
Case-Report | DOI: https://doi.org/10.31579/2692-9392/003
*Corresponding Author: Richa Gupta, MS Ophthalmology, FICO (UK), Consultant- Department of Glaucoma, CL Gupta Eye Institute, Ram Ganga Vihar Phase II, Moradabad-244001 (India).
Citation: Richa Gupta (2019) Open globe ocular injury- Etiology and outcome, J.Archives of Medical Case Reports and Case Study. 2(1); DOI:10.31579/2692-9392/003
Copyright: © 2019 Richa Gupta, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 29 August 2019 | Accepted: 06 September 2019 | Published: 10 September 2019
Keywords: ocular trauma; open globe injury; ocular trauma score
Ocular open globe injuries are often disabling for both the victim and society, as most of these eyes may remain unsalvageable. Many initial variables have been identified which can help in predicting the final visual outcome in these eyes. Also, various prognostic tools have been validated by previous studies. This article aims to review all these factors.
Ocular injury is a frequent and often preventable cause of visual impairment. Although it comprises of only 2% of all ocular injuries, it accounts for over half a million cases of monocular blindness worldwide. [1-5] In 1998, World Health Organization estimated the global incidence of open globe injuries (OGIs) to be 3.5 per 100,000 persons per year. [5]
The primary aim in managing these eyes is to restore the structural integrity of the globe at the earliest by primary repair. For eyes that are beyond repair, a primary enucleation may be considered. Inspite of improved micro-surgical facilities available now-a-days, the prognosis of most of these eyes remain grim.
Definitions of ocular trauma
Penetrating injury: Full-thickness corneoscleral wound with no exit wound
Perforating injury: Full-thickness corneoscleral wound with an exit wound
Intra-ocular foreign body (IOFB): Foreign object retained within the globe
Various mechanisms of injury have been identified by previous authors. In most of the articles, a sharp object (projectile objects, such as glass) has been reported to be the most common cause of injury, others being wooden/ metal stick injuries, fist injury, pellet, fall etc.[3,6,17,18]
There is a significantly higher incidence of OGIs in males, suggesting either more aggressive behaviour or involvement in higher risk indoor and outdoor activities. [2,3,6-9] Also, a correlation has been observed
between the place of injury and gender. Street and work place related injuries are more common in males, where-as home- related injuries are seen more in females. The most common place of injury in pediatric age group is school. [6,12-14,17,18]
Haavisto et al [21] reported that, 36% of eye injuries caused by Pellet guns resulted in permanent impairment. In November 2016, American academy of ophthalmology also recommended five safety tips to avoid toy related eye injuries. [22]
In their study, Gupta et al [16] found that injuries were more prevalent in pre-school and school age group, most of injuries occurred at home, majority of domestic injuries were caused by assault, wound size in accidental injuries was less as compared to those with assaults and, no case of sympathetic ophthalmitis was reported during follow-up.
Variables Affecting Final Visual Outcome
Previous studies have reported several preoperative factors associated with visual outcome of surgical repair in OGIs, most significant being the presence or absence of RAPD, presenting VA, and size of wound.[10-19,23-25] Other variables include age, [8-12] location of wound, [14- 20,20,22] lens damage, [13]vitreous haemorrhage (VH),[13,15,17,19] retinal detachment (RD), [12-19] and presence of intraocular foreign body (IOFB) [3,12,13,17,19],The outcome is significantly worse if the RAPD is present at the initial examination. Previous studies have shown that the presenting VA of less than 6/60 has significantly worse outcome as compared with an initial VA of more than 6/60. [17-19, 23-25]
Agarwal et al [25]in their study reported an association of hyphema and adnexal injuries with poor visual outcome, however reports by Rahman et al, [18] and Agarwal et al [23] did not corroborate this. Studies by Groessl et al, [15] Pieramici et al, [17] Rahman et al, [18] and Williams et al [27] have shown that visual outcome in cases where only single initial procedure was required is significantly better than those requiring more than one procedure.
Post traumatic endophthalmitis is most important complication of OGIs associated with worse final vision. Its incidence range from 4.9% to 54.2%. [28-31] RD is also a major complication in OGIs, associated with worse visual outcome, [31]
Ocular trauma score (OTS) and CART model
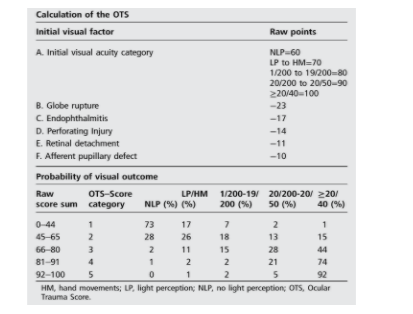
Various system has been reported to predict final visual outcome on the basis of pre identified presenting factors. In 2002, ocular trauma score (OTS) developed by Kuhn et al [32]from eye injury registry. They listed initial poor VA, rupture, endophthalmitis, perforations, RD and APD as factors negatively affecting the final VA. OTS scores range from 1 (most severe injury and worst prognosis at 6 months follow-up) to 5 (least severe injury and least poor prognosis at 6 months). Each score is associated with a range of predicted post-injury visual acuities. It has a predictive accuracy of approximately 80%, which means that the OTS will be accurate 4 out of 5 times.
Open globe injury present with management dilemmas to an ophthalmologist. The visual prognosis of such eyes is often difficult to assess. The OTS may help them in this regard. The initial visual acuity can be useful for non- ophthalmologists to help predict the final visual prognosis in OGIs.
Conflicts of interest: There are no conflicts of interest
Ocular injury is a frequent and often preventable cause of visual impairment. Although it comprises of only 2% of all ocular injuries, it accounts for over half a million cases of monocular blindness worldwide. [1-5] In 1998, World Health Organization estimated the global incidence of open globe injuries (OGIs) to be 3.5 per 100,000 persons per year. [5]
The primary aim in managing these eyes is to restore the structural integrity of the globe at the earliest by primary repair. For eyes that are beyond repair, a primary enucleation may be considered. Inspite of improved micro-surgical facilities available now-a-days, the prognosis of most of these eyes remain grim.
Penetrating injury: Full-thickness corneoscleral wound with no exit wound
Perforating injury: Full-thickness corneoscleral wound with an exit wound
Intra-ocular foreign body (IOFB): Foreign object retained within the globe
Various mechanisms of injury have been identified by previous authors. In most of the articles, a sharp object (projectile objects, such as glass) has been reported to be the most common cause of injury, others being wooden/ metal stick injuries, fist injury, pellet, fall etc.[3,6,17,18]
There is a significantly higher incidence of OGIs in males, suggesting either more aggressive behaviour or involvement in higher risk indoor and outdoor activities. [2,3,6-9] Also, a correlation has been observed
between the place of injury and gender. Street and work place related injuries are more common in males, where-as home- related injuries are seen more in females. The most common place of injury in pediatric age group is school. [6,12-14,17,18]
Haavisto et al [21] reported that, 36% of eye injuries caused by Pellet guns resulted in permanent impairment. In November 2016, American academy of ophthalmology also recommended five safety tips to avoid toy related eye injuries. [22]
In their study, Gupta et al [16] found that injuries were more prevalent in pre-school and school age group, most of injuries occurred at home, majority of domestic injuries were caused by assault, wound size in accidental injuries was less as compared to those with assaults and, no case of sympathetic ophthalmitis was reported during follow-up.
Previous studies have reported several preoperative factors associated with visual outcome of surgical repair in OGIs, most significant being the presence or absence of RAPD, presenting VA, and size of wound.[10-19,23-25] Other variables include age, [8-12] location of wound, [14- 20,20,22] lens damage, [13] vitreous haemorrhage (VH),[13,15,17,19] retinal detachment (RD), [12-19] and presence of intraocular foreign body (IOFB) [3,12,13,17,19], The outcome is significantly worse if the RAPD is present at the initial examination. Previous studies have shown that the presenting VA of less than 6/60 has significantly worse outcome as compared with an initial VA of more than 6/60. [17-19, 23-25]
Agarwal et al [25] in their study reported an association of hyphema and adnexal injuries with poor visual outcome, however reports by Rahman et al, [18] and Agarwal et al [23] did not corroborate this. Studies by Groessl et al, [15] Pieramici et al, [17] Rahman et al, [18] and Williams et al [27] have shown that visual outcome in cases where only single initial procedure was required is significantly better than those requiring more than one procedure.
Post traumatic endophthalmitis is most important complication of OGIs associated with worse final vision. Its incidence range from 4.9% to 54.2%. [28-31] RD is also a major complication in OGIs, associated with worse visual outcome, [31]
Various system has been reported to predict final visual outcome on the basis of pre identified presenting factors. In 2002, ocular trauma score (OTS) developed by Kuhn et al [32] from eye injury registry. They listed initial poor VA, rupture, endophthalmitis, perforations, RD and APD as factors negatively affecting the final VA. OTS scores range from 1 (most severe injury and worst prognosis at 6 months follow-up) to 5 (least severe injury and least poor prognosis at 6 months). Each score is associated with a range of predicted post-injury visual acuities. It has a predictive accuracy of approximately 80%, which means that the OTS will be accurate 4 out of 5 times.
In 2008, Schmidt et al [20] developed classification and regression tree (CART) model to prospectively validate the VA prognosis in OGIs. Gupta et al [6] found this useful in predicting the final visual outcome based on some initial factors. Scott R, [33] Shah et al, [34] and Unver et al [35] reported usefulness of OTS in prognosticating final visual outcome in different types of ocular injuries. Wai Man et al [24] reported that OTS has high prognostic accuracy to predict final visual outcome. However Knippers et al [36] reported that both the OTS and CART models are accurate predictors of visual acuity outcomes after open globe injury.
Open globe injury present with management dilemmas to an ophthalmologist. The visual prognosis of such eyes is often difficult to assess. The OTS may help them in this regard. The initial visual acuity can be useful for non- ophthalmologists to help predict the final visual prognosis in OGIs.
There are no conflicts of interest
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
