg.
Flow cytometry analysis
Total blood was utilized to study T lymphocytes subsets CD3+/CD4+. For each T lymphocyte subsets, double marks were used. The analyses were performed with a Cyflow Space Cytometer (PARTEC GmbH, Münster, Germany) by FloMax 2014 using Versión 2.9 program.
HIV-RNA plasma viremia (viral load)
Biomerieux polymerase chain reaction (PCR-NASBA) was applied to determine the HIV viral load using an ultrasensitive assay with the lower quantification limit of 50 IU.
Oxidative stress indexes
Samples of venous blood were taken from fasted patients in mornings between 8.00 and 10.00 hours after signing the informed consent. Blood samples were extracted by venipuncture into heparin-treated tubes, and serum was obtained after centrifugation.
Superoxide dismutase and catalase activities assays were developed in erythrocyte cells that were extracted from hemolysate. For the rest of the indexes, 3 mL of serum was used. Serum samples were preserved at –70°C and secured from light exposure until analyses were accomplished. All redox indexes were determined by spectrophotometric procedures using a Spectro-photometer Zuzi 4211/50 (Japan).
Glutathione concentration
Serum reduced glutathione (GSH) was evaluated by the spectrophotometric method after the reaction with 5,5’-dithiobis (2-nitrobenzoic acid) (Motchnik, Frei, & Ames, 1994). The analysis of the reduced chromogenic was assessed at 412 nm and it was directly proportional to the GSH concentration. GSH (Sigma, St. Louis, M.O., USA) was used to produce standard curves.
Malondialdehyde
Malondialdehyde (MDA) concentrations were detected with the LPO-586 kit from Calbiochem (La Jolla, CA, USA). Concentrations of MDA in serum samples were evaluated using the corresponding standard curve, and values were expressed as nmol/g Hb (Erdelmeier, Gerard, Yadan, & Chaudiere, 1998).
Peroxidation potential (PP)
To calculate the sample susceptibility to lipid peroxidation, each serum was incubated with a solution of cupric sulfate (final concentration of 2 mM) at 37°C for 24 h. The PP was determined by subtracting the MDA concentration at time 0 from the one obtained at 24 h (Bartosz, 2003).
Total hydroperoxide (HPO)
HPO was measured using Bioxytech H2O2-560 kitCat.21024 (Oxis Internacional Inc. Portland, USA). The assay considered the oxidation of ferrous ions to ferric ions by hydroperoxides under acidic conditions. In this assay, peroxide first reacts with sorbitol (which provides sensitivity enhancement), producing a peroxyl radical, which generates Fe3+ (Jiang, Woollard, & Wolff, 1991).
Superoxide dismutase activity
SOD activity was evaluated by the method of Marklund. This method generates the inhibition of auto-oxidation of pyrogallol by SOD (Marklund & Marklund, 1974). One unit of SOD activity is considered as the amount of the enzyme required to inhibit the rate of pyrogallol autooxidation by 50%.
Catalase activity
CAT activity was determined using the method of Clairbone (1986) (Clairborne, 1986). Catalase activity was expressed as U mg/Hb.
Advanced oxidation protein products (AOPP) concentration
Serum AOPP was evaluated using the methods of Witko-Sarsat et al. (1998) (Witko-Sarsat et al., 1998). The values were expressed in chloramine T equivalents and corrected by serum albumin concentrations.
Biochemical indexes
Blood indexes such as hematocrit, hemoglobin, and complete blood count-differentiation and erythrocyte sedimentation rate were assessed by Hematological counter MICROS 60. Others like triglycerides, creatinine, cholesterol, glucose, uric acid, urea, lactate dehydrogenase, and aspartate and alanine aminotransferase activity were assessed by standard methods in HITACHI analyzer 912 in the clinical laboratory of IPK Hospital.
Statistical analyses
Descriptive statistics of continuous variables as means and standard deviations were calculated, whereas categorical variables proportions were calculated. The normality of variables was calculated by the Kolmogorov-Smirnov test. Comparisons between groups were determined using the Kruskal-Wallis test, followed by a post hoc Dunn's Multiple Comparison Test. Pearson correlation coefficient was used to evaluate the relationship among the different indexes combining redox and follow-up parameters. Statistical significance was defined as p < 0>
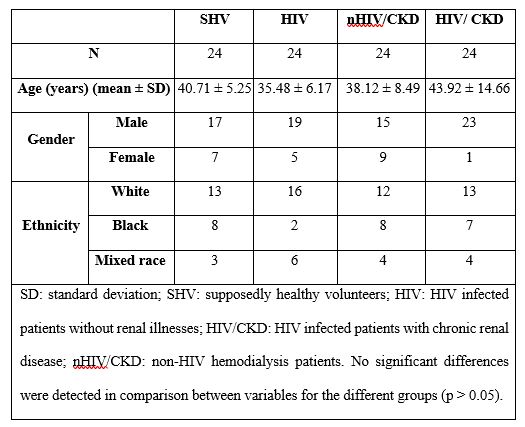
Table 1 shows the age, gender, and ethnicity data of the 96 subjects divided in their corresponding groups. There were no statistically significant differences among the groups according to demographics such as ages, gender, ethnicity, and the number of patients (p ˃ 0.05). A major percent of patients in the groups were males over 35 years of age and of white skin color.
All subjects were seronegative for other co-infections. The etiology of kidney disease in non-HIV patients was related to diabetes mellitus (37.5%), hypertension (37.5%) or polycystic kidney (25%). Meanwhile, in the case of HIV patients the etiology of kidney disease was related to diabetes mellitus (25%), hypertension (12.5%) or nephropathy associated to HIV infection (62.5%). Other comorbidities/complications were not present in the patients with CKD during the study. At the moment of the research, concomitant drugs (including alcohol) or antioxidant supplementation were not reported. When the period living with HIV is analyzed, 16% of the patients had less than 5 years, 42 between 5 and 10 years, and 42 more than 10 years from the diagnosis of the infection. All patients reported taking the drugs according to the doctor's prescribed regimen. 82 of HIV patients were on rescue-regimen for primary virological failure, the other 18 used first line ARV schedule.
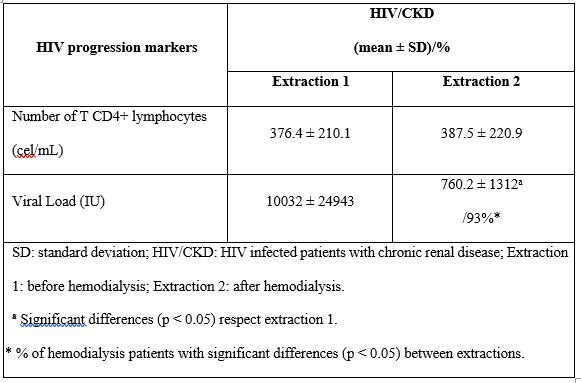
The progression markers of HIV are shown in Table 2. HIV viral load was significantly lower (p < 0>
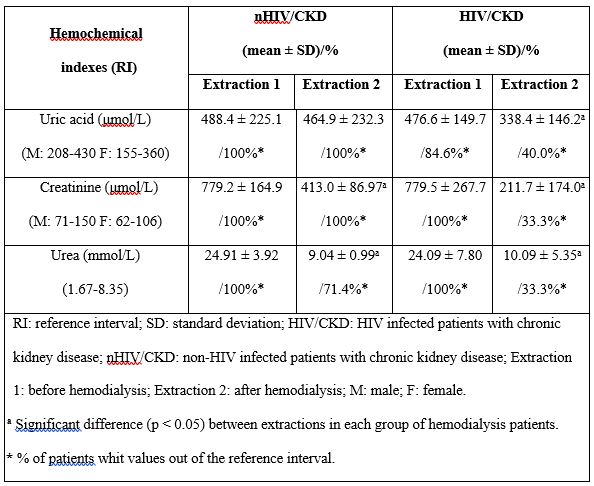
Hemochemical index data of HIV/CKD patients and nHIV/CKD patients before and after hemodialysis are showed in Table 3. Hemoglobin, hematocrit, complete blood count-differentiation, and erythrocyte sedimentation rate media values from these groups of patients abided on intervals recognized as physiological-reference without significant differences (p > 0.05) after HD (not presented data). The same behaviors were found in triglycerides, cholesterol and glucose concentration, lactate dehydrogenase, aspartate, and alanine aminotransferase activity (not presented data). Creatinine and urea concentrations were significantly (p < 0>
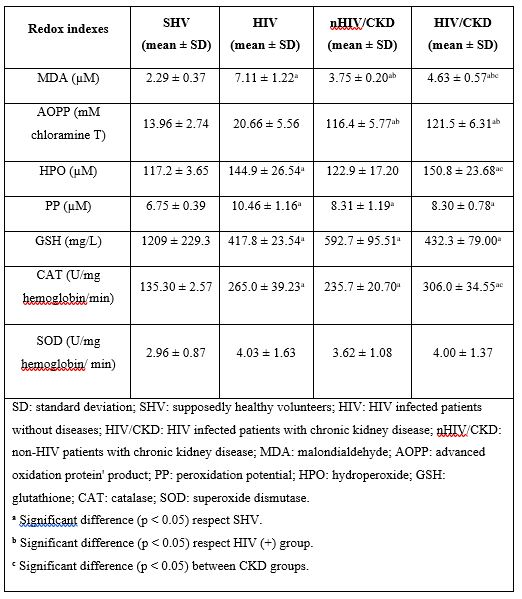
Redox index data of the different studied groups are shown in Table 4. All groups exhibited significantly higher (p < 0>
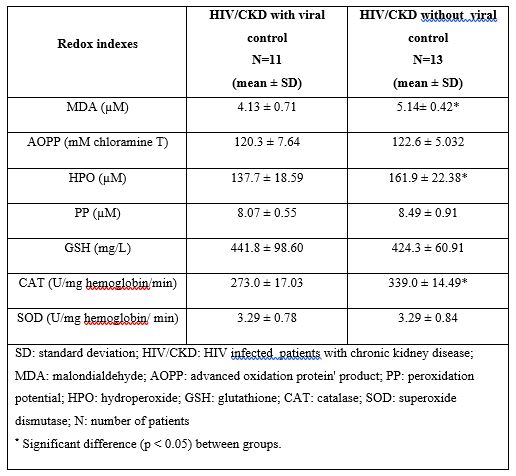
Redox indexes data of HIV/CKD patients’ divides in two groups to analyze the influence of viral replication control are shown in Table 5. HIV/CKD patients without viral replication control showed values of MDA, CAT and AOPP higher than the HIV/CKD patients with viral replication control.
Redox indexes data of patients before and after hemodialysis are shown in Table 6. GSH Significantly lower values (p < 0>
| Redox indexes | nHIV /CKD | HIV/CKD | ||
Extraction 1 (mean ± SD) | Extraction 2 (mean ± SD)/% | Extraction 1 (mean ± SD) | Extraction 2 (mean ± SD) /% | |
| MDA (µM) | 3.75 ± 0.20 | 7.41 ± 1.62a /100%* | 4.63 ± 0.57 | 7.07 ± 1.67a /92%* |
| AOPP (mM Chloramine T) | 116.4 ± 5.77 | 127.5 ± 5.48a /75%* | 121.5 ± 6.31 | 130.1 ± 7.06ab /67* |
| HPO (µM) | 122.9 ± 17.20 | 139.7 ± 19.36 | 150.8 ± 23.68 | 145.5 ± 17.40 |
| PP (µM) | 8.31 ± 1.19 | 11.91 ± 1.05a /100%* | 8.3 ± 0.78 | 12.97 ± 1.25ab /100%* |
| GSH (mg/L) | 592.7 ± 95.51 | 383.2 ± 62.68a /100%* | 432.3 ± 79.00 | 329.7 ± 49.45ab /79%* |
| CAT (U/mg hemoglobin/ min) | 235.7 ± 20.70 | 262.5 ± 84.47 | 306.0 ± 34.55 | 246.3 ± 73.47 |
| SOD (U/mg hemoglobin/min) | 3.62 ± 1.08 | 4.79 ± 1.08 | 4.00 ± 1.37 | 5.27 ± 1.75a /25%* |
SD: standard deviation; nHIV/CKD: non-HIV infected patients with chronic kidney disease; HIV/CKD: HIV infected patients with chronic kidney disease; MDA: malondialdehyde; AOPP: advanced oxidation protein' product; PP: peroxidation potential; HPO: hydroperoxide; GSH: glutathione; CAT: catalase; SOD: superoxide dismutase; Extraction 1: before hemodialysis; Extraction 2: after hemodialysis. a Significant differences (p < 0> b Significant differences (p < 0> * % of patients with significant differences (p < 0> | ||||
Table 6: Redox indexes data of the different groups before and after hemodialysis.
Redox indexes data of HIV/CKD patients’ after HD was divides in two groups to analyze the influence of viral replication control. But no significant differences (p > 0.05) were found (not presented data).
Correlation analysis between redox and other index values was done without any significant relation among the studied parameters (p > 0.05).
In recent years, a relevant decline in morbidity and mortality of HIV infection has been observed due to ART_ENREF_11. ART can also successfully prevent AIDS-related morbidity and mortality, resulting in an increased lifespan of HIV-infected patients. In turn, the course of HIV disease has evolved from a universally fatal infection to a manageable chronic illness _ENREF_15(De Clercq, 2009). Survival of these patients with CKD receiving HD has also progressively improved (Ahuja, Borucki, & Grady, 2000; Dandachi, Fabricius, Saad, Sawkin, & Malhotra, 2022; Mandayam & Ahuja, 2004).
However, it has become evident that patients taking effective ART remain at increased risk of non–AIDS-related morbidity and mortality. Some ARV classes are associated with lactic acidosis, hyperlipidemia, glucose intolerance, diabetes mellitus, fat redistribution, wasting, and atherosclerosis. These conditions include the premature onset of cardiovascular disease, neurocognitive disease, bone disease, cancer, and renal disease (Otto & Pecora Fulco, 2021; Sánchez & Gutierrez, 2008). These observations could be related to augmented OS associated with ARV toxicity previously reported and that suggests mitochondria as a toxic target (Lewis, 2003).
OS could be affecting both viral replication and cell apoptosis during HIV infection (Anthony & Ashok, 2011; Cacciapuoti, 2016; Palipoch & Koomhin, 2015). It has been previously reported that HIV-infected individuals have significantly lower antioxidant concentrations than non-HIV subjects (Coaccioli et al., 2010; González et al., 2014). A similar switch was observed in patients with ARV treatment and diverse clinical conditions (Gil, Gravier, & Pérez, 2013). The results of HIV patients' redox status in the present study agreed with those reported by previous studies with a patient taking ART in adequate viral control. Abnormal high concentrations of pro-oxidant species resulting from sustained immune system activation by HIV infection could reduce the antioxidants defense system and the cumulative damage of cellular components generating increased lipid peroxidation products and oxidized proteins(Al-Dalaen & Al-Qtaitat, 2014; Sies, 2015). The clinical development of HIV infection is influenced by diverse molecular mechanisms on increased oxidative metabolism appending risk of molecular deterioration and improving diverse virus replication, or/and contributing to poly pathology condition (Anthony & Ashok, 2011; Coaccioli et al., 2010). These observations could be explained in part by different contributing factors, such as low intake of antioxidants or their precursors, and malabsorption events accompanying HIV clinical evolution. Furthermore, ARV therapy has an additional incidence on pre-existing OS related to HIV status (Ikekpeazu, Orji, Uchendu, & Ezeanyika, 2020).
Diverse experimental studies have demonstrated that oxidative imbalance is also a hallmark in renal diseases, representing a fundamental process in the development and complications of CKD (Pellegrino, La Russa, & Marrone, 2019; Scholze, Jankowski, Pedraza-Chaverri, & Evenepoel, 2016; Small, Coombes, Bennett, Johnson, & Gobe, 2012). It appears that ROS increase in a graded manner as renal function deteriorates, as different studies have reported inverse correlations between different markers of OS and glomerular filtration rate (Dounousi, Papavasiliou, & Makedou, 2006; Terawaki, Yoshimura, & Hasegawa, 2004). OS has a vital role in the pathophysiology of different kidney diseases, and several complications of these diseases are mediated by OS or by OS-related metabolites or inflammation (Ozbek, 2012). That is why one element for OS occurrence in patients with renal disease is the underlying complication itself.
Persistent systemic inflammation has been associated with HIV disease progression. ART suppresses viral load during long-term effective treatment corroborated by physician follow-up using different biomarkers. But HIV-infected individuals treated have persistent low grade inflammation and immune activation that have been associated with various factors such as OS (Erlandson & Campbell, 2015). Afterward an increase in viral load could raise inflammation and immune reactivation that are connected to augmented ROS generation with clinical decline of kidney function (Longenecker et al., 2009). All patients without viral control in the study were treated with rescue-regimen and presented long time living with HIV. In that sense physician-oriented treatment change evaluation.
In the present study, a reduction in viral load after dialysis could have been due to adsorption of the virus to the dialysis membrane, as have been reported by other authors (Ahuja & Agraharkar, 2000).
Even when it has been reported that HD leads to depletion of urea, creatinine, and uric acid (Mozdalifa & Idres, 2016; Nisha, Srinivasa Kannan, Thanga Mariappan, & Jagatha, 2017) as in the present study, a graded increase in OS has also been reported and with increasingly longer durations of HD. Thus, this suggests that OS could accelerate renal injury progression by inducing cytotoxicity (Cachofeiro et al., 2008). Replacement procedures such as HD can induce OS because of massive repeated contact of blood with dialysis membranes that triggers defense mechanisms in the red cells to protect against oxidative damage, together with a chronic deficit in antioxidant defense system whose consequences are also of secondary antioxidants loss during HD process (Liakopoulos et al., 2017).
HD is associated with OS, which is involved in the pathogenesis of kidney failure events, systemic complications, and subsequently cardiovascular diseases (Coombes & Fassett, 2012; Gosmanova & Le, 2011). Previous report showed MDA and ROS increased values in inflammatory kidney diseases, including CKD. Moreover, dialysis treatment per se exaggerates OS (Liakopoulos et al., 2017). The identified modifications include the concentration of lipid peroxidation products, like MDA, which was superior in uremic patients compared to healthy people (Himmelfarb, 2008). Similar results were obtained in the present study with the biomarkers of oxidative damage (MDA and AOPP).
It has been demonstrated that the presence of OS may conduce to substantial molecular modifications in the kidney, similar to those seen in CKD. Oxidizing metabolites contribute to progressive kidney failure by promoting renal ischemia, inciting glomerular injury, cell death, and apoptosis, and finally, by stimulating a severe inflammatory process (Modaresi, Nafar, & Sahraei, 2015). Several results suggest that HD is distinguished by excessive OS state, which results from loss of antioxidants throughout dialysis procedures and accumulation of oxidative products. OS is also triggered by iron infusion, anemia, central venous catheter, bio-incompatible dialyzers, and endotoxin challenge (Liakopoulos et al., 2017; Shouman et al., 2019). Throughout HD, blood exposure to dialyzer membranes and dialysate provoke activation of complement factors, platelets, and polymorphonuclear cells, and subsequently ROS production, within minutes after initiation of HD sessions (Granata, Zaza, & Simone, 2009; Liakopoulos et al., 2017). It has also been reported an increased level of lipid peroxidation parameters during years of HD patient's follow-up (Sioud, Ati, Bouzidi, Kerkeni, & Hammami, 2019). To explain these findings, it has been prompted that impairment of the mitochondrial respiratory system, which is pronounced in CKD patients, and more spoiled in HD patients, could be one of the causes of ROS generation (Granata et al., 2009; Liakopoulos et al., 2017). The patients included in our study showed both an increased oxidative damage and a lower antioxidant capacity after HD.
In conclusion, the present study contributes to the evidence that HIV is related to the increased OS in CKD and non-CKD patients. Metabolic imbalance, such as altered redox parameters showed in previous and present articles, could be an important part of complications in HIV infection and comorbidities. On the other hand non-viral control could influence on oxidative status in HIV/CKD patients, that is why ART affectivities should be monitored using HIV progression markers. Therefore, the OS evaluation will be a potentially useful strategy to characterize infection conditions, both effects of the antiviral combinations and hemodialysis, and alternative therapies for ameliorating the oxidative impact.
Redox imbalance could play a causal role in the progression of these pathologies by promoting damage to cell structure and functions. Redox status diagnosis should be included in follow-up and treatment effect evaluation of HIV hemodialysis patients.
The study and enhancement of surrogate markers of HIV disease progression, including OS indexes, continues to be an outstanding research topic related to emerging therapies that claim to modify the process of immunological decline. Moreover, antioxidant treatment has contributed to suppressing some of the pro-oxidant effects of ART and HD (Coombes & Fassett, 2012; Elkhair Ali et al., 2020). Antioxidants supplementation in combination with both therapies may have a beneficial impact on these patients.
The authors thank healthy volunteers and patients with HIV infection who participated in the study.
This research was funded by Project MINSAP 151068 (Cuba) and Project FONDECYT 1130601 (Chile).
The authors declare that they have no conflicts of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
