
Review Article | DOI: https://doi.org/10.31579/2694-0248/028
1 Orthopaedic Surgeon,Private Practitioner Mumbai, Maharashtra.
2 Department of Periodontology AND Oral Implantology M A Rangoonwala College of Dental Sciences and Research Centre, Pune.
3 Pedodontist and Preventive Dentist Private Practitioner.
4Assistant Professor dr Vasanat Rao Pawar Medical College, Nashik.
5Department of Periodontology and Oral Implantology M A Rangoonwala College of Dental Sciences and Research Centre, Pune.
*Corresponding Author: Sharayu Dhande, Department of Periodontology AND Oral Implantology M A Rangoonwala College of Dental Sciences and Research Centre, Pune.
Citation: Sagar Chaudhari, Sharayu Dhande, Sheetal Ajit Jangale, Ajit Govind Jangale (2022). Osteoporosis and Periodontitis: The Bi-Directional Link. J. Clinical Orthopedics and Trauma Care, 4(2); DOI:10.31579/2694-0248/028
Copyright: © 2022 Sharayu Dhande, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 10 January 2022 | Accepted: 20 January 2022 | Published: 17 February 2022
Keywords: osteoporosis; periodontitis; periodontal disease; tooth loss; fragility fractures; menopause; hormonal replacement therapy
Periodontitis is a multifactorial disease elicited by a complex of bacterial species, variety of risk factors, bacterial plaque, calculus that interact with host tissues causing the release of a broad array of inflammatory mediators, cytokines, chemokines some of which lead to destruction of the periodontal structures, leading to tooth mobility. Osteoporosis and Osteopenia are the conditions that represent the mineral content of the bone. In addition, aspects of bone composition and structure that may not be captured by bone mineral density measurements, such as bone size and geometry, and bone structure and material, contribute to increased bone fragility. Periodontitis as well as osteoporosis could also be risk factors for each other and have a impact that requires mutual concomitant management. An interventional approach is emerging with complex treatment options. Prevention and management of both of these diseases require interdisciplinary approaches and warrant future well-controlled longitudinal and interventional studies for evidence-based clinical guidelines.
Increasing life expectancy and popularity of dental implants, surgeons face a larger number of osteoporotic patients who require bone augmentation. [1] In addition, the combination of risk factors such as age, menopause, race, genetics, calcium intake, family history, medications and physical activity contribute to osteoporosis. [2-5]
Remodeling of bone in these units is important not only for maintaining bone mass, but also to repair microdamage, to prevent accumulation of too much old bone, and for mineral homeostasis. The activities of osteoblasts and osteoclasts are controlled by a variety of hormones and cytokines, as well as by mechanical loading. [6] Most importantly, sex hormones are very crucial for keeping bone mass in balance, and the lack of either estrogen or testosterone leads to decreased bone mass and increased risk for osteoporosis. The prevalence of osteoporotic fractures is increasing dramatically in the Western part of the world and is a major health problem in many countries. [7-8]
Periodontitis can be defined as the presence of gingival inflammation at sites where there has been a pathological detachment of collagen fibres from the cementum and the junctional epithelium has migrated apically. Inflammatory events associated with connective tissue attachment loss also lead to the resorption of coronal portions of tooth supporting alveolar bone. [9-10]
Osteoporosis, "too little bone in the bones," is a condition which mainly is seen in elderly women. The postmenopausal bone loss occurring in women can be an aggravating factor for osteoporosis. In cases of severe osteoporosis, the bone mass and structure of the skeleton are altered in such a way that the risk of fractures is very high. Since loss of alveolar bone is a notable feature of periodontal disease, severe osteoporosis could be suspected of being an aggravating factor in the case of periodontal disease. However, such a relationship is may easily be confounded by other factors such as gender, hormone intake, smoking, race, and age. [11-13]
The Global Burden of Disease Study conducted in 2016 reported that severe periodontal disease was the 11th most prevalent condition in the world. [14-15] Periodontitis and Osteoporosis both are diseases that are characterized by bone resorption. Osteoporosis involves systemic degenerative bone loss that leads to loss of skeletal cortico-cancellous microstructure and result in subsequent fracture, whereas periodontitis involves local inflammatory bone loss, following an infectious breach of the alveolar cortical bone, and it may result in tooth loss. Both diseases are defined by a preponderance of bone resorption, and their progression or severity is assessed systemically and/or locally. It is reasonable to argue that systematic skeletal change inevitably impacts the jaws and alveolar bone. [11-13]
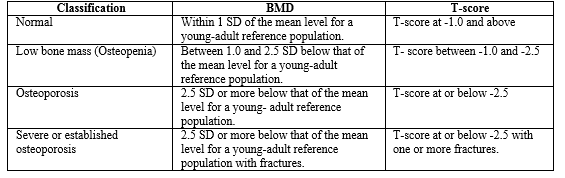
The techniques currently used to assess osteoporosis include dual-photon absorptiometry (DPA), dual-energy absorptiometry (DXA), and quantitative computerized tomography (QCT). According to World Health Organization (WHO) osteoporosis is considered to be present when the bone mineral density (BMD) is 2.5 standard deviations below the young normal. Osteopenia is defined as bone density levels 1 standard deviation and 2.5 standard deviations below normal.[16] Preferred locations for diagnosing osteoporosis with BMD are the spine and hip and femur. On the other hand, methods for assessing periodontal conditions and oral bone loss include clinical probing depth (PD), attachment levels (CAL), tooth loss, radiographic measures of alveolar crest height (ACH), absolute bone density (DXA, DPA, QCT), and computer-assisted densitometry image analysis (CADIA). The diagnosis of osteoporosis is often made by using bone density measurements. They are often expressed in relative terms (T scores and Z-scores); the Z-score is the number of standard deviations from the age matched average value of healthy women. The T-score statistic is a simple transformation of the Z-score, using sample mean and sample standard deviation rather than the population mean and standard deviation. A low Z-score indicates the bone density is lower than it should be for a patient’s age and sex. Osteoporosis is defined as a BMD loss of 2.5 standard deviations or more below the established mean. [17]A precise, accurate measure for the degree of osteoporosis in the jaws by dual-photon absorptiometry. [18-24]
A robust association of osteoporosis and periodontal disease has been noted. Osteoporosis of the alveolar bone may lower the resistance of the periodontium to infectious challenge and may result in a local infection of the periodontium that first invades the cortical bone and results in a dimensional change in the alveolar ridge. [24-25] Another possible mechanism involves increased production inflammatory cytokines, in that osteoporosis patients have elevated systemic levels of pro-inflammatory cytokines IL-1, IL-6, and TNF-α. These cytokines account for osteoclastogenic bone resorption-inducing cytokines and are also involved in the tissue response to periodontal disease. [26] Both osteoporotic as well as osteopenic conditions predispose an individual to loss of attachment eventually resulting into loss of tooth. [27-30]
Genco and Grossi proposed a model, based on elevated levels of cytokines associated with post-menopausal oestrogen deficiency. [31] Deficiency in estrogen causes upregulation of macrophages and osteoblasts, which in turn produce inflammatory mediators such as interleukins, TNF-α and GM-CSF. This results in generalized collagenolysis and bone resorption. On the other hand, Yoshihara et al, found weak association between periodontal disease and BMD. The influence of estrogen upon bone remodelling like upregulation of osteoprotegrin is known to inhibits receptor activator of nuclear factor kappa B ligand (RANKL) results in breakdown of alveolar bone. Thus, it could be postulated that accelerated periodontal breakdown in osteoporotic patients is possibly a result of combination of elevated inflammatory responses and locally increased resorptive potential. [31]
In a study by Taguchi et al, a significant difference in BMD at the third lumbar vertebrae and posterior tooth loss was found. Similar results were found by Earnshaw et al in their study on early post-menopausal women with BMD and tooth loss. [32] Another retrospective study by Astrom et al demonstrated a positive correlation between tooth loss and incidence of hip fracture. [33]
RISK FACTORS : 11 Periodontitis is an inflammatory disease characterized by loss of connective tissue attachment and alveolar bone. Like osteoporosis, it is a silent disease, not causing symptoms until late in the disease process when mobile teeth, abscesses, and tooth loss may occur. While the etiologic agent in periodontitis is a pathogenic bacterial plaque in a susceptible patient, periodontitis and osteoporosis have several risk factors in common. They include an increased prevalence with increasing age, smoking, and influence of disease or medications that may interfere with healing. The rate of progression of periodontitis sharply increases immediately after menopause.
Osteoporosis :Sex, Age, Low bone mass, Early menopause, Thin, small-framed body, Race
Lack of calcium intake, Lack of exercise, Smoking, Alcohol and/or caffeine, Heredity, Certain medications (e.g., steroids), Propensity to fall.
Periodontitis :Bacterial plaque, calculus, Age, Smoking or medications that inhibit healing and/or immune response, History of previous bone loss. Osteoporosis has been proposed as a risk factor for periodontal disease. These established or potential risk factors also provide significant information regarding differential etiology and contributing factors that will assist clinicians in preventing or managing these two diseases simultaneously.
Common Risk factors : Cigarette smoking, Nutritional deficiency, Increased age, Corticosteroid use, Immune dysfunction
UNIVERSAL RECOMMENDATIONS FOR ALL PATIENTS : Numerous interventions like adequate intake of calcium and vitamin D, regular weight-bearing and muscle-strengthening exercise, cessation of tobacco and alcohol, treatment of other risk factors.
THE ROLE OF FRAX IN MAKING THE DIAGNOSIS OF OSTEOPOROSIS : FRAX is a World Health Organization-sponsored, country specific fracture risk assessment tool that combines BMD at the femoral neck (or total hip) with a group of well-validated and weighted clinical risk factors for fracture that are largely independent of BMD. Finally, for individuals who have an elevated fracture risk based on FRAX, the term osteoporosis can be used for diagnosis. [34] It is based upon epidemiological data from 60,000 women and men studied prospectively to correlate risk factors for fracture with fracture outcomes and then validated in independent cohorts including more than 230,000 patients. It is useful as a way of predicting the risk of hip fracture and major osteoporotic fractures, i.e., clinical spine, hip, proximal humerus, and distal forearm fractures, in previously untreated men and women aged 40–90 years. Its use in the USA allows the assessment of fracture risk in both genders and four ethnic groups and is recommended primarily for individuals with a BMD finding of osteopenia.
As a result, the reduced BMD, characterizing osteoporosis and further alteration of trabecular pattern may lead to a more rapid jawbones resorption caused by periodontal disease, resulting in the invasion of periodontal bacteria. Invading bacteria, in turn, may alter the normal homeostasis of bone tissue, increasing osteoclastic activity and reducing local and systemic bone density by both direct effects (release of toxins) and/or indirect mechanisms (release of inflammatory mediators; in particular, interleukin-1 and interleukin-6). [35-42]
POSSIBLE MECHANISMS OF THE BI-DIRECTIONAL LINK BETWEEN OSTEOPOROSIS AND PERIODONTAL DISEASE (PD) :
The relationship between osteoporosis and PD may be supported by the following mechanisms : [43]
Systemic to local bone resorptive disease : Other than the hormonal effect, the systemic to local bone resorptive disease is considered for describing the link between osteoporosis and periodontitis. Osteoporosis of the alveolar bone may lower the resistance of the periodontium to infectious challenge and may result in a local infection of the periodontium that first invades the cortical bone and results in a dimensional change in the alveolar ridge. On the other hand, it also causes altered bone density in maxilla as well as mandible and further leads to increased alveolar porosity, microarchitectural deterioration of trabeculae, reduced remodelling rate, reduction in volume of the residual ridge, and decrease in the cortical thickness following invasion by periodontal pathogens.
Few studies conducted on hormone replacement therapy (HRT) carried out in humans have reported improved mandibular bone density by reducing gingival bleeding and mobility of the teeth. Another hormone associated with homeostasis of bone is Parathyroid hormone (PTH), which increases resorption of bone to ensure sufficient levels of calcium within the blood. Thus, intermittent PTH application also aids to improve healing of the periodontium thereby promoting bone regeneration. Further PTH is also known to promote homeostasis of bone by regulating pro-resolving lipid mediators that are known to promote macrophage efferocytosis. [50, 51]
Together, these interactions suggest a possible link of interaction of hormones related to bone remodeling and inflammation may be a mechanism that links osteoporosis and periodontitis. [52-53]
Genetics is known to have a major role in periodontal disease pathogenesis. Certain twin studies and family based studies conducted by Krall & Dawson-Hughes, 1993; Gueguen et al. 1995 have indicated that 60–85% of the variance in bone mineral density (BMD) is genetically determined, while Arden et al. 1996; Garnero et al. 1996 assessed the effect of other risk factors for osteoporotic fractures, such as quantitative ultrasound properties of bone, femoral neck geometry and bone turnover markers range, have also been shown to have a strong heritable component. Cummings et al. 1995; Torgerson et al. 1996 conducted a study on family history of fracture and reported it to be a risk factor for fractures independently of BMD. Candidate gene association studies have shown several polymorphisms that are associated with BMD, bone loss or osteoporotic fractures.
Deng et al 2000 carried out a study on post-menopausal women to assess heritability of wrist fracture which was estimated about 25%, whereas compared to another study of twins carried out by Andrew et al 2005 suggested that the heritability of wrist fracture may be as much as 54%. Nevertheless, the heritability of wrist fracture in both these studies was shown to be largely independent of BMD, suggesting that predisposition would be affected due to genetic influences on other factors such as bone turnover, bone geometry or even perhaps the risk of trauma. [63-64]
STUDIES LINKING OSTEOPOROSIS AND PERIODONTAL DISEASE :
Kribbs et al 1990 was the first one to study the association between osteoporosis and periodontal disease in which he compared the mandibular bone mass of 85 osteoporotic women with 27 normal women. They concluded that the osteoporotic group showed less mandibular bone mass and density and a thinner cortex at the gonion compared the normal group. No significant differences in clinical periodontal measurements were found between osteoporotic and normal groups. [82]
Klemetti et al 1994 conducted a study on women aged 48-56 years. They reported greater number of tooth loss in post-menopausal women from low bone density category. The authors also concluded, women from the higher bone density category were known to retain their teeth inspite of deep periodontal pockets better than those underlying osteoporosis. [83]
A case-control study carried out by Von Wowern and colleagues 1994 comparing 12 female patients having osteoporotic fractures and 14 normal women, reported significantly greater clinical attachment loss in the osteoporotic women compared with normal women. The authors concluded that the osteoporotic women has less mandibular bone mineral content, as measured by dual photon absorptiometry, than the 14 women. The mandibular bone mineral density values found were less than 2 SD for mandibular bone content for young normal women in 92% of the osteoporotic group and in 64% of the control group that also suffered from mandibular osteopenia. The relationship between osteopenia and severity of periodontal disease also examined in a sample from the Third National Health and Nutrition Examination Survey (NHANES III) of 11,247 participants ranging from 20-90 years of age. Osteopenia of hip was significantly associated with severity of periodontal disease (mean attachment loss ≥ 1.5 mm) in females and males independently of the confounding effects of age, gender, smoking or intake of dietary calcium. This association was increased even further within the post-menopausal women. [25]
Further, Taguchi et al 1999 assessed relationship between bone mineral density and tooth loss in elderly women. Studies revealed reduced bone mass when susceptible to greater occlusal forces for a longer period of time has been suggested as one of the cause for increased molar tooth loss. [84] Furthermore, teeth with furcation involvement are at a significantly greater risk of premature tooth loss. Therefore, one may expect more multi-rooted teeth to be lost in patients with osteoporosis if there is a correlation between periodontal disease and osteoporosis. [84-86] Females with osteoporosis are three times more likely to experience loss of teeth. Techniques used to assess oral bone loss include radiographic measures of alveolar crestal height (ACH), residual ridge resorption (RRR), and probing measures to assess clinical attachment level (CAL) and measures of tooth loss. Oral bone density is measured through absolute bone density (DXA, DPA, QCT, RA) and CADIA (computer assisted densitometric image analysis) to assess approximate alteration in density over time. [87-90]
Taguchi et al 1999 found a significant difference in BMD at the third lumbar vertebrae and posterior tooth loss. [91]
Wactawski - Wende et al 2001 in their study conducted on 70 post-menopausal women, found a significant relationship between alveolar crest bone height as a measure of periodontitis and skeletal osteopenia (femur and lumbar spine) measured by DXA. This relationship was found as a result of combination of all associated risk factors like bacterial plaque, years of menopause and smoking. Interestingly, a confirmed co-relation was found between osteopenia at the hip and clinical attachment loss within the same group participants. [90]
Bollen et al 2004 studied the association between osteoporotic fracture and tooth loss. A positive co-relation was seen between residual alveolar ridge height and incidence of osteoporotic fractures. Although, reduced BMI remains the primary cause for fractures. [92]
Darcey et al 2013 carried out a study to assess whether there is a relationship between the osteoporotic status of patients and the number of their teeth. Total of 359 patients were scanned and their data was collected on osteoporotic status, smoking status, alcohol consumption, age and the use of hormone replacement therapy. Dental panoramic tomographs were advised for each patient and the total number of teeth present were assessed. The authors concluded a statistically significant relationship between molar loss and osteoporotic status of all the scanned individuals. [93]
D C Penoni et al 2018 conducted a Longitudinal Study and study included retrospective follow-up of 6-10 years to assess effects of Bone Fragility and Antiresorptive Drugs on Periodontal Disease and Tooth Loss. This study aimed to assess effect of systemic bone fragility over severe periodontal clinical attachment loss (CAL) and tooth loss over the years and to check the influence of anti-resorptive medications and periodontal maintenance. Elderly women were assessed for bone mineral density (BMD) and for fracture risk assessment (FRAX) in a cross-sectional analysis. The authors concluded that the use of bisphosphonates not only improved the bone condition but also the periodontal status. On the other hand, periodontal maintenance also minimized the negative impact of low BMD on periodontal tissues in the studied population. [94]
Hsin-Hua Chou 2021 studied association between Bone Mineral Density and Periodontal Disease in Middle-Aged Adult. A total of 7298 patients aged between 40 to 44 underwent oral screening. Data as collected on quantitative ultrasound for the measurement of bone mineral density (BMD) and Community Periodontal index was assessed for periodontal disease. The results showed prevalence of 39.8% of periodontal disease in adults with osteoporosis, followed by 33.3% of periodontal disease in osteopenic patients. The authors thus concluded, low bone mass was associated with the increased risk of periodontal disease. [95]
The authors thus recommend that postmenopausal women and also men over the age of 50 years should be undergo BMD testing on regular intervals in order to diagnose a marked risk of future fractures. However, there may be a disruption of the homeostasis involving bone remodelling, hormonal balance, as well as inflammation progression and resolution. Nevertheless, both of these diseases warrant for a interdisciplinary management.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
