
Research Article | DOI: https://doi.org/10.31579/2639-4162/197
Dept. Of Dentistry, JIS School of Medical Science & Research, Howrah, Kolkata, India.
Dept. of Microbiology, All India Institute of Hygiene and Public Health Kolkata, West Bengal India.
*Corresponding Author: Bhattacharyya Dept. of Microbiology, All India Institute of Hygiene and Public Health Kolkata, West Bengal India
Citation: Sudakshina Das, Bhattacharyya S, Mukherjee A, Chandra D, Sudakshina Das., (2024), Oral premalignant lesions and infections, J. General Medicine and Clinical Practice, 7(12); DOI:10.31579/2639-4162/197
Copyright: © 2024, Bhattacharyya S. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 27 June 2024 | Accepted: 08 July 2024 | Published: 12 July 2024
Keywords: premalignancy; leukoplakia; OSMF; oral proliferative verrucous leukoplakia; EBV; candida infections
Precancerous lesions of the oral mucosa, consists of a group of diseases, which should be diagnosed in an early stage. Oral leukoplakia, oral submucous fibrosis, erythroplakia are among the most common oral diseases having a high malignant transformation rate. Oral lesions, and viral infections (eg. HPV) are early signs of oral precancerous diseases even leading to squamous cell carcinoma. All doctors, dental surgeons, and especially dermatologists are encouraged to perform an accurate oral examination of all suspected cases to recognize the disease in its early stage.
Oral premalignant lesions can cause malignancies later on in life. Many infective agents can cause oral premalignant lesions. The premalignant oral disorder is a broad term covering a variety of pathologies which arises in the oral cavity. Early recognition and prompt management are pivotal for optimal outcomes. However, there is quite a significant knowledge gap in this area among medical practitioners (1).
Etiology
The most commonly described etiologies of premalignant oral lesions are tobacco exposure (smoke/ smokeless form) along with chronic alcohol consumption associated with certain microorganisms e.g.HPV (Human Papilloma virus), EBV (Epstein Barr virus) (Bánóczy et al., 2001; Sabashvili et al., 2018), fungal infections (chronic mucocutaneous candidiasis) etc.
Epidemiology
Oral premalignant lesions are found roughly in between 1.5% and 4.5% of the world's population and disproportionately have a sex predilection affecting men more compared to women [1]. Examples of common such premalignant conditions are leukoplakia, erythroplakia, oral proliferative verrucous leucoplakia (OPVL), oral submucous fibrosis (OSMF) and actinic cheilitis [2]. The latest nomenclature given by WHO of “oral potentially malignant disorders” (PMDR) has an overall prevalence of about 4.47% [2]. Animal studies have further shown that Candida can cause epithelial hyperplasia and cellular atypia [3]. Chronic mucocutaneous Candidiasis is a well-established premalignant condition. Habits like smoking also act synergistically with microorganisms to produce premalignant lesions. It can be mentioned here that smoking in Indian young women has gone up from 3.8% in 2009 to 6.2% in 2019. However, alcoholism can damage oral mucosa and decrease population of oral Streptococci, whilst having no effect on Candida spp.
Etiopathogenesis
Tobacco particles adhere to the tongue and buccal mucosa in smokers, also cause more adherence of pathogenic microbes like Candida albicans to oral mucosa. Then in smokers the incidence of chronic mucocutaneous candidiasis and other premalignant lesions will be commoner. Smoking impairs the host oral mucosal defence response and hence increases its susceptibility to C. albicans [4]. An association has already been reported between human papillomavirus (HPV) and OPVL. Between 0% and 89% of OPVL are reported to be HPV positive (5); it has also been reported in association with Epstein‑Barr virus infection in oral mucosa [6]. Candida infection is another infection associated with OPVL [5]. The proliferative effect of OPVL was explained on the basis of the high rate of field cancerization existing in OPVL patients [7].
Clinical features: -
Leukoplakia:
According to WHO -1998 (8) leukoplakia can be defined as: -
• Thin, smooth leukoplakia-Translucent thin grey soft flat plaques, usually with sharply demarcated borders.
• Thick, fissured leukoplakia - 2/3 of white plaques has a distinctly
white appearance, fissured and is leathery to palpation.
• Granular, verruciform leukoplakia - Lesions have surface
irregularities of nodular or granular nature with verrucous appearance. Erythroleukoplakia - Lesion showing intermixed red and white
--Proliferative verrucous leukoplakia was first described by Hansen in 1985. It is a subtype of verrucous/ verruciform leukoplakia characterized by a very aggressive evolution,characterized by resistance to treatment, and high recurrence rate.[9]. It has a high risk of malignant transformation [10]
In Candidal Leukoplakia, dysplasia occurs 4 -5 times more frequently than ordinary leukoplakia. Carcinomatous changes take place more frequently here [11]. PAS staining is used to differentiate it from other forms.
Oral submucous fibrosis:
In 1966, Pindborg defined OSMF as “an insidious chronic disease affecting any part of the oral cavity and sometimes pharynx. It is associated with juxta-epithelial inflammatory reaction followed by fibro elastic changes in the lamina propria layer, along with epithelial atrophy which leads to rigidity of the oral mucosa proceeding to trismus and in mouth opening.” [12]. An increased prevalence in India is due to increased use of areca nut (containing arecoline, arecadeine etc.) and smokeless tobacco product - gutkha, pan masala, flavored supari, etc. [13]. A classification system has been given on clinical presentation, progression of the disease only [14].
[Tab.1]. (kindly insert table 1)
Table 1: Clinical staging/classification of OSMF-
Stage I- Stomatitis and vesiculation: Stomatitis includes erythematous mucosa, vesicles, mucosal ulcers, melanotic mucosal pigmentation and mucosal petechiae
Stage II- Fibrosis: Blanching of the oral mucosa, vertical and circular palpable fibrous bands in the buccal mucosa, lips, mottled, marble‑like appearance of the mucosa. Reduction of mouth opening, stiff and small tongue, blanched and leathery appearance of floor of the mouth, fibrotic de‑pigmented gingiva, rubbery soft palate with reduced mobility, atrophic and blanched tonsils, shrunken cheeks with bud‑like uvula.
Stage III-Sequelae of OSMF: Speech and hearing difficulties may present due to involvement of tongue and eustachian tube. Treatment of OSMF depends on the degree of disease progression and clinical features. At early stages, stopping habit with nutritional supplements are done. At moderate stages, conservative treatment with intralesional injections is provided. At advanced stages, surgical interventions are required.
Epstein Barr Virus infection:
Epstein–Barr virus (EBV), a herpesvirus showing a typical oral ecology is commonly found in many oral lesions. This viral infection, considered a benign infection in most healthy individuals, is however associated with various premalignancies & malignancies [15]. To address the EBV infection, the host has to maintain efficient immune functions, including innate and adaptive immunities [15]
Clinical cases
A patient 65yrs old presented with a complaint of missing upper back teeth since 3years. (Fig.1). Patient’s oral examination revealed extraction. He had a habit of cigarette smoking about 1packet (10 cigaretttes)/ day and gutkha chewing since his college days. Intraoral examination revealed a thin white flat patch in the right buccal commissural region extending about (2.0- 2.5) cm across the occlusal plane (Kiesow zone). The lesion was non-tender, non-scrapable. It was a clear case of leukoplakia.
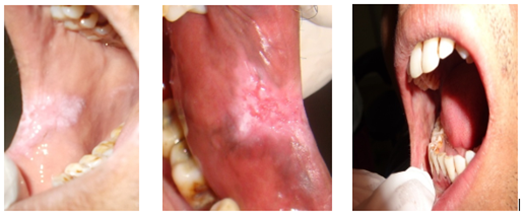
Figure 1: Oral leukoplakia Figure 2: Erythroplakia Figure 3a: OSMF
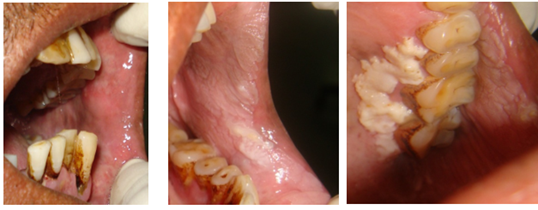
Figure 3b. OSMF
Figure.4a, - Oral verrucous leukoplakia Fig.4b, - Oral verrucous leukoplakia
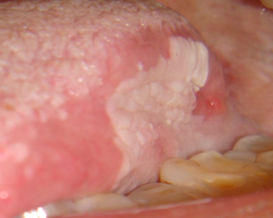
Figure.4c.- Oral verrucous leukoplakia
Figure.2 shows a mixed red and white(predominantly) flat patch in the left lateral commisure of the mouth. It was nontender non scrapable. The patient had a history of bidi(tobacco) smoking since last 23years about 3-4times/day. Fig.3a 3b shows blanching of left and right buccal mucosa, upper and lower lip with a marble like appearance, with shrunken bud-like uvula, reduced interincisal distance. On palpation vertical as well as circumoral fibrotic bands found with stiff tongue. Fig.4a, b,c shows diffuse white slightly raised plaques extending across the buccal mucosae, left & right commisure of mouth, the palatal mucosa, the buccal vestibule. There is a homogenous white raised leathery plaque having a granular texture in the left palatal mucosa about (2*3) cm in dimensions extending across the upper left premolar molar teeth. It is nontender non scrapable with a corrugated surface. The mechanisms causing premalignant oral lesions due to infections can be manifold and generally involve immune mediator cells and viral latency, like EBV. Nitrosamines produced by Candida albicans individually or in synerguly with other carcinogenic compounds, can activate some particular proto-oncogenes which may initiate such lesions
Clinical oral examination is the first and foremost method for screening various patches on the oral mucosa followed by scraping it with a sterile gauze. The experience and skill of the clinician is of utmost importance in such screening procedures, but it is not a method by which the risk level of any lesion can be calculated. There are various adjunctive screening methodologies which have been used to assess oral premalignant lesions that include vital staining with toluidine blue, exfoliative cytology, brush biopsy examination, autofluorescence, chemiluminescence, and biomarker assessment (from saliva, or serum) [16\. Candida albicans usually causes adherent white patches on oropharynx and tonsillar area, that bleed on forceful removal, and which can be subjected to culture and microscopy. Culture on SDA (Saburou’s dextrose agar) shows pasty smooth yeast colonies of Candida spp. that yield a positive reaction in Germ tube test, produce single terminal chlamydospores on Dalmau plate or Rice extract agar, and grow on subculture on SDA slant at 44 degrees C. EBV infections can be identified by serological tests like Paul- Bunnell test and molecular methods like PCR. EBNA-2 gene detection by PCR from the lesions or tissue is also helpful.
Management of PMDRs (2) starts with non-pharmacological treatment like habit cessation, followed by observation of the lesion for a long time followed by periodic check-ups There are no strict guidelines that can be applied regarding the duration of follow-ups. In general, a long-term follow-up examination is advised at 6–12-month intervals. In patients who remain disease-free for 3 years need perhaps no longer follow ups needed [17\. Various antifungal agents are given when Candida-associated leukoplakia is suspected in oral cavity. Other Management techniques include Chemoprevention- Retinoids, Vitamins (A, C, E), carotenoids, topical therapy- Bleomycin, Vitamin A, photodynamic therapy, surgical excision with or without grafting, electrocoagulation, cryosurgery and Laser surgery [18\. A recent study has reviewed the use of CO2 laser for management of leukoplakia and have shown that laser technique was reliable and reproducible with low morbidity [19].
An understanding of the infevtive as well as non-infective conditions leading to oral premalignant diseases and their prevention can result in better outcomes. The PMDRs are premalignant conditions that can transform into malignant tumours in many cases, if not detected early. Therefore, an understanding of their identification, pathogenesis, and prevention is of great importance in oral cancer. The scientific research on PMD s is still in an infant stage and requires more research to develop early intervention, better diagnostic and treatment strategies. This is also very important from public health viewpoint, since premalignant lesions due to infections are largely preventable.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
