
Research Article | DOI: https://doi.org/10.31579/JHV-2021/012
*Corresponding Author: Mohammad Alsalaldeh, Assistant Professor Doctor, Pamukkale University, Faculty of Medicine Hospital, Cardiovascular Surgery Department. Denizli / TURKEY
Citation: Alsalaldeh M. A. D. Kaya (2021) Our Center Experience with Modified Eversion and Conventional Carotid Endarterectomy J, Heart and Vasculature 1(3); DOI: 10.31579/JHV-2021/012
Copyright: © 2021, Mohammad Alsalaldeh, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 05 April 2021 | Accepted: 15 April 2021 | Published: 11 May 2021
Keywords: modified version carotid endarterectomy, conventional carotid endarterectomy, carotid artery stenosis, revision, postop stroke
Objective: Carotid artery stenosis is considered to be the cause of 10-20% of all strokes and ischemic attacks. Conventional carotid endarterectomy (CCEA) and modified eversion carotid endarterectomy (MECEA) are the most performed surgical procedures nowadays. We compared the results of both surgical techniques to shed light on the advantages and disadvantages of each one.
Materials and Methods: From January 2018 to October 2019 all carotid endarterectomy surgeries were collected and analyzed. 61 patients had been included in this study. 46 patients were operated on with MECEA and 15 patients with CCEA. Age, sex, the side of the operated carotid artery, revision, restenosis, mortality, and comorbidity were checked up.
Results: MECEA had shown superiority to CCEA in post-op stroke possibility while CCEA was superior in postop revisions due to hematoma and bleeding. Operated isolated left carotid arteries were not found in any revision procedure while right and bilateral arteries were equal in revision need. hospitalization stayment time MECEA was found shorter than in CCEA. During analyzing the data we noticed that there are significant relations between age, Diabetes mellitus (DM), hypertension, and smoking when correlated with postop revision. We found, also a significant relationship between smoking, DM, and hypertension with renal disease.
Conclusions: MECEA can be considered the first surgical choice of carotid artery stenosis management. Attention should be taken in some cases where there are long, tough, and strongly adherent plaques that CCEA is still the first choice. We still need more studies with bigger populations to ensure our results.
Carotid artery stenosis is a vascular pathology, usually resulted from atherosclerosis [1] and considered as a major risk factor for ischemic stroke or transient ischemic attacks in about 10-20% of all cases [2]. The management of the stenotic carotid artery depends on the stenosis degree, stenotic lesion location and length, the nature of the plaque, and whether the patient is symptomatic or asymptomatic. Medical treatment, open surgery, and stenting are the possible treatment methods according to the patient's situation and guidelines.
Carotid endarterectomy is a surgical treatment method which should take place in symptomatic patients with stenotic lesions or asymptomatic patients with severe stenotic lesions and high risk of stroke if kept on medical treatment only. According to the CREST study, the restenosis and occlusion were infrequent and there was no significant difference between endarterectomy and stenting up to 2 years [3].
Endarterectomy surgery can be done with the conventional procedure or with classic eversion or modified eversion procedures [4]. Eversion endarterectomy was first described by De Bakey et al in 1959 [5]. This technique has the advantage of complete autogenous repair [6]. Modified endarterectomy had been described lately as an alternative surgical technique to classic eversion with the advantages of less clamping time, fewer neurological problems, and primary closure [7].
In this study, we have reported our experience in treating carotid artery stenosis by modified eversion and conventional endarterectomy.
This is a retrospective study, done in our center over about two years (from January 2018 till October 2019) and by one surgeon. Ethics Committee Approval had been taken on 07/08/2020 under the approval number (60116787-020/41155). 62 patients had been operated on for carotid artery stenosis. 46 (74%) patients were operated on by modified eversion endarterectomy (MECEA) technique while 15 (24.6%) patients were operated on by conventional endarterectomy (CCEA). 80.3 % (n=46) of all patients were male and 19.7% (n=12) were female. According to the side of the operated carotid artery, the left carotid artery number was 29 (47.5%), right was 21 (34.4%) while bilateral operated carotid artery cases were 11 (18.0%). The bilateral stenotic carotid arteries were operated on in different sessions.
All our patients were checked up for diabetes mellitus (DM), hypertension, cerebrovascular accident (CVA), coronary artery bypass grafting (CABG), chronic renal disease, chronic obstructive pulmonary disease (COPD), peripheral artery disease (PAD), smoking, mortality, hospitalization time, revision, and re-occlusion. The mean age of the patients was around 67 years. The youngest patient was 46 and the eldest one was 86 years old. The hospitalization period was calculated too and found to be between 2 and 16 days with a mean of 5.8 days. 13 (21.3%) patients stayed 3 days while 12 (19.9%) patients stayed 4 days, one (1.6%) patient stayed 2 days and one patient who had CABG in the same admission stayed 16 days at the hospital postoperatively. According to the data of comorbidities, we found that 37 (60.7%) of the patients were hypertensive, 27 (44.3%) were diabetic, 14 (23%) had coronary artery bypass grafting (CABG) operations and four of them had CABG at the same admission, 15 (24.6%) patients had a history of CVA, 8 of them had CVA within one month prior carotid endarterectomy, 2 patients had CVA postoperatively and the remain 5 patients had CVA long time ago. Patients with renal diseases were 13 (21.3%), COPD and asthmatic patients were 9 (14.8%) and those who had peripheral artery disease were 4 (6.6%) while 20 (23.8%) patients were found, smokers. There were 6 patients needed revision operations for bleeding and hematoma. All of them had been operated on with MECEA surgical technique. Three of the revision cases were operated for the right carotid and the remaining three for the bilateral carotid artery stenosis.
Surgical Procedure: All patients were operated on under general anesthesia. The head is tilted to the contralateral side, and a folded dressing roll or an intravenous fluid bag is put under their shoulders to elevate the side of the neck which will be operated on. After painting and toweling of the operation are completed incision is done in oblique shape along with the medial border of the sternocleidomastoid muscle of about 8-10 cm in length. Gentle dissection of the underlying tissues is done after opening the platysma muscle downward to the carotid artery. Attention is taken to avoid vagal nerve injury. Common carotid artery (CCA) and its both main branches; internal carotid artery (ICA) and external carotid artery (ECA) are mobilized from the surrounding tissues and hanged by Dacron tapes (figure 1). Superior thyroid artery is hanged up too by silk suture. Systemic heparinization is given with the dosage of (70 IU/kg) and an average of 5000 IU bolus I.V to maintain ACT around 200-250.

MECEA Surgical Procedure: After heparin has been administrated and vascular clamps applied over CCA, ECA, and ICA with tightening a silk suture over superior thyroid artery, longitudinal arteriotomy is done in the CCA priorly to the bifurcation and extended to the ECA. ICA endarterectomy was done with a modified eversion technique without division the artery from CCA (figure 2a). Primary closure is done side by
side with the de-airing of the three arteries from the air.
CCEA Surgical Procedure:
the first steps are done typically as in MECEA while the arteriotomy is done here starting from CCA priorly to the bifurcation and extended to ICA and the endarterectomy is done as usual. (figure 2b).

Statistical analysis: Statistically we analyzed all our data using IBM SPSS statistics version 21, independent variables were compared by independent samples the Levene's Test for Equality of Variances and t-test for Equality of Means. p<0>
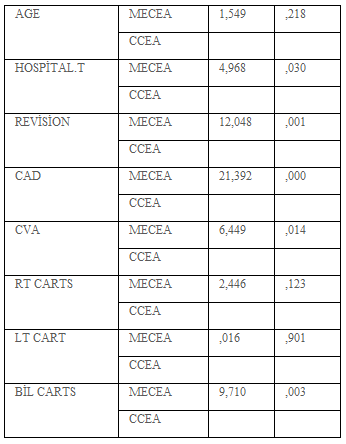
Over about two years we reported the results of our surgical procedures in managing carotid artery stenosis disease. We found significant differences when MECEA was compared to CCEA in hospitalization stayment time (p=0.03) and revision need (p=0.001) in favor of MECEA (Table 1)
Patients who developed post-op CVA (n=2) were both operated on for right carotid artery stenosis and with CCEA surgical procedure. When we compared the two surgical procedures for those two cases there was a significant difference in favor of the MECEA procedure (p=0.000).
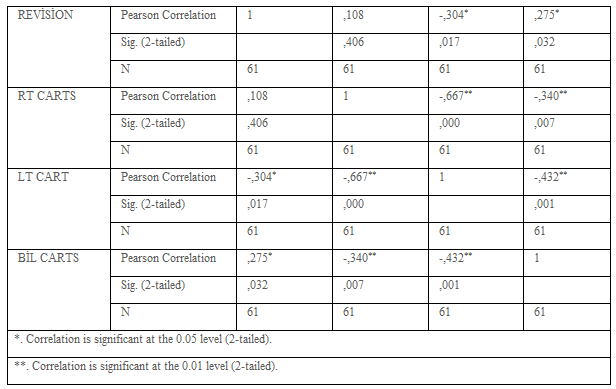
We noticed that there was no significant relationship between age and hospitalization stayment time while age has a significant correlation with the need for revision (p=0.021). Revision operations were found to have a significant difference when correlated with left carotid (p=0.017) and bilateral carotid artery stenosis (p=0.032) as well as it was significant in MECEA when the two surgical procedures were compared (p=0.001) (Table 2).
According to the data that we had obtained from our patients we found interesting correlations among patients comorbidities and habits, for example; there were significant correlations between renal disease with hypertension (p=0.008), DM (p=0.042), and smoking (p=0.000)
Carotid artery stenosis is one of the vascular pathologies which affect directly the central nervous system representing in stroke or transient cerebrovascular attacks. Surgical treatment according to the guidelines played a big role in managing carotid artery stenosis. The surgical procedures have been changed from time to time and nowadays the most acceptable types of such procedures are the eversion endarterectomy and for some surgeons the conventional ones. The stenotic lesion type, length, and localization are the main factors affecting the decision of the surgical procedure type.
In our study, we reported our experience in one center in managing carotid artery stenosis disease over the last two years. Our data of the patients were collected from computerized medical records. We used to perform modified eversion endarterectomy in most of our cases. On the other hand, conventional endarterectomy still has a place in our management. We tried to study those two procedures in the favor of the need for revision, the type of carotid artery, age, sex, and the other comorbidities associated with the carotid artery stenosis.
In 2016 Scott E. Musicant et al had done a similar study to analyze the clinical and financial outcomes of the modified eversion surgical technique in treating carotid artery stenosis. 197 patients were included in that study and (77.7%) of them were operated on with modified eversion endarterectomy while the others were operated on with conventional endarterectomy. The arteriotomy of modified eversions was done longitudinally and limited to the carotid bulb. All the operations were done by three surgeons. They had found that late stroke and death were higher in conventional endarterectomy while they were similar in the perioperative period. Also, the average time and cost of modified eversion operations were less than those in conventional ones [8]. In our study, all the operations were done by one surgeon. Our modified eversion endarterectomy was not limited to the carotid bulb but extended to the external carotid artery while in the conventional endarterectomy the arteriotomy was started from the common carotid artery and extended longitudinally upward the internal carotid artery. We preferred the conventional technique when the stenotic lesion is too long and it was seemed to be difficult to be managed by eversion. We had one case where we had started with the modified technique but because of the tough, long, and very conjoined lesion we had to convert our technique to a conventional one. None of our both techniques had significant restenosis over the short-mid term of the study. We had not included a financial review in our study but we found that the hospitalization stayment time was shorter when MECEA was performed.
In another study done by Khan, K. A et al where the two techniques were performed by four surgeons for forty patients. They had to use patch plasty in (2.5%) of the patients and selective shunt in 10% of the patients. 2 patients had to be reviewed in the operation room for hematoma [7].
We had used nor patch plasty neither selective shunt for any patient in both groups. We had a revision for 6 (9.8%) patients. All the revision cases had been operated with MECEA, 3 of them were done to the right carotid artery and the remaining 3 were done to both arteries (bilateral). Statistically, when we compared the two surgical procedures we found a significant difference in favor of the modified one (p=0.001).
In the 2020 year, another study was done by Davidovic L.B et al. They reviewed multi centers studies in modified Everson and conventional endarterectomy and the authors emphasized the efficacy, safety, and reduction of operative time of the modified eversion carotid endarterectomy, also they considered this procedure as the first choice in carotid surgery [9]. According to our study, we recognized that the modified eversion technique had a disadvantage in revision when compared to conventional surgery. We also noticed that the revision cases were limited in the right and bilateral carotid artery surgeries.
Postop CVA cases were operated by conventional technique. We had two patients developed CVA postoperatively and both of them were operated on for the right carotid artery stenosis. Statistically, there was a significant difference (p=0.000)
In this study, we evaluated the data of all patients not only according to their surgical procedures but also for their comorbidities too. We found that there are strong and significant relations between age, smoking, DM, and hypertension with postop revision due to hematoma and bleeding. Also, we found such a significant relationship between smoking, DM, and hypertension with renal disease.
According to our experience, MECEA can be considered as the first choice of the management of carotid artery stenosis with taking attention to its possibility of postop revision while CCEA has a higher risk for postop CVA. In long, tough, and strongly adherent plaques CCEA is still the first choice. The hospitalization stayment time in MECEA was found shorter than in CCEA. We still need more studies with a bigger population to ensure our results.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
