
Case Report | DOI: https://doi.org/10.31579/2641-0419/122
*Corresponding Author: Sandeep M Patel, Director, Structural Heart and Intervention Center St. Rita's Medical Center (Mercy) 730 West Market Street, 2K Tower Lima, Ohio 45801
Citation: Siddharth Agarwal, Christopher Sosnofsky, Jamie Saum RN, Brian Taylor, Sandeep M. Patel (2021) Out of the Blue Acute May-Thurner Syndrome. J. Clinical Cardiology and Cardiovascular Interventions, 4(1); Doi:10.31579/2641-0419/122
Copyright: © 2021 Ali Alkhayru, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 21 December 2020 | Accepted: 30 December 2020 | Published: 08 January 2021
Keywords: may-thurner syndrome; phlegmasia cerulea dolens; DVT; IVUS; vertebral manipulation
May-Thurner syndrome (MTS) is defined as extrinsic ilio-femoral venous compression by the aorto-iliac arterial system against vertebral bodies and has been associated with many abnormalities involving the arterial system as well as bony structures around the ilio-caval region. We present an unusual case of a patient who came with phlegmasia cerulea dolens in the setting of acute onset MTS after chiropractic vertebral manipulation and was treated with a multimodal interventional approach, combining pharmaco-mechanical catheter directed thrombectomy along with venoplasty with stenting and subsequent post-procedure anticoagulation and antiplatelet prophylaxis.
Classic May-Thurner syndrome (MTS) involves the compression of the left common iliac vein between the right common iliac artery and the fifth lumbar vertebrae. MTS can be asymptomatic or can present with symptoms related to acute deep vein thrombosis (DVT) or chronic lower extremity venous hypertension. MTS is typically considered in young patients who present with unilateral left lower extremity swelling, symptoms in spite of adequate treatment of DVT, or recurrent, ipsilateral proximal DVT without any predisposing risk factors. Within this report, we detail an unusual case of acute onset May-Thurner syndrome due to spinal manipulation.
Case Presentation
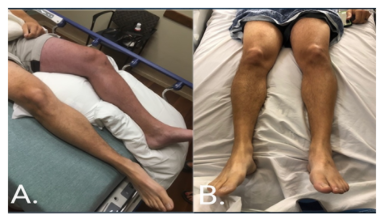
A 43-year-old male presented to the emergency department with sudden onset swelling and severe pain in the left lower extremity (LLE) after several spinal manipulations by his chiropractor a few hours prior, for chronic lower back pain, which has been present for the last couple of months. He reports receiving several high frequency thrusts to the lower back located at the level of lumbar vertebrae and the lumbosacral junction. He states that his back pain improved after manipulation but within half an hour of leaving the chiropractor’s office, he noticed that his left leg started to swell. The swelling involved the entire leg and he also complained of severe pain in the LLE even while at rest. On presentation in the emergency department, physical examination showed 4+ pitting edema along with bluish-discoloration and exquisite tenderness of the entire LLE (Figure 1-A).
Range of motion was preserved in all extremities and all pulses in the LLE were palpable. There were no skin changes suggestive of chronic arterial or venous disease.
Past medical history was unremarkable. The patient had no prior history of DVT, malignancy, or hypercoagulable disorder and was not on any medications at the time of presentation.
The patient was afebrile with stable vital signs. Initial investigations were unremarkable except for creatine kinase levels (872 U/L) (suggestive of muscle ischemia) and elevated D-dimer (820 ng/ml). Doppler ultrasound of the left lower extremity showed extensive proximal DVT extending from left popliteal vein, the left common femoral vein upto the point where it could be visualized, along with superficial venous thrombosis within the great saphenous vein. With the patient’s clinical history that was provided, abnormal physical examination, along with the LLE doppler results, the findings were suggestive of phlegmasia cerulea dolens (Painful Blue Inflammation). In view of an acute onset left-lower extremity DVT, complicated by phlegmasia cerulea dolens and despite absence of any risk factors, contrast CT of abdomen and pelvis was performed to rule out any mechanical abnormality, which revealed the right common iliac artery was compressing the left common iliac vein against the lumbar vertebrae (Figure 2).

The patient was started on IV heparin and morphine. Interventional cardiology was consulted for possible intervention. Based on the anatomy detailed from the CT scan and the emergent need to restore the blood flow in the setting of PCD, a decision was made to perform pharmaco-mechanical thrombectomy using AngioJet rheolytic thrombectomy system (Boston Scientific, Marlborough, MA, USA) followed by IVUS to determine the need for subsequent venoplasty +/- stenting.
The left popliteal vein was accessed, and digital subtraction venography was performed which showed occlusion of the left popliteal, femoral, external iliac, and common iliac vein up to the bifurcation at the inferior vena cava, without any presence of collaterals (Figure 3-A).
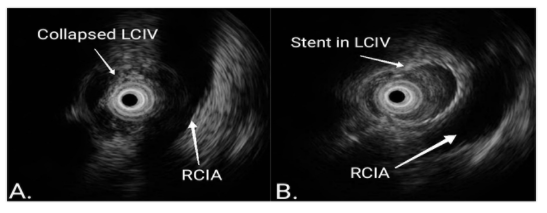
Given the findings on presentation, intervention using Zelante AngioJet catheter was performed to remove the acute clot. Two runs using the catheter were performed from the popliteal vein to the IVC. After which, a pulse spray of tPA with 30-minute dwell time was performed. Repeat venography showed clearance of the thrombus from the popliteal vein to the common femoral vein, however, there remained an approximately 95% stenosis of the left common iliac vein. Decision was made to perform IVUS to understand the anatomy, size of the vessel as well as choose appropriate treatment plan to maintain patency. IVUS demonstrated near-complete obliteration of the venous lumen compressed between the right common iliac artery and the vertebral body (Figure 4-A). Therefore, balloon venoplasty with a 16 mm x 40 mm ATLAS balloon (Bard peripheral vascular, Tempe, AZ) was attempted (Figure-3B). Venoplasty of the entire left common iliac, external iliac as well as common femoral vein was performed and subsequently a 18 x 90 mm Wahlstent (Boston Scientific, Natic, MA) was inserted from above the confluence of left and right common iliac veins into the IVC to left external iliac vein. Another 18 x 90 mm stent was deployed in an overlapping fashion with the first stent and finally the third stent of 16 x 60 mm was deployed in an overlapping fashion with the second one, proximal to the origin of the profunda femoris vein. The entire lengths of the stents were post-dilated and IVUS was again performed which demonstrated appropriately sized, well-apposed stents (Figure 4-B). Final venography was done which illustrated excellent flow from the below the popliteal vein to common femoral vein, and subsequently from the iliac vein into the IVC (Figure 3-C).

Within a couple of hours, the swelling and pain started to resolve. The patient became completely asymptomatic within 24 hours post-procedure (Figure 1-B). The patient was discharged on the second day post-procedure on aspirin, clopidogrel and apixaban for three months followed by discontinuation of clopidogrel. On follow up visit after two months the patient was completely asymptomatic and venous ultrasonography was unremarkable.
Discussion
May Thurner Syndrome (MTS) is reported in only 2-5 percent of patients who present with symptomatic lower extremity venous disorder and hence it requires a high index of clinical suspicion [1].
The definition of MTS involves extravascular compression of the venous outflow tract between the arterial system and other nearby structures in the ilio-caval region, this allows for a broad range of etiologies ranging from congenital predisposition to localized aneurysms of the arterial system, lumbar spondylosis, osteophytes of the lumbar vertebrae, endometriosis and prostatic enlargement all have been reported in various case reports [2]. In our case, due to the acute onset of left lower extremity swelling and bluish-discoloration on presentation along with a temporal relationship with spinal manipulation, in the absence of any pre-existing risk factors for development of iliofemoral thrombosis, we hypothesize that the spinal manipulation caused a shift of the vertebral body which resulted in a “sandwiched” left common iliac vein between the right common iliac artery and the vertebrae. Although cervical manipulation has been associated with the development of internal jugular vein thrombosis [3], this is the first case report connecting spinal manipulation to iliofemoral DVT that we are aware of. Rarely, as in our case, PCD develops. PCD is a late manifestation of non-collateralized venous obstruction, which prevents adequate antegrade arterial flow, therefore causing massive fluid sequestration, increased compartment pressures and ultimately leading to arterial ischemia that progresses rapidly to gangrene and limb loss within hours [4]. As in our case, it presents with severe pain, swelling and cyanosis and can be preceded by an early stage of phlegmasia Alba dolens i.e. painful white inflammation. When identified, PCD is a harbinger for proceeding with timely intervention.
Initial diagnostic testing includes doppler venous ultrasonography which can detect the presence of DVT but cannot precisely locate the area of compression. Supplementary noninvasive testing includes helical abdominal CT, CT venography, or MR venography which can precisely indicate the location and cause of iliac vein compression and other anatomic considerations which might be imperative for choosing appropriate treatment modality [5]. Definitive diagnosis can only be made through conventional venography along with the use of intravascular ultrasonography (IVUS) which can be very useful for determining the vessel diameter, aiding stent sizing, placement, and ensuring full stent expansion.
The basic strategy for the treatment of MTS includes clearing of the thrombus to restore blood flow and addressing the venous compression to ensure prolonged venous patency. Endovascular treatment including thrombectomy followed by venoplasty and stenting provides immediate relief of symptoms with long term patency rates and decreased incidence of post-thrombotic syndrome as compared to conservative anticoagulant therapy [6]. As in our case the patient had clinical as well as diagnostic evidence of PCD and henceforth required emergent thrombectomy [7]. Although IV thrombolytic infusions have been used, pharmaco-mechanical thrombectomy (PMT) is a contemporary approach that allows for on-the-table immediate results with reduced risk of bleeding associated with thrombolysis. According to the CaVenT study, ilio-femoral DVT was successfully treated with catheter directed thrombolysis correlated with increased clinical benefit for up to five years [8]. The technical success of the endovascular approach is upward of 96% with a 1-year primary and secondary patency rate of 58%-100% and 76%-98% [6]. Subsequently, expert consensus recommends 3-6 months of post-procedure anticoagulation as well as antiplatelet therapy, as in our patient who was started on aspirin, clopidogrel and apixaban to maintain venous patency as well as prevent in-stent restenosis [9].
Conclusion
Our case presents an unusual association of acute onset May Thurner syndrome (MTS) by spinal manipulation in a patient presenting with signs of PCD. Emergent interventional treatment, preferably with PMT can be performed, to prevent progressive limb injury or loss. The diagnosis of MTS requires a high index of clinical suspicion and needs to be kept in mind when evaluating lower extremity pathologies, even in the acute setting to ensure appropriate endovascular treatment.
Conflicts of Interests: None
Disclosure: None
Consent: written consent has been taken from the patient regarding the publication of case details as well as the images.
Funding: None
Acknowledgement: None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
