
Case Report | DOI: https://doi.org/10.31579/2690-4861/196
1 University of the Andes, Faculty of Medicine, Department of Morphological Sciences. Merida, Venezuela.
2 Servicio de Neurocirugía, Instituto Autónomo Hospital Universitario de Los Andes, Universidad de Los Andes, Mérida, Venezuela.
3 School of Medicine, Faculty of Medicine, Universidad de Los Andes, Mérida, Venezuela.
4 Resident of the fifth year of neurosurgery of the autonomous university institute of the Andes, Venezuela.
*Corresponding Author: Wilfredo Molina Wills, School of Medicine, Faculty of Medicine, Universidad de Los Andes, Mérida, Venezuela.
Citation: E O R Graterol, Wilfredo M Wills, L Arditi. (2022). Osteolytic Alteration, Cervical Myelopathy and Dysphonia Associated with Mucoepidermoid Carcinoma: A Case Report. International Journal of Clinical Case Reports and Reviews. 10(2); DOI: 10.31579/2690-4861/196
Copyright: © 2022 Wilfredo Molina Wills, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 December 2021 | Accepted: 30 December 2021 | Published: 08 January 2022
Keywords: mucoepidermoid carcinoma; myelopathy; osteolysis
Summary: A vertebral neoplasm of extraosseous origin, is that which affects the vertebra starting from a tissue that has metastized. Clinical diagnosis and imaging only provide an etiopatological approach due to various sources of metastasis, so early obtaining of material for sample analysis and timely treatment becomes important.
Objective: This study presents a 62-year-old male patient who manifested dysphonia, respiratory distress, cervical compressive myelopathy syndrome; being as a whole this picture with characteristics of increasing intensity and persistent imaging compatible with osteolysis of the spinous process of the fourth cervical vertebra.
Methods: lateral radiographs of preoperative cervical spine and cervical magnetic resonance without contrast in sequences T1 and T2 as well as cervical magnetic resonance without contrast axial cut sequence T2 were evaluated. A week after the diagnosis by image is taken to the operative table where resection of tumor mass associated with cervical paravertebral muscles, C4 laminectomy and exceresis of an extension of the tumor to the spinal canal (extradural) is performed and the anatomopathological study was performed.
Results: The patient presented improvement due to recovery of the respiratory bellows in the immediate post-operative period, although dysphonic persisted. The biopsy result reported mucoepidermoid carcinoma. We are interested in highlighting in this case the particular evolutionary association between the respiratory-laryngeal process, cervical osteolytic process and myelopathic manifestations as a regional development of the mucoepidermoid adenocarcinoma tous neoplastic activity.
Spinal metastases represent a challenge, usually and because of the variety of tissues that originate the process. The current measures of care for patients with tumors have led to survival with the appropriate quality to our time. The spine represents a very common location of metastases to the bone [1], of which 10% have been reported related to the cervical spine [2]. Pain and neurological deficit continue to guide the physician in the syndromatic diagnosis although the difference in evolutionary success can be located in post-surgical therapeutics. Advances in radiotherapy as the treatment of choice for vertebral metastases, and chemotherapy have improved the quality of life of patients [3].
Spinal cord compression myelopathy is defined by invasion of the medullary canal by a tumor that advances locally or by a metastasis that produces compression or displacement of the spinal cord [4], and is classified into external and internal. According to the metastasis is located intramedullary or extramedullary [5], being the most frequent metastases, those with origin in the breast, lung and prostate [6].
Male patient of 62 years of age, who manifests onset of current disease of one month of evolution, characterized by progressive pain cervical of strong intensity, of sharp type, with irradiation to shoulders, calm partially with non-steroidal anti-inflammatory NSAIDs, concomitantly progressive decrease of the muscular strength of the four limbs, respiratory distress and dysphonic. He also manifested alterations for urination and constipation, which is why he is referred to the University Hospital of the Andes Mérida-Venezuela. During the physical evaluation, he was vigilant, conscious, oriented, fluent language with prolonged pauses, preserved memory. Norm photo reactive isochoric pupils, overall decrease in muscle strength (quadriparesis), muscle hypo tonicity, osteotendinous hyporeflexy, non-clonus, non-Babinsky and Dyspnea during rest.
Images
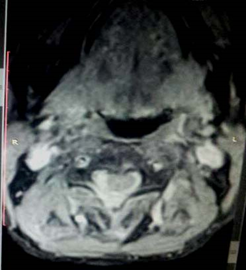
X-ray of the cervical spine was performed in anteroposterior and lateral projections where rectification of the physiological curvature is observed, with the absence of a spinous process of C4 (Fig. 1). In simple Cervical Nuclear Magnetic Resonance in sagittal and axial cut, a rectification of physiological curvature was observed, an image of ovoid, extradural, poorly delimited shape, with irregular edges, of solid characteristics, with isointense behavior in sequence T1 (Fig. 2), hyperintensive in T2 sequence (Fig. 3, 4), which occupies the posterior portion of the spinal canal from C3 to C4, with muscle invasion, and involvement of laminae, spinous process of the vertebral bodies. C3-C4 extradural spinal space occupant injury is diagnosed. (Fig. 1) Lateral X-ray of the cervical spine preoperative. Rectification of the physiological curvature and absence of spinous process of C4 are observed. (Fig. 2) Cervical magnetic resonance without contrast T1 sequence is observed with isointense posterior cervical extradural spinal image.



Surgical procedure
Patient who is taken to the operating table one week after the imaging diagnosis. Where a cervical incision was made posterior from C1 to C5, dissection by planes. Among the findings, we observed a rounded mass attached to cervical paravertebral muscle of 3x3x3 centimeters which we removed, with transformation of bone tissue to cartilaginous in c4 spinous process corroborated by histological study. Spinal decompression was then performed by C3-C4 laminectomy, extradural intraschid compressive mass exceresis.
Completed surgical act without complications, the patient had a satisfactory clinical evolution presenting improvement of the respiratory process.
Anatomopathological Findings
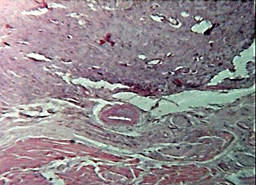
The histological sections of the examined material show malignant neoplasm of epithelial lineage consisting of cells with moderate to abundant amount of well-delimited cytoplasm, pleomorphic and hyper chromatic nuclei, others with chromatin in lumps, reinforcement of the nuclear membrane and evident nucleoli. Other cells show abundant well-delimited cytoplasm. These cells are arranged forming tubules, masses and nests that infiltrate the adjacent stroma. Cysts and areas with cribriform pattern with lights occupied by a cellular amorphous eosinophilic material are identified (Fig. 5, 6).


The spine is the third most frequent implantation site of systemic neoplasm metastases, then the lung and liver. Of the 40% of patients with spinal metastases, 10-20
Mucoepidermoid carcinoma at the cervical level is very rare, as well as its presentation. Imaging studies such as radiography, computed tomography and magnetic resonance imaging are very useful to make the diagnosis. The surgical treatment should have as its purpose the resection of the lesion in order to avoid complications and receive the treatment of chemotherapy and radiotherapy in the fastest way to avoid recurrence of the presented clinic.
None of the authors have conflicts of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
