
Case Report | DOI: https://doi.org/10.31579/2690-1897/164
1 UOC General Surgery, ASST Cremona & University of Brescia, UOC Anesthesiology, ASST Cremona.
2 UOC General surgery, ASST Ospedale Maggiore di Cremona.
*Corresponding Author: Baiocchi GL, UOC General surgery, ASST Ospedale Maggiore di Cremona.
Citation: Dendena A, Quarti LM, Celotti A, Bonafede M, Baiocchi GL et al (2023), Open Left Hepatectomy with Caval Thrombectomy for Huge HCC with Left Hepatic vein Tumoral Thrombosis, J, Surgical Case Reports and Images 6(5); DOI:10.31579/2690-1897/164
Copyright: © 2023 Baiocchi GL, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 11 August 2023 | Accepted: 21 August 2023 | Published: 12 September 2023
Keywords: hepatocellular carcinoma; tumor thrombus; inferior vena cava tumor thrombus; left hepatic vein tumor thrombus; cirrhosis-Child A; hcc; open hepatectomy
Hepatocellular carcinoma (HCC) is the most common primary liver tumor, and its incidence has been on the rise worldwide. It is a common cause of cancer-related death. HCC carries a poor prognosis and is challenging to manage, especially when diagnosed in advanced stages [6]. We present a rare case of open left hepatectomy with caval thrombectomy for huge HCC with left hepatic vein tumoral thrombosis.
Multiple types of primary malignant tumors can arise from the liver, namely, hepatocellular carcinoma (HCC), cholangiocarcinoma, hemangiosarcoma, angiosarcomas and hepatoblastoma, with HCC being the most common, accounting for more than three-fourth of liver primary malignant tumors [1]. The common risk factors for HCC include chronic viral hepatitis types B and C, alcoholic liver cirrhosis, non-alcoholic steatohepatitis (NASH), and obesity [2]. Patients presenting with advanced or metastatic HCC have a very poor
prognosis [3]. HCC is one of the tumors commonly associated with intravascular invasion and tumor thrombus formation [4]. Patients who present with tumor thrombus have worse outcomes and limited treatment options [5]. Our patient presented with HCC associated with intravascular invasion of middle hepatic vein and left hepatic vein tumoral thrombosis.
This is the case of a 61-years old Caucasian male in mild cirrhosis (Child A) that presented a left liver lesion on ultrasound investigation. Neoformation appeared solid, rounded with an inhomogeneously hyper-echogenic echostructure and vascularized. 10 cm in diameter, with clear-cut contours. The finding was compatible in the first hypothesis with hepatoma.
Then an MRI was performed that showed almost complete atrophy of the left hepatic lobe in the context of which some biliary ectasic branches are recognized. The voluminous solid lesion had clear and slightly lobulated margins, size 11x10x10,5 cm. Non-homogeneity in the weighed T2 sequences and likely intralesional haemorrhagic outbreak of 17 mm to the middle third on the back and 10 mm in the anterior to the upper third. The lesion, characterized by marked restriction of the diffusivity in DWI/ADC, had modest heterogeneous enhancement in the arterial phase, with rapid washout in the successive phases of the dynamic study and hypointensity of homogeneous signal in hepatospecific phase. (Figure. 1a-b)
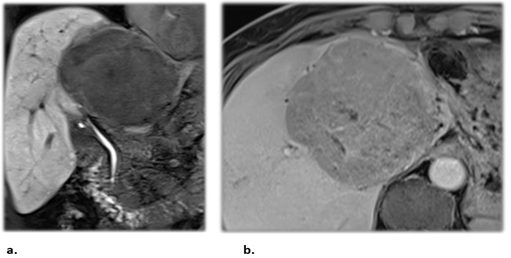
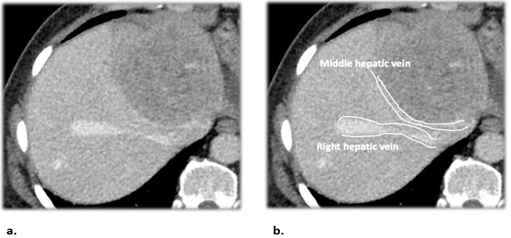
The lesion, probably originated from the fourth segment, determined a clear imprint and dislocation of the middle hepatic vein and the portal branch for S8, also marked, but pervious. Not recognizable the portal branch of the left and the homolateral hepatic vein. Ectasica (12 mm) the right hepatic vein (Figure. 2a-b).
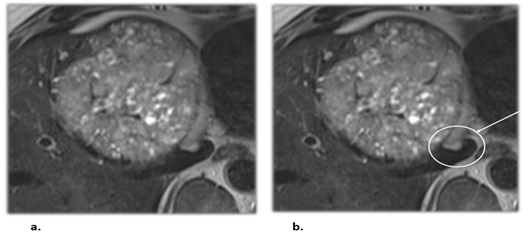
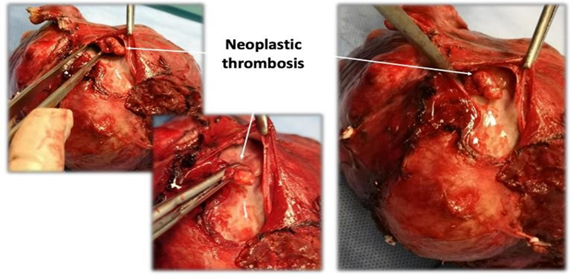
Careful analysis of the image made it possible to identify the neoplastic thrombosis in cava vein from left hepatic vein (Figure. 3a-b).
In the caudate lobe was also identified a roundish nodular lesion of about 2 cm with characteristics signal and enhancement superimposed on the lesion of greater dimensions, to be referred in the first hypothesis to satellite nodule.
The major lesion did not show the typical pattern of HCC, however it did have a peripheral capsule. These characteristics in the first hypothesis put diagnosis of primitive hepatic lesion, but with question between atypical HCC, cholangiocarcinoma and hepatic primary lymphoma; It was therefore recommended a bioptic evaluation for a histological characterization.
HCC was diagnosed after the needle biopsy (18 G needle, Bio Prince fullcore) in July 2023.
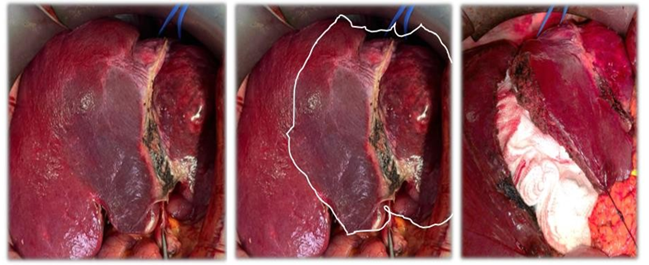
Because of the advance stage of disease, in multidisciplinary board, it was decided to treat the patient with an open left hepatectomy with caval thrombectomy, in order to remove tumor with a curative intent. We chose open and extended left hemilhepatectomy (Fig. 4) also because clinically the patient did not show hepatic failure (no history of previous hepatitis infection; no encephalopathy; albumin 4,87 g/dl; bilirubin 0,84 mg/dl; INR 1,12).
After performing a J-shaped laparotomy, there was no peritoneal carcinosis. The right liver was characterized by steatosis without frank cirrhosis, while the left liver was entirely occupied by voluminous mass (S3-S4), partly exophytic, which at the ultrasound control included the left hepatic vein (inside which a thrombosis was seen projecting into the Cava lumen) and the middle hepatic; the left portal vein was involved 2-3 mm from the origin and appeared hypotrophic and the right vessels were free, albeit dislocated.
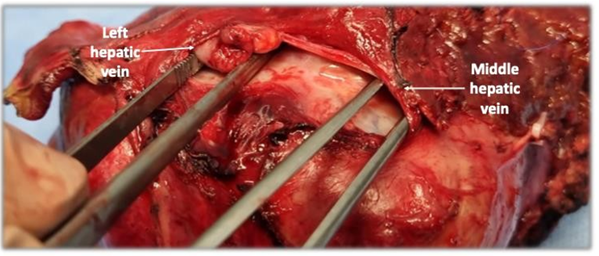
The case was therefore considered resectable. Following cholecystectomy, complete dissection of the hepatic hilum was carried out with ligation of all the left arterial branches (starting from both the left gastric and the common hepatic), ligation of the left portal vein and preparation of the left and middle hepatic blockages (Figure. 5).
We continued with the removal of the left caudate with macroscopic control of radicality, parenchymal section with CUSA and 3 pedicular clampings total of 11, 13 and 17 min.
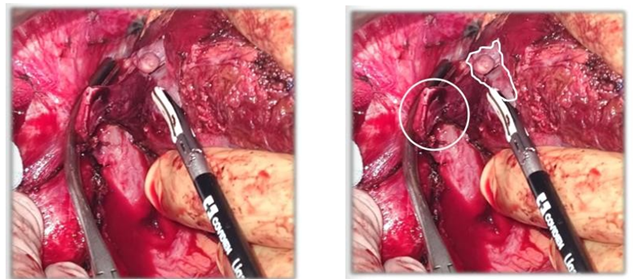
At the time of the hepatic section was evidenced thrombosis on the left (Figure. 6), with the head of the thrombus that appeared attached to the wall and it was removed with the piece.
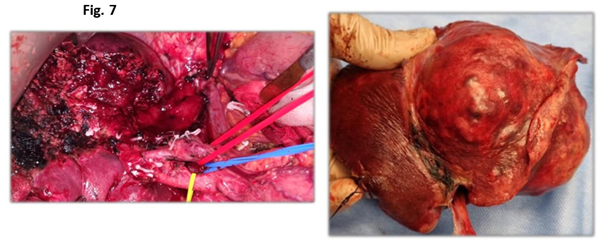
Instead middle hepatic vein was free from tumoral thrombus but involved by cancer in the parenchyma. Following left hepatic artery and left portal vein ligation, successful excision (Figure. 7) of the tumor (S1, S2, S3, S4) was achieved without complication, with good control of hemostasis (Floseal) and biliostasis (Tachoseal).
Total operation time was 6 h, with blood loss of 300 ml and no RBC transfusion was performed.
In agreement with anesthesiologists, we decided to monitor the patient in the ICU for the next day (1 day in ICU) and the patient was discharged on 5 post operatory day.
This case illustrates the importance of accurate radiological diagnosis as an aid to surgery. Thanks to MRI identification of the thrombus, it was possible to remove it and prevent the iatrogenic spread of the disease in the circulation.
In fact, on August 2023, the histological report of the surgical piece defined a moderately differentiated hepatocarcinoma G2 with poorly differentiated areas G3; infiltration of large vessels (middle hepatic vein), perineural invasion and neoplastic lymph-vascular embolization. The surgical edges and three lymph nodes analysed also appeared microscopically free of carcinoma, so pTNM staging [A.J.C.C.C. 2017; 8. Ed.] was found to be pT4N0 with macroscopic and microscopic radicality.
Patients with HCC who present in advanced disease stage or with large tumor thrombus have limited treatment options and poor outcomes. This case adds to the limited number of reported cases of HCC with left hepatic vein tumor thrombus extended in IVC. More clinical trials and new treatments are needed to improve the outcomes in patients with advanced HCC [6].
The diagnostic study, the multidisciplinary evaluation, the open surgical approach and the “en block” removal of the mass including the thrombus were fundamental for the radicality of the intervention.
The patient monitoring over time will allow us to understand the long-term effectiveness of this surgical technique, which can be used with curative intent in selected cases.
Future study should be established for improving the overall survival of the HCC patients with IVC and left hepatic vein TT.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
