
Review Article | DOI: https://doi.org/10.31579/2642-973X/103
Dr. med. Dipl.-Med. Internal Medicine, Rehabilitation, Social Medicine Hochwaldstraße 2 D-97769 Bad Brückenau Germany, Bavaria.
*Corresponding Author: Hans-Klaus Goischke, Dr. med. Dipl.-Med. Internal Medicine, Rehabilitation, Social Medicine Hochwaldstraße 2 D-97769 Bad Brückenau Germany, Bavaria.
Citation: Hans K. Goischke, (2024), Optimization of disease-modifying therapies (DMTs) in women with multiple sclerosis through daily vitamin D supplementation: requirement and duty of care? J. Brain and Neurological Disorders, 7(2): DOI: 10.31579/2642-973X/103
Copyright: © 2024, Hans-Klaus Goischke. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 April 2024 | Accepted: 18 April 2024 | Published: 25 April 2024
Keywords: multiple sclerosis; women´s health; disease-modifying-therapies; adverse events; vitamin d supplementation; cancer prevention
Multiple sclerosis (MS), like other autoimmune diseases, shows gender-specific physiological differences in the immunological reactivity of those affected. There is a worldwide deficit in the daily practice of caring for female multiple sclerosis patients. Women's health would be optimized by establishing women's neurologists. As one of several pillars in the therapy of multiple sclerosis, basic Vit D supplementation should be accepted as a “synergistic therapy pillar” from the onset of the disease. The indication arises from the effect of vitamin D on the regulation of the cytokine profile with promotion of the anti-inflammatory and reduction of the pro-inflammatory cytokine profile. A neurobiological benefit from vitamin D is expected on the course of MS, the activity of the disease and disability, the MRI lesions, and adverse events of DMTs. Puberty, adolescence, before, during and after pregnancy, menopause and older age are phases of altered immune responses. Different results in the vitamin D supplementation studies are explained by a lack of international consensus regarding the level of target values of 25(OH)D serum levels in autoimmune diseases, considering daily intake, duration, mode of administration, body weight and temporal adjustment to hormonal levels changes in the life of a woman with MS. The current pathophysiological and pathoimmunological findings are recorded and conclusions for practice are discussed. Overlaps between the disciplines of neurology, psychiatry, endocrinology, gynecology, and obstetrics as well as geriatrics require interdisciplinary collaboration.
Multiple sclerosis (MS) is a complex, autoimmune-mediated disease of the central nervous system, characterized by inflammatory demyelination and axonal/neuronal damage [1]. It is represented by relapse-associated neurological deterioration, but also by gradual increase in disability that is independent of relapse. The disease begins earlier than current diagnostic criteria can detect [2-4].
To reduce the inflammatory and relapsing activity with the formation of new lesions and to stop the irreversible clinical disability and neurodegeneration, the early use of over 20 highly effective disease-modifying therapies (DMTs) is becoming the focus of treatment, even in pediatric MS. [5-8]. Proactive management in clinical practice could significantly improve the quality of life of people with multiple sclerosis (PwMS), both in terms of the underlying disease itself [6] and in relation to the prevention of adverse events (AEs).
Autoimmune diseases, like MS, show gender-specific physiological differences in immunological responsiveness throughout the life of a woman with MS. There is also a clear connection between sex hormones and the clinical activity of MS [9]. The demand for a subspecialization in women's neurology, which deals with the phases of puberty, adolescence, pregnancy, peripartum care, menopause, and old age, i.e. the entire life of the woman, especially in wwMS, is a consequence of the endocrine, neurobiological, and immunological factors [9, 10]. An important contributing factor that likely contributes to the progression of age-related MS disability is immunosenescence, which affects both the adaptive and innate parts of the immune system [11]. Women with MS [wwMS] can exhibit premature immunosenescence. Another phenomenon of increasing age is a general, small increase in the production of proinflammatory cytokines [12]. In most current studies, a significant increase in serum concentrations of IL-10 and TGF-ß-1 was observed, so that an anti-inflammatory effect of Vit D suppl in wwMS would be a useful consequence [13].
2. Healthcare providers must particularly include women with MS in treatment decisions
Women have a higher incidence and prevalence of autoimmune diseases than men, at around 80%, and at least 85% of patients with multiple autoimmune diseases (polyautoimmunity) are female [14, 15]. This group of people goes through four major endocrinologically active episodes in their lives, puberty, pregnancy, postpartum period, and menopause.
During these periods there are influences on the innate and adaptive immune system with changes in pro- and anti-inflammatory cytokines [16-18]. Women are affected by multiple sclerosis approximately two to three times more often than men (ratio 2-3:1) among the approximately 2.8 million PwMS currently in the world, particularly if they live at higher latitudes above 40 degrees [19, 20]. Gender differences are also evident in that women are more susceptible to MS, while men can have a worse course of the disease [18].
Shared decision making (SDM) between PwMS and doctors is required with the aim of initiation, optimization and medication adherence in therapy with DMTs [21, 22].
In doctor-patient communication, AE may have a high priority, especially for problems relevant to women [23]. In family planning, the desire to have a child is increasingly revealed [24, 25] and the influence of DMTs on the child and MS requires intensive discussion [26]. It was found that the assessment of the desire for pregnancy and escalation therapy by the attending physicians was very different between MS specialists and non-MS specialists [27]. If wwMS obtain a second opinion that leads to discrepant results, severe psychological stress is inevitable. It is also recommended to start DMT early despite the desire to become pregnant [28].
2.1 Prioritization of “basic vitamin D therapy” for wwMS who want to have children
While in the 1990s pregnancy was discouraged in wwMS, the introduction of DMTs made it possible to recommend the desire to have children. To date, there has been a lack of consistent data on how therapy should be designed with DMTs before, during and after pregnancy and breastfeeding (in addition to estimating the benefit-risk profile of DMTs, especially fetal risks).
Guidelines sometimes recommended contradictory information on family planning and pregnancy [29]. Current research has been able to provide very detailed findings for the individual DMTs [29-34] before conception, in pregnancy, in the newborn period and during breastfeeding.
For optimal management, interdisciplinary collaboration between neurologists, gynecologists and family doctors is a conditio sine qua non especially since far-sighted advance planning and intensive advice for future parents is crucial for pregnancy. A “planned pregnancy” is preferable and should be prepared intensively in family planning discussions. However, exact recommendations for Vit D suppl for wwMS can hardly be found in the literature in guidelines.
2.2 Vit D supplementation to prevent undesirable side effects of DMTs
A study of residents in the northern hemisphere showed vitamin D deficiency (<20ng>
Without a doubt, the prospect of preventing or mitigating AE, not only from a psychological perspective, through an available, simple, complementary, inexpensive, and promising long-term daily vitamin D supplement (Vit D suppl) will make a decision to take a highly effective DMT easier. With appropriate monitoring of serum 25(OH) D levels (s25(OH)D), serum Ca and serum phosphate (also with additional determination of serum parathyroid hormone), vitamin D toxicity can be ruled out.
Since wwMS under DMTs are always associated with strict routine laboratory tests, this does not result in increased use of healthcare providers or patient burden.
3. Vitamin D supplementation as basic medication to prevent cervical cancer
In a multicenter cohort study, therapy with DMTs showed a 3.79-fold increased risk of developing a cervical anomaly compared to non-users of DMTs [36].
The gynecological cancer risk, including cervical cancer, has recently been highlighted as an important knowledge gap in the MS literature [37]. In a case report, a short-term progression of cervical dysplasia to invasive cancer due to natalizumab therapy was described [38]. Cervical cancer develops from healthy tissue and progresses to invasive cervical cancer via cervical intraepithelial neoplasia (CIN1/2/3) [39-41].
Currently, all cervical cancer is thought to result from an underlying persistent infection with oncogenic types of human papillomavirus (HPV) [42].
There is evidence that Vit D deficiency could be a risk factor for HPV DNA persistence and the associated development of CIN [43]. The prevalence of Vit D deficiency is more than 50% in adults in half of all countries [44].
Because persistent HPV infection is associated with reduced immune function, which can be enhanced by DMTs, but Vit D can reduce the HPV infection rate by improving the body's immunity, a reduction in morbidity and mortality is expected [41]. Details about the connections between Vit D and the vitamin D receptors (VDR) in the occurrence and progression of cervical cancer in the literature [41]. Figure 1

Figure 1: Mechanisms underlying the protective actions of Vit D in cervical cancer. [41]. Original illustration from Dong H et al. J Cancer 2024;15(4), Ivyspring International Publisher.
For Vit D to have an effective influence on the inflammatory cytokines, which play an essential role both in MS itself and in the development of cervical anomalies, serum target values of 40-100 ng/mL 25(OH)D are required for Vit D suppl. D should be aimed at and should be administered when starting DMTs to prevent cervical cancer (basic prevention). Sustained cytokine production is a consistent feature throughout the entire course of the MS disease and therefore requires long-term daily Vitamin D administration [45]. Increased dietary intake of vitamin D could also reduce the risk of cervical cancer neoplasia [46].
Several studies have found an inverse relationship between the frequency of cervical neoplasia and vitamin D levels [47]. The preventive and therapeutic role of the endocrine vitamin D system has been documented in numerous in vitro and in vivo studies. Calcitriol plays a regulatory role in fundamental cancer-related processes such as cell proliferation, apoptosis, cell differentiation, angiogenesis, autophagy, inflammation, oxidative and energy metabolism, and modulation of the immune response [47-49]. Figure 2

Figure 2: Antitumoral actions of calcitriol in cervical cancer cells. In cervical cells, calcitriol activates the vitamin D receptor (VDR), which binds with retinoid receptor X (RXR) and the heterodimer VDR-RXR is recruited to vitamin D-responsive elements in promoter regions of vitamin D-target genes, modulating the transcription mediated by RNA polymerase II. By this mechanism, calcitriol blocks the expression of some oncogenes such as the oncogenic potassium channel EAG1 or human cervical cancer oncogene HCCR-1; furthermore, calcitriol reduces proliferation and inflammation. On the other hand, calcitriol increases the expression of some critical cell cycle regulators such as p21, increases the maturation of some microRNAs with anti-cancer-related functions and promotes the expression of peptides with antiviral activity such as cathelicidin and defensins that could limit HPV infection. Together, these mechanisms support the protective role of calcitriol on cervical cancer.
Original illustration from [47] Avila et al. MDPI.
Because chronic infection by the human papillomavirus (HPV) is considered a pathological factor for the development of premalignant and malignant lesions of the cervix [50], calcitriol (1,25 (OH)2D3), the active metabolite of vitamin D, could be via the Synthesis of cathelicidin and defensins exert antiviral activity [47].
The proactive recommendation for action, i.e. “basic prevention” with Vit D suppl with the start of DMTs, is based on the experience that long-term Vit D suppl has an effect on cervical intraepithelial neoplasia grade 1 (CNI1), synonymous with low-grade squamous epithelial lesion (LSIL). 50,000 IU twice a month, showed CIN1 regression [51]. In a study with 12,500 IU Vit D (suppositories intravaginal) three evenings per week for 6 weeks, a good anti-inflammatory and antidysplastic effect was developed in CIN1 stage, but not in CIN2 stage. [52]. The mechanism is explained by a possible clearance of HPV from lesions [43, 52].
4. Breast carcinoma and s25(OH)D levels – sufficiently assessed in monitoring with DMTs?
In the general population, an association between low s25(OH)D levels and post-menopausal breast cancer (BC) was verified 16 years ago [53]. 85% to 96% of BC patients had an s25(OH)D value <20ng>
The molecular mechanisms of 1,25(OH)2D3 action include regulation of cell proliferation and apoptosis. They reduce the ability of cancer cells to metastasize, inhibit angiogenesis and inflammatory processes associated with cancer [58]. Although preclinical studies have shown an antineoplastic effect of 1,25(OH)2D3 on BC, no effects of Vit D suppl on BC risk or BC incidence have been determined in RCTs to date. The error could be due to the fact that no optimal maximum threshold for s25(OH)D value and no optimal supplement dose (daily/monthly) have been established internationally [59].
In the RCTs without benefit, Vit D daily doses of 2000IU or monthly bolus doses were administered [59].
Therapy with monoclonal antibodies, such as CD20, could reduce the protective mechanism against cancer by suppressing normal B cells against tumor production and tumor lysis or lead to activation of the immune system in the sense of a pro-tumorigenic effect [60, 61]. The results on cancer prevalence and incidence in PwMS are contradictory and could be registered as increased, decreased or equal risk [61]. Caustics report the occurrence of gynecological carcinomas with
natalizumab (BC, cervical CA[Z-Ca]); Fingolimod (BC); teriflumide (Z-CA); Cladribine (Z-CA); alemtuzumab (BC); ocrelizumab (BC); Dimethyl fumarate (BC, Z-CA); IFN-ß1a (BC); [60-62], although unreported cases cannot be ruled out.
If you are over 50 years old with MS and have had two changes in therapy with DMTS, regular monitoring should be carried out due to an increased risk of cancer. The increased incidence of cancer in this population over 50 years may be due to reduced estrogen levels [62].
5. Inflammatory bowel disease (IBD) as undesirable side effects of anti-CD20 antibody therapy
Rituximab, ocrelizumab, ofatumab and ublituximab are currently included in the treatment of MS as monoclonal anti-CD20 antibodies (AK). The suppression of inflammatory activity is achieved through predominantly selective depletion of CD20+ B cells, but also CD20+ T cells [5-8]. During therapy with ocrelizumab, over 38 cases of immune-mediated colitis, such as Crohn's disease (13 cases), ulcerative colitis and microscopic colitis (5 cases each), unspecified colitis (11 cases), autoimmune colitis (2 cases) and drug-induced colitis (3 cases) published [63, 64]. Reports of further case studies exist [65].
Women were affected at 76%. With the anti-CD20 antibody rituximab, there is a sixfold increased risk of developing inflammatory bowel disease (IBD) and women seem to predominate here too [66].
The cause of IBD/immune-induced colitis caused by anti-CD20-AK therapy may be an abnormal B cell-mediated T cell regulation because of B cell depletion [67]. Homeostasis of pro- and anti-inflammatory stimuli and CD20+ cells play an important regulatory and protective role in the gastrointestinal tract [67-69].
The lack of regulatory role of mature B cells on pathogenic CD4+ cells would be an explanation for colitis [67,68, 69]. The almost complete depletion of peripheral B cells up to 6 months after ocrelizumab leads to the deficit of their physiological function in the production of secretory immunoglobulins such as IgA and IgM antibodies, the lack of regulatory B cells (reg.B) and the anti-inflammatory cytokine IL -10, which physiologically inhibits the mechanisms of Th1 cells and prevents the proliferation of antigen-specific T cells [70-72].
A Vit D suppl. promotes the formation of anti-inflammatory IL-10 with high doses of Vit D suppl [73].
Concordant mechanisms in the pathogenesis of MS and IBD
The role of vitamin D in MS and the regulation of intestinal mucosal immunity is recognized [74-77]. [Figure 3,4,5]
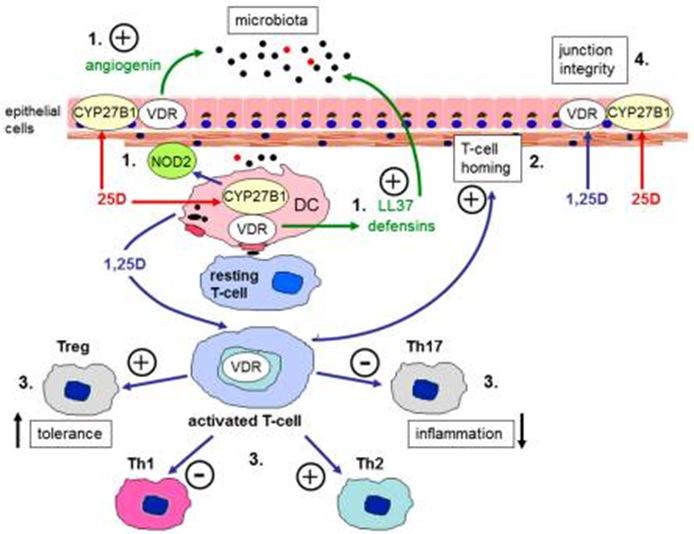
Figure 3: Vitamin D and barrier function in the gastrointestinal tract. Schematic representation of the expression of the vitamin D receptor (VDR) and vitamin D-activating enzyme (CYP27B1) in human colonic epithelial cells, antigen presenting cells such as dendritic cells (DC), and T cells. Immune responses to vitamin D occur either via systemic 1,25-dihydroxyvitamin D (1,25-(OH)2D) or local conversion of 25-hydroxyvitamin D (25-OH-D) to 1,25-(OH)2D. Possible target mechanisms include: 1) interface with microbiota (induction of antibacterials such as angiogenin, cathelicidin (LL37), defensins or intracellular pathogen recognition proteins such as nucleotide-binding oligomerization domain containing 2 (NOD2)); 2) T cell homing to sites of inflammation; 3) suppression of inflammatory Th17 and Th1 cells and induction of tolerogenic Treg and Th2 cells; 4) enhanced expression of epithelial membrane junction proteins. Original figure from Fletcher J et al. [76], MDPI
Regulatory T cells (Tregs) play a key role in the pathogenesis of IBD as well as MS. Their phenotype and function in MS or in the inflamed intestinal mucosa and in the periphery of patients with IBD are significantly disturbed compared to healthy controls. In PwMS, reduced resting and increased activated CD4+CD25+FOXP3+ regT cells were observed [78], while in IBD a reduced number of peripheral Treg cells and an increased number of peripheral Th17 cells as well as proinflammatory cytokines such as IL-6, IL-1β, IL-12, IL-23 and TNF have been documented [79, 80].
The increased number of proinflammatory cytokines is a significant part of the pathogenesis in both diseases [77, 81, 82]. and can lead to progression for both diseases [70].
It is believed that disrupted bacterial and viral gut microbiota are part of the pathogenesis of MS and that this mediates an altered gut-microbiota-
brain axis. The composition of the gut microbiota influences the production of serotonin in the intestine, which in turn influences the serotonin-mediated regulation of systemic immune function [83, 84, 85, 86].
Butyrate, a microbial metabolite in the gut, may contribute significantly to alleviating a disrupted intestinal barrier. In MS, butyrate-producing bacteria were reduced [87].
The microbiome also plays an essential role in IBD [88]. The composition of the gut microbiota may change in the early stages of IBD. The fluctuation in gut microbiota composition is greater in IBD patients than in healthy individuals [89, 90, 91]. Butyrate is also a potential therapeutic agent in IBD to reduce inflammation and maintain IBD remission [92, 93].

Figure 4: Vitamin D modulates different cellular and molecular mechanisms of CNS-resident cells and of the blood-brain barrier (BBB) involved in multiple sclerosis pathology. (Left) Schematic representation the cellular and molecular mechanisms involved in MS/EAE [Experimental autoimmune encephalitis pathology at the level of CNS-residents cells and the BBB. (Right) Schematic representation Vitamin D impact on cellular and molecular mechanisms involved in MS/EAE pathologyat the level of CNS-resident cells and the BBB (↑) Increased; (↓) decreased [77], Original figure from Galoppin et al; Oxford University Press].
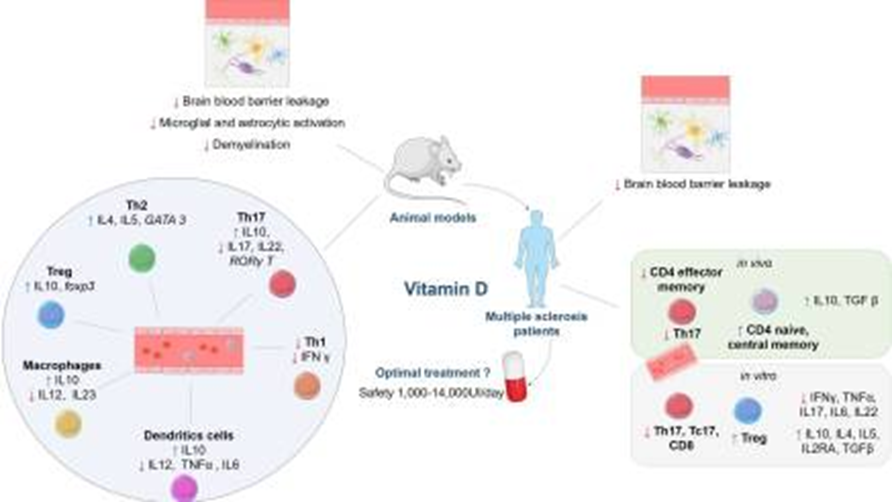
Figure 5: Original figure: Graphical abstract aus Galoppin et al. [77], Oxford University Press.
6. Vitamin D suppl as DMTs replacement before, during and after pregnancy
If some newer DMTs must be discontinued for safety reasons without long-term observation and there is a risk of a relapse, high-dose vitamin D supplementation could be used as a replacement for interrupted therapy with DMTs during pregnancy, postnatally and during breastfeeding.
The mother is the only source of vitamin D during pregnancy. If the expectant mother does not receive adequate vitamin D intake, the fetus or newborn suffers from hypovitaminosis with all the negative consequences [94].
The neuroactive steroid has a high level of safety in all periods of pregnancy and postpartum and can positively influence the activity of MS. The worldwide prevalence of hypovitaminosis D before, during (in each trimester of pregnancy) and after pregnancy in the general population requires healthcare providers [95, 96, 97, 98] to report an increased need for therapy especially in wwMS.
In a notable study, it was demonstrated in women (without MS) that the probability of pregnancy and live birth increased if there were sufficient preconception Vit D levels 25(OH)D (≥ 75nmol/l=30ng/mL) [99].
This intensive care must begin when you want to have children, because fertility depends on the Vit D level [95].
6.1 Advantages of vitamin D supplementation during pregnancy
Numerous studies have shown that hypovitaminosis D is associated with the occurrence of preeclampsia, premature birth, low birth weight, low gestational age (small infants), indication for cesarean section and gestational diabetes in women without MS [95, 100]. Effects of hypovitaminosis D on the newborn and on child development in terms of poor immune and skeletal development, allergies and respiratory infections have shown that neural, musculoskeletal, and psychomotor growth as well as bone health are negatively affected [100].
There is countless evidence that an optimal Vit D serum level has a positive influence on the progression of MS and that supplementation can also be used during pregnancy and breastfeeding [101, 102].
For women who want to have children, as part of prevention for the course of pregnancy and for maternal and child health, it is crucial to start Vit D suppl at least 2 months before conception (before placentation and trophoblast invasion) with around 5000 IU/the Vit D to achieve an optimal Vit D serum level (serum level over 100nmol/l=40ng/ml) [99].
Vit D deficiency can also be the cause of recurrent embryo implantation failure and recurrent fetal loss [94, 103, 104].
The influence of Vit D on placental gene expression and inflammation within the placenta creates an optimal starting position for the children [102-104].
Since a reduced vitamin D3-[25(OH)D] serum level also promotes, among other things, autoimmune diseases of the thyroid gland, which are also found in MS as a side effect (comorbidity) of alemtuzumab [105,106, 107], and also an insufficient 25(OH)-D serum level increases the risk of preeclampsia and premature birth and leads to a lower birth weight, an optimal Vit D level should be achieved [108]. Bi et al. found that Vit D supplementation during pregnancy was associated with a reduced risk of shortened gestational age and improved infant growth in gravid women without MS. Vit D at doses of 2000 IU/day or lower during pregnancy may reduce the risk of fetal or neonatal mortality [109].
Fetal excess of vitamin D metabolites in the fetus is unlikely if maternal Vt D levels are within normal limits. During pregnancy, up to 4000 IU Vit D/day was supplemented, resulting in sufficient Vit D levels without increased risk of toxicity to the women or the newborns. Serum levels of 25(OH)-D-above 125 nmol/l (50ng/mL) should not be reached [110].
The Endocrine Society (UK) recommends a safe upper limit for 25(OH)D intake in pregnancy of 10,000 IU/day for those over 19 years of age who are Vit D deficient [111]. Since the relapse rate of RRMS increases three months postpartum, but correction of Vit D hypovitaminosis can lead to a reduction in the annual relapse rate, this therapeutic arm should not be neglected to reduce disease activity [112]. In a large cohort study that recorded a high maternal milk intake (2-3 glasses/day, enriched with 400IU Vit D/1.2l liter)) during pregnancy, a lower risk of MS was found in the daughters [113]. In mothers with an insufficient Vit D level (<30>
6.2 Health status during pregnancy in MS
The main problem in monitoring is the detection of a relapse, although experience shows that the acute risk of recurrence in the third trimester is reduced by approximately 70% compared to the period before pregnancy. However, Winkelmann et al. also found an increase in the relapse rate in the first trimester [118]).
A pathophysiological explanation as to why immunological tolerance is suppressed during pregnancy and thus also the activity of MS was found by Engler et al. [ 119]. In MS, Tregs were generally reported to have reduced suppressive potential. The authors demonstrated that progesterone greatly increases regulatory T cells (Tregs) via interaction at the glucocorticoid receptor in T cells [119]. The enrichment of Treg cells could also be enhanced by Vit D supplementation and contribute to relapse prevention because Tregs are essential for suppressing autoreactive reactions. Jeffery et al. were able to show that 1,25 (OH) 2 D3 has a significant and direct effect on the generation of FoxP3 + CTLA-4 + Treg, which are capable of strong immunosuppression [120].
The complex care provided by various disciplines during this period also requires the doctor-patient relationship to respond to the patients' individual ideas, especially regarding complementary and alternative forms of therapy, because around 80% of PwMS use these. Around 50% of PwMS confront the treating doctors about these forms of therapy, predominantly neurologists. If the therapist is convinced of the principle of action of the neuroactive steroid Vit D in MS, a “substitute DMT” is made available to the patient and thus a feeling of security is conveyed, this additional psychological factor should not be underestimated [121]. The active inclusion of PwMS in their treatment has invaluable value, especially as it can prevent the patient from choosing an ineffective or dangerous alternative therapy [121, 122].
7. Effects of menopause in wwMS
Menopause, which is linked to biological, hormonal, and immunological changes, has a significant impact on women`s quality of life, especially in women with MS [123]. Gender differences in concentrations of serum levels of total 25(OH)D, 24.25(OH)2D, free 25(OH)d and free 1,25(OH)2D3 are present and resulted in lower values in wwMS [124].
Several studies have reported worsening of MS symptoms during menopause [11, 123]. The most frequently reported symptoms were fatigue, anxiety, and depression, which could be positively influenced by Vit D supplementation [123, 125]. Vit D deficiency leads to an increase in aging processes [126]. Age is also associated with an increased risk of side effects of some multiple sclerosis therapies. Both somatic and reproductive aging processes can contribute to the development of progressive multiple sclerosis [127]. 1,25(OH)2D3 could contribute to neuroprotection [77,128, 129].
8. Comorbidities in PwMS
The higher prevalence of depression in women than in men in the general population highlights the need to specifically assess mental health in older women with MS [130].
Comorbidity, defined as the “total burden of diseases other than the disease in question itself,” was currently found in 46.5% of PwMS with one or more comorbidities [131]. Elderly and female PwMS with depression were most frequently affected at 16.45% [131]. Previous studies found depression at 23.7% and anxiety at 21.9%. Migraines were more common in wwMS. [131, 132, 133].
Other studies showed depression in 19-40%, although the influence of different DMTs varies [134, 135].
Positive effects on these comorbidities can be expected at s25(OH)D of 40-60ng/mL [105, 125].
The occurrence of fatigue has been observed in 80% (60-90%) of PwMS. On the other hand, a reliable connection between DMTs and fatigue could not be verified [136, 137], although there is evidence of an association [134].
Because of the high prevalence in PwMS even without DMTs, Vit D suppl could achieve a significant reduction in fatigue and an improvement in quality of life [125, 138, 139]. If patient-reported outcomes (PROs) were included in studies, the influence of DMTs could be better assessed [137].
Because PwMS suffer more frequently from cardiovascular diseases, Vit D suppl would reduce the risk of serious cardiovascular events, especially in older PwMS [140].
In a study of 2000 IU/day, over 5 years in the general population, no significant reduction in total invasive cancers or major cardiovascular events was observed. In the final discussion and summary, a daily dose of 2000 IU/day was described as “high dose”, which is not internationally defined and should therefore be viewed as very critical [141]. It suggests an optimal daily dose.
In this and in other studies, obesity (BMI) was not intensively considered, although subgroup analyzes showed a treatment-related reduction in cancer incidence among normal-weight participants in the study [141]. Longitudinal evidence suggests that BMI may be associated with altered response to vitamin D supplementation and would partially explain the observed decreased outcomes of supplementation for various end goals in individuals with higher BMI [142].
Because a higher vitamin D level in the serum is associated with a reduction in new active cortical and subcortical lesions and a smaller lesion volume, prescription of vitamin D is an essential therapeutic element in everyday practice [143].

Figure 6: Spectrum of effects of vitamin D supplementation in PwMS Increase (↑) decrease (↓)
9. Obesity promotes disability progression in PwMS
Worldwide, the number of obese people in the world population has increased rapidly. In Germany, 46.6% of women are overweight or 19% are obese (BMI > 30kg/m²) [144, 145]. In studies with Vit D suppl with little benefit [146, 147], the connection between obesity (BMI) and response to Vit D suppl is not taken into account, because a higher BMI also requires an increased effective dosage of Vit D in order to achieve the necessary s25(OH)D values to be achieved. It is approximately 2.5 times higher than the dose [142]. The level of Vit D suppl especially in pregnant women with obesity, would therefore also have to be based on the BMI values. Placing this parameter at the center of proactive therapy is supported by the knowledge that obesity is associated with a poorer health-related quality of life per se. Obesity promotes progressive disease progression, greater disease severity, increased disability scores (higher EDSS [Disability Status Scale]) and a faster increase in cognitive disability. In particular, the degree of disability progresses more quickly in obese than in non-obese MS patients [148, 149].
The treatment of MS should therefore also include weight management in order to better slow down the clinical progression, also with regard to menopause and weight gain during this period [148, 150].
A convincing argument for recommending and achieving wwMS normal weight should be the stronger benifit ocrelizumab therapy in this group of people. BMI influences CD20 Kinetics. A higher BMI showed a faster repopulation rate of B cells, which contradicts a reduction in disease activity [151].
Adipose tissue is recognized as an independent endocrine organ and proinflammatory cytokines such as interleukin Il-6, tumor necrosis factor-alpha (TNF-alpha) and MCP-1 (monocyte chemoattractant protein-1) are produced. A state of systemic inflammation is a hallmark of excessive obesity. Obesity is characterized by a relative excess of proinflammatory and decreased anti-inflammatory adipokines. Due to these mechanisms, vitamin D supplementation aimed at reducing IL-6 and TNF-alpha could curb obesity-induced inflammation and reduce brain volume loss and the neuroinflammatory process [150, 152-154]. Overweight and obesity in middle age are risk factors for future gray matter loss and dementia [148, 155]. Impairment of insulin signaling, mitochondrial dysfunction and chronic inflammation are discussed as pathophysiological, biochemical mechanisms [148]. 25(OH)D and its active form, 1,25(OH)2 D3, are responsible for attenuating inflammation and oxidative stress as well as mitochondrial respiratory function. Hypovitaminosis D promotes insulin resistance [156].
An association of increased pediatric MS risk with obesity has already been observed in children, and obese children did not respond well to first-line medications (interferon beta and glatiramer acetate) [157].
About 80% of people affected by autoimmune diseases are women. They bear a high burden due to increased morbidity, the changed hormonal phases in their lives and an increased risk of polyautoimmunity [17].
To slow the progression of physical and cognitive impairments in patients with RRMS, a more proactive management strategy is recommended, including earlier use of highly potent DMTs and close monitoring of the clinical and radiological response to treatment [158, 159,160]. But there is also evidence that DMTs, such as anti-CD20 antibodies ocrelizumab, reduce relapses in PwMS over the age of 60 [women with 654%) [161]. The treatment of MS depends not only on fate, but also on place of residence, the family situation, the proximity of MS specialists and the therapeutic inertia of the attending physicians, especially if there is a desire for pregnancy [27, 162].
Regarding medical care, it is important whether the wwMS lives in an urban region, which has a clear advantage over a rural residence [163].
It can be speculated that “therapeutic lethargy” exists not only in the decision to use DMTs, but also in proactive add-on therapy with long-term daily high-dose Vit D suppl. Only a few countries recommend daily Vit D suppl in their guidelines [164]. Both from the literature and from national guidelines of the neurological community, the impression arises that with regard to the specific recommendations/prescriptions for long-term, daily, high-dose Vit D supp, which is based on s25(OH)D values in the range of 40-100ng /mL oriented, an indifferent attitude has so far been established.
An unjustified therapeutic nihilism due to the lack of presence of pathoimmunological mechanisms seems to be the cause here. There is evidence that Vit D signaling plays a greater role in maintaining T cell tolerance in women than in men. Decreased Vit D and sex-specific Vit D signaling could contribute to the breakdown of T cell self-tolerance and increased incidence of MS in women [77].
A further argument for the reluctance to prescribe could be seen in published individual case studies on the problem of vit D intoxication due to extreme overdosing (supraphysiological doses) [165, 166, 167]. Hypercalcemia is more likely to be the cause here, but serum Ca levels are easy and inexpensive to monitor [168]. There is a balance between net Ca absorption from the intestine and calcium excretion in the kidney. An excessive production of the active 1,15(OH)2D3 results in an adequate production of the catabolic enzyme 25-Hydroxyvitamin D-24-hydroxylase (CYP24A1), thus largely avoiding Vit D toxicity [ 169].
The benefit of a five-year Vit D suppl with 2000IU/day was proven with a 22% reduction in autoimmune diseases in the general population. In high-risk groups (e.g. obesity), a higher daily dose must be targeted [170, 171]. An interruption of Vit D suppl leads to a decline in protective functions [171].
Disturbed immune homeostasis in MS requires therapy-relevant Vit D doses and 25(OH)D values
What makes it more difficult for the healthcare provider is the unwillingness of MS specialists to internationally define 25(OH)D serum levels (Vit D deficiency (≤50nmol/l=20ng/mL); Vit D insufficiency (≤51-74nmol /l=21-29ng/mL); Vit D sufficiency (≥75nmol/L=30ng/mL), Vit D optimal (100-150nmol/L=40-60ng/ml and upper safety limit (250nmol/L=100ng/ml). (multiply by 2.5 to convert ng/ml to nmol/L). The inconsistencies in the cut-off levels in the individual countries for many years in vit D research illustrate the dilemma [172, 173].
In addition, s25(OH)D target values are missing in autoimmune diseases, which cannot be compared with healthy people.
There is also no attempt at consensus to agree on target values of s25(OH)D values in the upper normal range (100ng/mL) in studies. The lack of agreement makes it difficult to assess studies, especially since widespread obesity is not yet regularly included.
For 13 years, neurologists in Sweden have been informing PwMS about the benefits of Vit D therapy [174].
Since 2018, the Multiple Sclerosis Society of Canada has recommended for PwMS a serum 25(OH)D level of 20-50ng/mL (50-125nmol/L) through a daily vitamin D supplementation (600-4000 IU/day) and as an add-on therapy also to influence bone health (risk minimization for osteoporosis, falls and fractures) [164].
The practice of withholding Vit D suppl in many countries is astonishing because of the known pathophysiological and immunopathological findings on its effect on MS, as side effects are hardly to be expected.
Optimal pregnancy results – only through interdisciplinary collaboration in pregnancy planning
To achieve optimal maternal and fetal outcomes in wwMS and pregnancy, especially in the case of simultaneous immune-mediated comorbidities interdisciplinary collaboration between neurologists, gynecologists and endocrinologists is not only desirable but absolutely necessary.
Vit D suppl is one of the best ways to make optimal use of preventative measures months before conception. It is evident that this increases the probability of pregnancy and live birth and reduces the risk of abortion ([99, 100, 175]. The “feat” will be to provide women with a desire to have children who do not live in large cities with MS centers to provide timely care based on the latest findings. It is undisputed that a large number of questions arise, and the answers must depend on the respective severity of the MS. The latest findings on the effects of previously used and current immunomodulatory and immunosuppressive therapeutics and the translation into practice will shape the outcome for mother and child. In the Covid-19 era, the risk of maternal complications can increase with wwMS and pregnancy [176], which is why Vit D suppl is also recommended for this indication [177, 178].
Prevention of adverse events - A strong psychological factor for therapy decisions and adherence to DMTs
Motivating wwMS to take highly effective DMT therapy depends on the AE that may occur. The effects of 1,25(OH)2D3 on the innate and adaptive immune system are undisputed and findings from the last decade on the pathophysiological and immunological mechanisms of vitamin D's effect on the course of MS itself [77, 168, 179], but also on AE, such as autoimmune thyroid diseases, autoimmune skin diseases (vitiligo, alopecia) [180]. Colitis, cardiovascular diseases, due to various DMTs (including alemtuzumab, natalizumab, fingolimod, teriflunomide) [181], Vit D suppl should be offered to wwMS as a potential addition to long-term immunotherapeutic treatment [168].
PwMS rarely achieve a protective effect with effective s25(OH)D values through necessary daily sun exposure, especially when living in higher northern latitudes (temperate zones [182]). The protective effect of sun exposure appears to be both vitamin D and affect non-vitamin D signaling pathways, which is important for prevention, especially for people with a genetic susceptibility to MS [183, 184]. In summer, around 20-30% of the total daily UV radiation occurs the time between 11 a.m. and 1 p.m. and 75% to the time between 9 a.m. and 3 p.m. (solar time, not local time). In temperate regions there are considerable seasonal fluctuations in the UV radiation hitting the earth's surface; closer to the equator these are much higher lower [185]. Very low levels of sun exposure are associated with worse disease progression and poorer health-related quality of life in PwMS [20].
A high-dose Vit D suppl (3000-11,000 IU/day) with s25(OH) values between 30-60ng/mL depending on the individual absorption rate is necessary to positively influence the course of the complex immunological disease MS [77, 186].
Low s25(O) levels at the onset of MS are associated with an increased risk of relapse. It was shown that with a genetic predisposition to higher s25(OH) values, the risk of relapse was reduced [187]. In addition, vit D suppl could also potentiate therapy with DMTs (e.g. fingolimod) because calcitriol blocks the migration of autoreactive CD4+ T cells into the CNS [77]. This adjuvant therapy forms the basis for several health benefits and should be incorporated into a comprehensive health concept as a holistic treatment [188, 189].
A recent study with follow-up over 22 years showed how the health of older women can be influenced by long-term Vit D supplementation in the general population with 400 IU/day [190]. A 7% reduction in cancer mortality has been verified and this should lead to long-term positive health outcomes in wwMS.
Since PwMS, early therapy with DMTs is recommended [1, 191]. and multiple DMTs are used over the course of MS and exposure may last for decades [192], the potential cancer risk plays a serious role. As the age of PwMS increased to 62 years or older, the risk of cancer increased over a follow-up period of 8.4 (4.3-10.4) years [193].
The effectiveness of Vit D Suppl on cancer mortality depends critically on the daily intake of this dietary supplement (reduction by 12%); bolus administration had no effect [194].
In a critical systematic review of Vit D supplementation in PwMS, it was found that the evidence for a positive effect of Vit D despite discrepancies showed a reduction in new MRI lesions in various studies and Vit D has positive effects on MS-related depression [96, 195].
Low serum calcidiol levels are further associated with cognitive impairment [[126, 196]. This result alone is an indication for the prescription of vitamin D.
The fact that negative results of RCTs on Vit D suppl cannot be the indication for prescription based solely on the result of the primary endpoints for recurrences [147] is supported by criticism of the circumstances of RCTs with dietary supplements [197].
If the results of a study are put into practice [198], discontinuing anti-CD-20 therapy as a sensible option in PwMS over 50 years of age with inactive MS, vitamin D could be used through the mechanism of sealing the BBB (blood-brain barrier) inhibit the migration of immune cells into the CNS and close the therapy gap [77].
An important argument for using Vit D therapy as an additive component in B cell depleting therapy, especially rituximab, is the increased risk of infection. The majority of PwMS were women [ (199, 200]. The proactive administration of Vit D with protective effect of 1,25(OH)2D3 through the mechanism of induction of antimicrobial peptides can reduce the risk of acute respiratory tract infections and urinary tract infections [201, 202, 203].
A current study shows the need to carry out gender-specific analyzes in the treatment of MS in PwMS to slow down the increase in disability [204].
Women develop stronger reactions of the innate and acquired immune defences and are therefore more likely to develop autoimmune diseases. Women with multiple sclerosis could achieve a better quality of life through daily vitamin D supplementation, especially during phases of hormonal changes such as pregnancy. The special nature of vitamin D metabolism during pregnancy prompts healthcare providers to aim for optimal 25(OH)D levels. Hypovitaminosis D is expected to have negative effects on the mother, fetus and newborn. The daily dose should be titrated individually and should be based on the achieved 25(OH)D serum levels, whereby high oral vitamin D doses are likely, and 25(OH)D serum levels of over 40ng/mL are the minimum. It is biologically plausible to aim for target values in the upper normal range to correct the immunological imbalance in multiple sclerosis and comorbid autoimmune diseases.
Because not all DMTs are available in all countries and regions, treatment equity could be achieved when prescribing vitamin D as daily basic medication and supplementary or replacement medication for DMT through easy availability, low costs, neglected side effects and a multifactorial benefit become.
“The practice of medicine remains more an art than a science” (Gavin Giovannoni, 2017) [205].
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
