
Case Report | DOI: https://doi.org/10.31579/2768-2757/141
1Department of Thoracic Surgery, Guilan University of Medical Sciences, Rasht, Iran.
2Department of Internal Medicine, Inflammatory Lung Diseases Research Center, Razi Hospital, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran.
3Department of Cardiology, Guilan University of Medical Sciences, Rasht, IR Iran.
4Department of Physiology, Razi Clinical Research Development Center, Guilan University of Medical Sciences, Rasht, Iran.
5Department of Genetics, Razi Clinical Research Development Center, Guilan University of Medical Sciences, Rasht, Iran.
*Corresponding Author: Mohaya Farzin., Department of Thoracic Surgery, Guilan University of Medical Sciences, Rasht, Iran.
Citation: Manouchehr Aghajanzadeh.,Reza Pourbahador.,Omid M. Rad.,Ali A. Foumani.,Azita Tangestaninejad, et al, (2024), One-stage operation for two large hydatid cysts in the left lungs, causing severe compression of the heart and liver in a 34-year-old female, Journal of Clinical Surgery and Research, 5(7); DOI:10.31579/2768-2757/141
Copyright: © 2024, Mohaya Farzin. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 September 2024 | Accepted: 18 October 2024 | Published: 24 October 2024
Keywords: liver; echinococcosis; lung; heart tamponade
Background: Echinococcosis remains a significant health hazard in endemic areas, including the Middle East, Mediterranean countries, and Central Asia. In younger individuals, pulmonary disease appears more commonly, but bilateral pulmonary involvement is rare. Concomitant pulmonary and liver hydatid disease may occur in 4% to 25% of patients with hydatidosis.
Case presentation: A 34-year-old previously healthy woman from northern Iran with no history of lung or liver disease presented with symptoms including palpitations, shortness of breath, moderate Good pharmacovigilance practices (GVP) engorgements in the right upper quadrant and left-side chest pain, and low-grade fever over the past month. Imaging revealed a cyst in the left lung, causing compression of nearby structures and a shift of the mediastinum to the right side. A cyst with a laminated membrane and septation was also found in the liver. Due to the symptoms caused by the cysts, surgical intervention was performed. The patient underwent surgery to remove the lung cyst via left-side anterolateral thoracotomy and to remove the liver cyst via right-side anterolateral thoracotomy and phrenotomy. The patient was discharged in good condition.
Conclusion: In areas where a disease is commonly found, lung and liver hydatid cysts can co-occur. The heart may become compressed, potentially leading to tamponade. For young patients, surgery should be carried out using a one-stage procedure.
Hydatid disease is a significant public health concern, prevalent in regions such as the Mediterranean, Far East, South America, and the Middle East, including Iran. It is caused by a parasite called Echinococcus granulosus. Humans become infected when they ingest parasite eggs from contaminated vegetables, soil, or water. Hydatid cysts can affect any organ but are most commonly found in the liver (50%–77%) and lungs (18%–35%) and occasionally in other organs. Concomitant liver and pulmonary hydatid cysts occur in 4-25% of patients and may be found during routine clinical exams or screening [1-4]. Hydatid liver cysts may not show any symptoms or may lead to complications such as infection or rupture. When the cyst ruptures, it becomes vulnerable to bacterial infection, causing complications. This can be observed on a CT scan, confirming the cyst's infection. The image finding will contribute to the final diagnosis of cyst infection, which presents as a hepatic abscess [1, 3-5]. A cyst can rupture the biliary system, through the diaphragm into the chest cavity, or directly into the abdomen. The cyst may rupture due to trauma, increased pressure, or during Albendazole treatment [3-6]. A ruptured hydatid cyst in the peritoneal cavity can cause symptoms such as abdominal pain, urticaria, anaphylaxis, sudden death, or shoulder pain due to irritation of the diaphragm [5]. Patients may experience symptoms such as cough, chest pain, shortness of breath, sputum, fever, coughing up blood, and allergic pneumonia [1, 3]. The complications of pulmonary hydatid cysts include rupture, secondary infection, pyopneumothorax, hydropneumothorax, suppuration, and, rarely, compression of the heart [6-8]. Infection-infected cysts can be challenging to differentiate from a lung abscess or neoplasm lesion [1, 3]. X-ray, CT, and MRI are valuable for diagnosing thoracic hydatid cysts. Abdominal ultrasound, CT, MRCP, and ERCP are diagnostic tools for liver hydatid cysts [2, 4]. The indications for surgery include large cysts close to the surface, likely to rupture, infected cysts, cysts in vital locations, and cysts presenting with symptoms [2-4]. n intrapleural or intraparenchymal rupture, thoracotomy and laparotomy are needed with evacuation, omentoplasty, capitonnage and decortication, and pericardiotomy [1, 3]. This case aims to evaluate the clinical presentation, diagnosis, treatment, and outcomes of this case.
A 34-year-old woman was brought to the emergency department with complaints of shortness of breath, progressive dyspnea, palpitations, exertional dyspnea, left-sided chest pain, difficulty breathing while lying down, and right upper quadrant pain. She lives in a small city in the north of Iran. During her physical examination, her vital signs indicated tachycardia, hypotension, and elevated jugular venous pressure. Her cardiac enzymes, blood chemistry, and complete blood count were average, except for high levels of eosinophils (30%). A chest X-ray and CT scan revealed a significant cystic lesion in the left lung, causing compression of the left border of the heart (Figure 1,2,3,4,5).
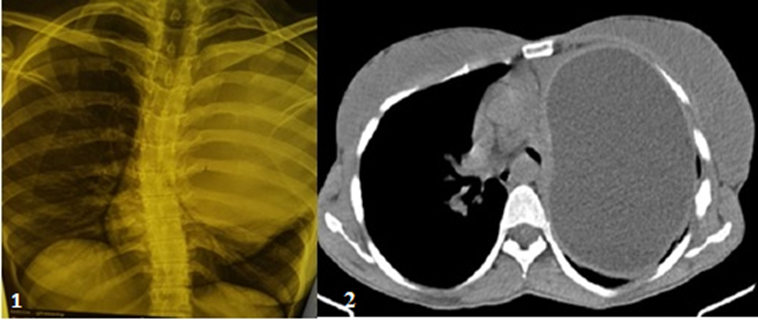
Figure 1: shows CXR with a substantial cystic lesion of the left lung, which compressed the heart and mediastinum.
Figure 2: shows a CT scan with a substantial cystic lesion of the left lung, which compressed the heart and mediastinum.
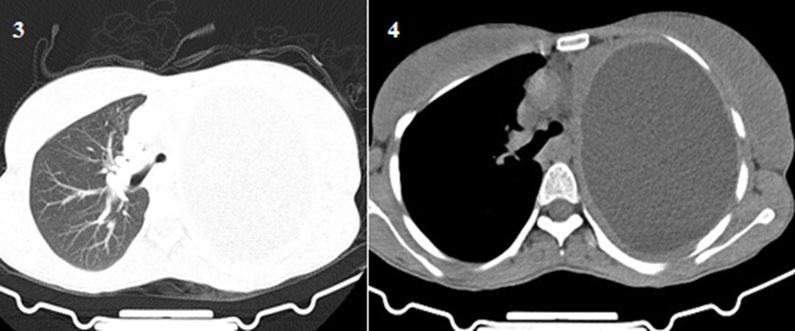
Figure 3: shows a CT scan with a substantial cystic lesion of the left lung, which compressed the heart and mediastinum in the parenchymal window.
Figure 4: shows a CT scan with a substantial cystic lesion of the left lung, which compressed the heart, mediastinum, and carina.
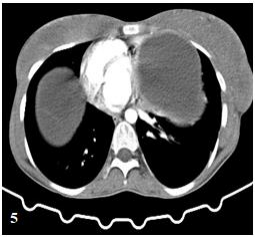
Figure 5: shows a CT scan with a substantial cystic lesion of the left lung, which compressed the heart mediastinum and carina.
The patient's ECG showed normal sinus rhythm, and her myocardial-specific enzyme levels were within the normal range. A cystic lesion was found to be causing pressure on the left ventricle and atrium on the lateral wall of the pericardium, as revealed by CXR and CT scans. Abdominal ultrasonography and contrast-enhanced CT scans confirmed the presence of a large hydatid cyst lesion with septation in the liver (Figure 6,7,8).
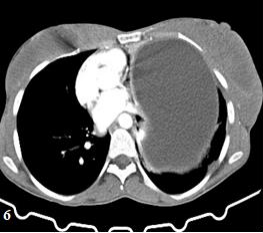
Figure 6: shows a CT scan with a substantial cystic lesion of the left lung, which compressed the heart and mediastinum, carina, and liver cyst.
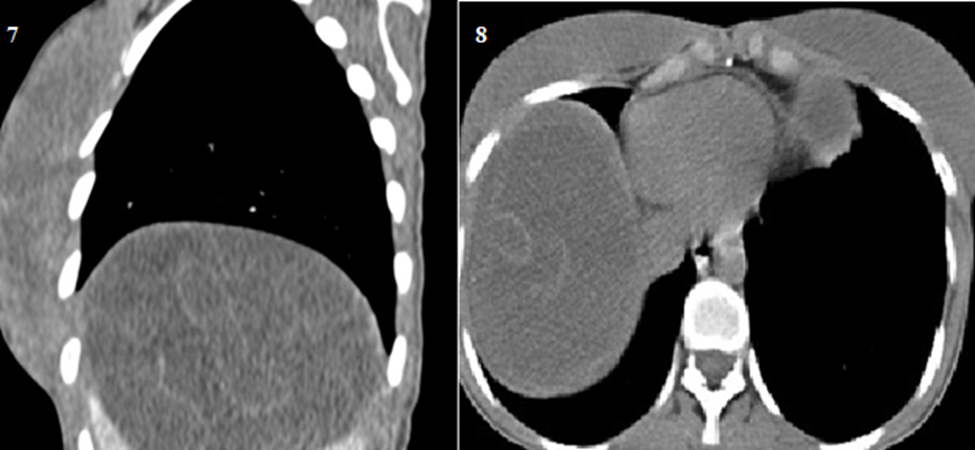
Figure 7: shows a coronal CT scan of the liver with huge cystic, septation, and laminated membrane.
Figure 8: shows a CT scan of the liver with huge cysts, septation, and a laminated membrane in another view.
The patient tested negative for hydatidosis but had marked eosinophilia (30%). Surgery was scheduled to address lung and liver hydatid cysts in a single stage. The patient underwent general anaesthesia and one-lung ventilation. A solitary cystic lesion adhered to the pericardium adjacent to the left ventricle and atrium (15 to 10 cm) was removed via left antero-lateral thoracotomy and treated with hypertonic saline and aspiration (Fig 6,7).
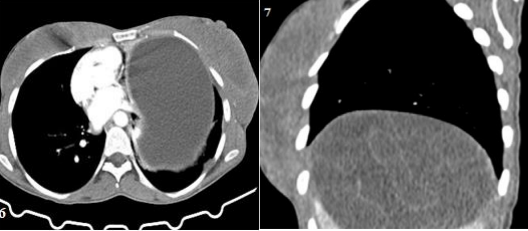
Figure 6: shows a CT scan with a substantial cystic lesion of the left lung, which compressed the heart and mediastinum, carina, and liver cyst.
Figure 7: shows a coronal CT scan of the liver with huge cystic, septation, and laminated membrane.
After approaching the liver cyst near the left chest wall, an anterolateral thoracotomy was performed in the seventh intercostal space. The cyst was aspirated and evacuated, and the cavity was closed using omentum and capitonnage. Following the operation, thousands of daughter cysts and a laminated membrane were found (Figure 9,10,11).
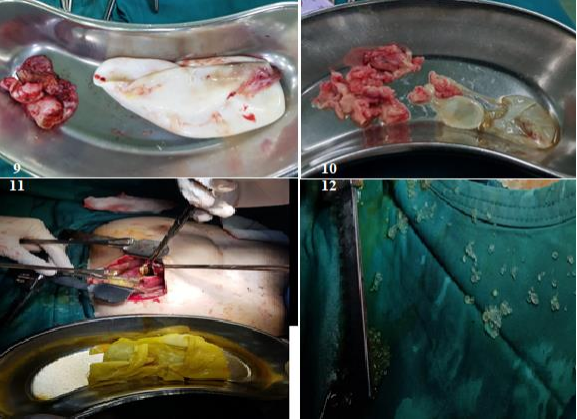
Figure: 9,10,11,12 show elements of hydatid cyst herniotomy and daughter cysts.
The diaphragm was repaired after the chest tube insertion. The patient was extubated in the operating room and was discharged five days after the operation, in good condition and taking 800 mg of albendazole for three months. The patient's condition remained good during the one-month follow-up.
Hydatid disease is a parasitic infection prevalent in the Mediterranean, Far East, South America, and the Middle East, including Iran [1-3]. Concomitant pulmonary and hepatic hydatid cysts are found in 4% to 25% of echinococcosis patients [2, 3]. Pulmonary hydatid cysts are more common in younger individuals. Around 30% of people with these cysts have multiples, and only 4% have cysts in both lungs. Of 216 surgically treated cases, 18 individuals had cysts in both lungs, accounting for 8.33% of the cases [4, 6-8]. It may be found during routine clinical examination and serologic, radiographic, or ultrasonographic screening[4, 5]. The clinical signs and symptoms of hydatid cysts depend on the location and size of the cysts, as well as their proximity to other organs. Complications may arise from infection or rupture of the cysts, which can occur in several areas such as peritoneal, intrabiliary, pleural, lung parenchymal, and rarely, intrapericardial cavity, leading to potential heart compression and tamponade [1, 3, 4]. Secondary bacterial infection of the hepatic hydatid cyst occurs when the rupture of both pericyst and endocyst and bacteria can enter the cyst (10). The presence of an air-fluid level inside the cyst on CT scans may indicate infection. The patient's condition and imaging results will determine the final diagnosis. Cyst rupture can occur in various body cavities due to trauma, pressure increase, or Albendazole treatment. A ruptured hydatid cyst in the peritoneal cavity may cause symptoms like abdominal pain, urticaria, anaphylaxis, sudden death, or shoulder pain due to diaphragm irritation. However, in our case, the main complaint was only abdominal pain [3-6]. Complications of pulmonary hydatid cysts include rupture, secondary infection, hydropneumothorax, and suppuration. Heart compression is rare. Symptoms after cyst rupture may consist of sudden chest pain, cough, fever, hemoptysis, and urticarial wheezing and anaphylaxis. Other symptoms include cough, chest pain, breathlessness, expectoration, and anaphylactic pneumonia. Infection can make it difficult to differentiate from an abscess or neoplasm of the lung [1-3]. Our patient is experiencing shortness of breath, progressive dyspnea, palpitations, dyspnea on exertion, and JVP engorgement. We used CXR and CT scans for the lung hydatid cyst and abdominal ultrasound, CT, MRCP, and ERCP for liver hydatid cysts to diagnose thoracic hydatid cysts [2, 4]. Indications for surgery may include large, superficial cysts at risk of rupture, infected cysts, cysts in important anatomical locations, and significant mass effects [6-8]. In the event of intrapleural or intraparenchymal rupture, thoracotomy and laparotomy are required for evacuation, omentoplasty, capitonnage, decortication, and pericardiotomy [1, 3]. In our case, During the surgery, the patient underwent a one-stage bilateral anterior-lateral thoracotomy. A cystic lesion adhering to the pericardium adjacent to the left ventricle and atrium was drained and secured with capitonnage. A liver cyst was also drained and filled with omentum, and the diaphragm was repaired. The patient was discharged in good condition five days post-surgery and prescribed 800mg of albendazole for three months. In the following month, the patient's condition continued to improve.
In areas where a disease is commonly found, both lung and liver hydatid cysts can co-occur. The heart may become compressed, potentially leading to tamponade. For young patients, surgery should be carried out using a one-stage procedure.
M A, R P, O M R, A A F: case curation, methodology, original draft, writing-review & editing. A F, A A F, ZS, SA: data curation, investigation. MF: conceptualisation, investigation, project administration, supervision, writing-original draft, writing-review & editing. All authors read and approved the final manuscript. All authors take responsibility for their contributions as outlined above, and they have read and approved the final manuscript.
There are no sources of funding for this case report.
Availability of data and materials:
All data and materials are provided in the manuscript. Data sets used and analyzed during the current study are available to the corresponding author upon reasonable request.
Ethical approval and consent to participate:
The study was performed following the declaration of Helsinki and approved by the Ethics Committee of Guilan by the Local Ethical Committee of Arya Private Hospital. Iran, Rasht, Guilan, Tel=+981333759790-9 E-mail =info@Aryahospital.ir
Written informed consent was obtained from the patient to publish this case report and any accompanying images
The authors declare no competing interests.
The authors would like to thank the Razi Clinical Research Development Unit.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
