
case report | DOI: https://doi.org/10.31579/2639-4162/069
1Assistant professor, Obstetrics and Gynecology Department, Lebanese University, Beirut, Lebanon
2Obstetrics and Gynecology Department, Al Zahraa Hospital University Medical Center, Beirut, Lebanon.
3Medical Director, Heah of Obstetric and Gynecology Department, Director IVF center Abou Jaoude Hospital, Jal el Dib, Lebanon
4Medical Doctor, Radiology Department, Abou Jaoude Hospital, Jal el Dib, Lebanon
5Pathologist, Pathology Department, Al Zahraa Hospital University Medical Center, Beirut, Lebanon.
6Assistant professor of Radiology Colombia University, USA, Dianostic Radiology, Nuclear Medicine
7Obstetrics and Gynecology Department, Lebanese University, Beirut, Lebano
*Corresponding Author: Kariman Ghazal, MD Assistant professor, Obstetrics and Gynaecology Department Lebanese University.
Citation: Kariman Ghazal, Imad Abou Jawde, Sandra Hasbani, Marwan Saliba, Sami Faddoul and Fatima Hamiye (2022). Backward Falling Elderly. J. General Medicine and Clinical Practice. 5(3); DOI:10.31579/2639-4162/069
Copyright: © 2022 Kariman Ghazal, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 27 June 2022 | Accepted: 05 July 2022 | Published: 13 July 2022
Keywords: leiomyoma; misdiagnosed; sarcoidosis; torsion; ovarian fibroma
Preoperatively, torsion of ovarian fibroma is frequently misdiagnosed as an uterine leiomyo-ma. A 58-year-old lady who complained of nausea and stomach pain was proviso diagnosed with uterine leiomyoma. Right solid mass with maintained blood flow was visible on trans-vaginal ultrasonography and Doppler. A well-defined solid mass measuring 15 cm by 10 cm and most likely a subserous uterine leiomyoma with central necrosis and more positive lymph nodes were detected by magnetic resonance imaging on the right side of the pelvis. RMI re-sults were confirmed by PET scan, and the sarcoidosis pattern was confirmed by biopsy. The right ovary was the source of the solid mass at laparotomy, which had torsion evidence. Mi-croscopic analysis of the mass supported the diagnosis of ovarian fibroma with necrosis. The preoperative misdiagnosis of ovarian fibromas and the sarcoidosis diagnosis are both repre-sented in this article.
However, extra uterine masses provide a more difficult diagnostic problem. Pedunculated/Intra ligamentous leiomyomas or ovarian masses are two differential diagnoses for solid abdominopelvic extra uterine masses. Although imaging tools aid in the diagnosis, histology is crucial in excluding other possible diagnoses.[1]
Ovarian fibromas are the most frequent benign solid cancers of the ovary, accounting for 1-4 percent of all cases. They are typically found in middle-aged women [1], are frequently challenging to identify preoperatively, are commonly mistaken for uterine fibromas due to similar pathology, complications, clinical, and ultrasonic characteristics [2, 3], and are occasionally misdiagnosed as malignant carcinoma due to ascites and elevated serum CA-125 levels [5, 6].
In this case study, a 58-year-old postmenopausal woman with acute pelvic pain was clinically suspected to have a uterine fibroma pedunculated due to rapid growth of the mass in one year after cancer evaluation and imaging was diagnosed as a uterine fibroma with necrosis centrally and with RMI and PET scan released evident lymph nodes and
biopsied confirmed diagnosis of sarcoidosis. The patient's final diagnosis was an ovarian fibroma with necrosis central and torsion and she didn't know she had sarcoidosis.
To evaluate whether abdominal and pelvic tumors in postmenopausal females are benign or malignant, a strong index of suspicion is required.
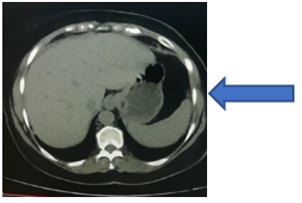
Yes; but It is preferable to add the difference between the sexes in the previous literature, especially that the two cases in the study are female. A 58-year-old post-menopausal multiparous woman in G5 P5 gravida 5 para 5 ( 5 pregnancy and 5 delivery) reported to the emergency room complaining of nausea, vomiting, and a 6-day history of severe abdominal pain that first appeared in the right lower quadrant before spreading to the entire abdomen. She had previously experienced sporadic episodes of stomach pain, dysuria, pollakiuria, and a feeling of abdominal heaviness in the months before. All of her vital indicators were within the usual range. She took intravenous analgesic as a pain reliever after receiving a tentative diagnosis of uterine fibroma from a CT scan. (Figure 1)
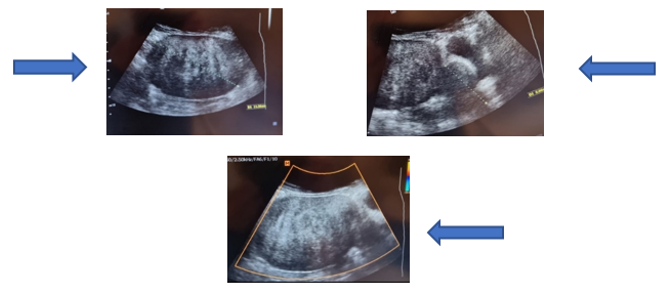
For inquiry and follow-up, the patient came back to the clinic. In the right iliac fossa and hypogastrium, a palpable, firm mass the size of a 16-week uterus was seen during a physical examination. Its bottom limit could not be attained, and it lacked a tender and clearly defined limit. A vaginal examination indicated an expanding uterus and a 15 cm-long, uncomfortable, irregular lump that was firm in consistency. The mass was not affected by cervical movements, according to pelvic ultrasonography, which revealed a non-homogeneous mass (15 cm 10 cm) in the upper and right lateral uterine (Figure 2), endometrium thickness of 4 mm. The same mass was also located directly anterior to the uterus and continuous with it (Figure 3). Doppler control is negative in the mass. (Figure 4).
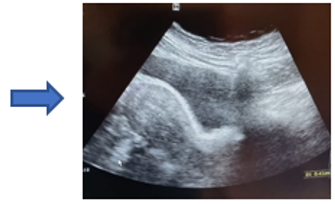
Recent abdominal and pelvic ultrasounds do not show any pelvic mass based on the history. (Figure 5)
Biochemical and hematologic tests that were routinely conducted were normal. Every tumor marker was also within normal limits. A well-defined lobulated mass lesion (15cm .10 cm.9.3 cm) located anterior to the uterus and superior to the bladder was discovered by MRI. It looked to shift the uterus posteriorly, extended up to the anterior abdominal wall anteriorly, and compressed the bladder dome inferiorly. Superiorly, it extended up to level L5-S1. On T2, it showed a heterogeneous signal strength that was more intense than the myometrium and iliopsoas (Figure 6), and on T1 had isointense myometrium and hyperintense iliopsoas (Figure 7)
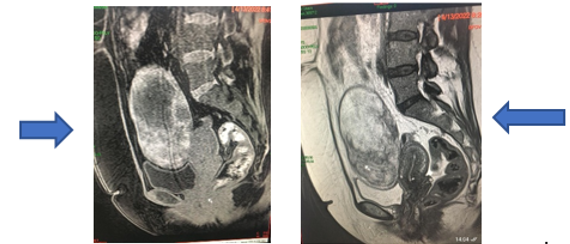
According to imaging, it was determined that it was a right pedunculated fibroid with necrosis in the center and more obvious lymph nodes, which advised Pet scans with biopsy to confirm the diagnosis of sarcoidosis.
The research subject gave written approval for a laparotomy and the preoperative tests conducted by hospital protocol were normal for the full blood count hemoglobin. Laparotomy was performed, and the solid mass, which was torsioned and measured 15 cm by 10 cm, was discovered to be coming from the right ovary irregularly surfaced, black, the blue-encapsulated mass that is twisted three times is linked to the right ovary (Figure 8, Figure 9) via a twisted pedicle.
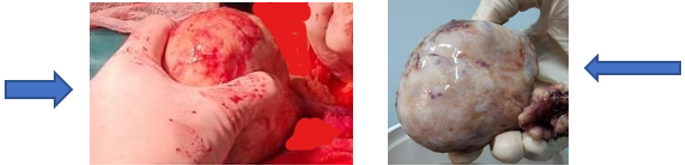
The left adnexa and uterus both seemed healthy. Both a bilateral salpingo-oophorectomy and a complete hysterectomy were carried out. The diagnosis of ovarian fibroma with widespread ischemia necrosis was established based on pathological and immunohistochemical results For follow-up appointments for the sarcoidosis every three months, the patient was released on the third postoperative day
Ovarian mesenchymal neoplasms are rare, non-specific, and pose challenging issues for diagnosis, histogenesis, behaviour, and therapy [5]. Between the ages of 20 and 65, ovarian fibromas are diagnosed, with mean ages falling between the fifth and sixth decade [6-8]. In 4–8% of patients, ovarian fibromas can be bilateral, and in 10% of instances, they can be numerous [5], notably in Gorlin syndrome [9, 10], or they can be accompanied by pleural effusion and ascites in Meigs syndrome [11]. It is infrequently linked to hirsutism or infertility [13] and frequently observed concurrently with uterine leiomyoma, suggesting a similar hormonal stimulation. Despite their size, these tumours are frequently asymptomatic and are typically found during routine examinations [1]. They can occasionally present as abdominal enlargement, urinary symptoms, or abdominal pain [5], and on occasion in our instance [14, 15] with torsion, which is uncommon in postmenopausal patients.
Because of its solid form, relationship with ascites and pleural effusions [16], as well as its high CA-125 levels [8], which are particularly prominent in torsion due to necrosis and inflammation [4], ovarian fibroma can also mimic ovarian cancer. Typically, ultrasound features lack specificity [16]. When ovarian torsion is suspected, doppler imaging is the preferred examination. Due to bleeding, oedema, coexisting bulk, free pelvic fluid, a lack of arterial or venous flow, and a twisted vascular pedicle [14], the ovary typically appears swollen, amorphous, hypoechoic, and heterogeneous. Ovarian fibromas typically show up on a CT scan as uniform tumors with delayed enhancement [8, 17]. A midline adnexal mass that is rotated toward the pelvic side opposite to that of the patient's torsion is among the diagnostic indicators Ascites and uterine deviation to the afflicted ovary's side [14]. Ovarian fibromas must frequently be further characterized with MRI in order to be distinguished from other solid ovarian tumors [16]..
Due to the leiomyoma's degeneration, which included bleeding, necrosis, cyst formation, calcareous and sarcomatous degeneration [2, 5], the tumour showed up on T1 as a well-circumscribed low signal intensity mass with mixed signal intensity on T2. In fact, solid mass, size greater than 10 cm, internal hypervascularity, advanced age, spread of the tumour into the pelvis or adjacent viscera, and metastases are all indicative markers of malignancy [13]. While, tube thickening, ascites, diversion to the twisted side, bleeding in the thickened tube, and torsion knot are suggestive indications of torsion. [17].
Due to its rarity, and in our case, we assume that the torsion of the ovarian fibroma was a false-positive diagnostic of uterine fibroma with necrosis and hazy somatotypes In actuality, surgical removal is required for ovarian fibroma treatment. Preoperatively, uterine leiomyoma is frequently mistaken for ovarian fibroma. According to Leung et al, The diagnosis of an ovarian fibroma or a solid ovarian tumor was correctly made preoperatively in only 5 patients (21.7%) [18] In a retrospective comparative analysis of 97 patients with ovarian fibroma/fibrothecoma Yeon Jean Cho et al, found that 42.2% of cases were misdiagnosed as uterine myomas and 6.2% were misdiagnosed as malignant ovarian tumors [19]. Other retrospective analysis of 47 women with ovarian fibromas, Son et al. reported five occurrences of laparoscopic ovarian cystectomy. [7] 15 ovarian fibromas were treated in a series of cases by ovariectomies (five cases), adnexal resections (three cases), and total hysterectomies with salpingo, according to Târcoveanu et al (five cases). [13] High-resolution ultrasonography and color Doppler in 10 of the cases in the Târcoveanu et al. investigation pointed to the presence of an ovarian fibroma whereas computed tomography (CT) and magnetic resonance imaging (MRI) were only suggestive for the diagnosis of ovarian fibroma in three cases. [13] When the transvaginal ultrasound revealed the solid nature of the left adnexal mass, the investigated case was re - evaluated by MRI and given a preliminary diagnosis of leiomyoma.
A well-defined solid hypointense mass, most likely a subserous anterior wall uterine leiomyoma, was visible on MRI in the right side of the pelvis. The solid ovarian mass, approximately 15 cm by 10cm, was discovered during an exploratory laparotomy and was coming from the right ovary. A mass in the right ovary with ovary was removed. The removed mass's postoperative histologic analysis supported the ovarian fibroma diagnosis. According to Najmi et al, young women with ovarian fibromas should consider cystectomy while perimenopausal or postmenopausal women should consider salpingo-oophorectomy. [1] The right ovarian tumour was removed from the investigated case along with a total abdominal hysterectomy and a left annessiectmy. In the blood sample collected before to surgery for cross-matching, the ovarian reserve indicators were normal. The patient was sent home with instructions to monitor sarcoidosis. The preoperative misinterpretation of ovarian fibroma with uterine leiomyoma with torsion and the diagnosis of sarcoidosis are highlighted in this study.
The most frequent benign solid tumor of the ovary, ovarian fibromas are rare. Despite its rarity, it ought to be taken into account in the differential diagnosis before surgery. Ovarian fibromas are frequently misdiagnosed as uterine leiomyomas and occasionally as malignant ovarian tumors. In perimenopausal or postmenopausal women, the usual treatment option for ovarian fibromas is salpingo-oophorectomy, which entails surgical removal along with immunohistochemistry testing for a certain diagnosis.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
