
Case Report | DOI: https://doi.org/10.31579/2690-1919/203
1 MDS. Reader. Department of Oral and Maxillofacial Surgery, People Dental Academy, Bhopal.
2 MDS. Professor and Head. Department of Oral and Maxillofacial Surgery, People Dental Academy, Bhopal.
3 MDS. Senior Lecturer. Department of Oral and Maxillofacial Surgery, People Dental Academy, Bhopal.
4 Post Graduate Student. Department of Oral and Maxillofacial Surgery, People Dental Academy, Bhopal.
5 MDS. Consultant. Private Practioner. Bhopal
6 MDS. Reader. Department of Oral Medicine and Radiology, Rishiraj College of Dental Science and Research Center. Bhopal.
*Corresponding Author: Neha Jain, Room No 101, Department of Oral & Maxillofacial Surgery, People’s Dental Academy, Bhopal.
Citation: Neha Jain, Ajay Pillai, Amirthaa Varshini, Dhwani Kawadkar, Kriti Dubey and Ajita Singh (2021). Odontome- Revisted. J Clinical Research and Reports, 9(2); DOI:10.31579/2690-1919/203
Copyright: © 2021 Neha Jain. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 29 September 2021 | Accepted: 15 October 2021 | Published: 26 October 2021
Keywords: odontome; odontoma; complex odontoma; compound odontoma; odontogenic tumour; hamartoma; enucleation
Odontomas are benign odontogenic tumors subdivided morphologically into complex or compound odontomas. This paper describes the case of a complex odontoma in a 31-year-old male who complained of a painless swelling in right mandibular region which was diagnosed radiographically as complex odontome. Surgical enucleation of the lesion was done and sent for histopathological examination.
The term odontoma was coined firstly by Pierre Paul Broca in 1867, who described it as tumours formed by the disproportionate transitory or full growth of dental tissues [1]. Odontomes are the most common benign odontogenic tumours of epithelial and mesenchymal origin accounting for 22% of the odontogenic tumors [2]. Odontomes are usually seen on radiograph as a small, solitary, or multiple radiopaque lesions which may because delayed eruption of teeth, retention of primary teeth or displacement of teeth [3]. According to radiographic, microscopic, and clinical features, two types of odontomas are recognized: Complex and compound odontomas. Compound odontoma forms a conglomeration of small structures resembling teeth, whereas a complex odontoma forms an irregular mass in a disorderly pattern [4].
Odontomas are discovered during the second and third decades of life [5]. The compound odontoma is slightly more common than the complex odontoma. The majority of odontomas seen in the anterior region of the jaws are compound in nature (61%), whereas the majority observed in the posterior region is complex in nature (34%) [6]. The compound odontome most frequently occurred in incisor cuspid region of the maxilla in contrast to the complex odontome which were commonly found in molar and premolar region of the mandible [7]. They are observed more in right side of the jaws (compound 62%, complex 68%) [6].
Feature | Compound Odontome | Complex odontome |
Definition | Malformation in which all dental tissues are arranged in a more orderly pattern than in the complex odontoma so that the lesion consists of many tooth-like structures | Malformation in which all dental tissues are arranged in a hapazard manner. |
Shape | Regularly shaped, solitary or multiple small denticles or tooth like structures | Amorphous conglomeration of dental tissues |
Appearance | Bizzare peg shaped teeth show anatomic resemblance to normal teeth | An irregular mass with no morphologic similarity. |
Incidence | 9 to 37% | 5 to 30% |
Sex | Female predilection is seen | |
Age | Commonly seen in second and third decades. Both the type of odontomas are seen in younger individual with mean ages 14.8 and 20.3 years respectively. | |
Site | Commonly situated in the anterior region of maxilla | Posterior region of mandible |
Side and dentition | Both type of odontomas occurred more frequently on the right side of the jaw than on the left. Commonly occur in permanent dentition and are rarely seen in primary dentition | |
Sign and symptoms | Asymptomatic, although occasionally signs and symptoms relating to their presence do occur symptoms • These generally consist of – Unerupted or impacted teeth, retained deciduous teeth, swelling, evidence of infection and displacement of teeth and malocclusion. • Compound odontome rarely cause expansion of bone but in complex odontome marked bony expansion has been observed. | |
Radiological feature | Comparatively well-organized malformed teeth or tooth-like structures or denticles of varying size and shape surrounded by a narrow radiolucent zone | Irregular mass of calcified material surrounded by a narrow radiolucent band with smooth outer periphery |
Histopathology | Tooth-like structures with central cores of pulp tissue that are encased in shells of dentin and partially covered by enamel, surrounded by a fibrous capsule similar to the follicle surrounding a normal tooth. | Microscopically they consist of haphazard conglomerates of dentin enamel matrix, enamel, cementum and pulp tissue. |
Treatment | Surgical enucleation | |
Table 1: Difference between compound odontoma and complex odontoma [8]
A 31year old male patient reported to the outpatient department of Oral and Maxillofacial surgery, People’s Dental Academy, Bhopal with a complaint of painless swelling in the lower right back tooth region from last 5-6 months. Initially the swelling was pinhead sized which has progressively increased over a period of 6 month to attain present size.
On examination, no facial asymmetery was noted extraorally. On intraoral examination single, well defined, oval, non tender swelling of 4*3 cm was present in buccal vestibule extending from 45 to 47 obliterating the buccal vestibule (figure 1). The swelling also seen in lingual vestibule in 46 and 47 region (figure 2). The color of the swelling was normal as that of mucosa. On palpation the swelling was smooth and firm hard in consistency. No evidence of crepitus or pathological fracture was seen. Hard tissue examination revealed buccal pits restored with amalgam restoration in relation to 46 and 47. The tooth 46 was found to be tender on percussion.


A provisional diagnosis of periapical cyst was made.
OPG revealed an ill-defined radiopacity present in relation to the apex of 46. The radiopaque mass was encased by a well -defined radiolucent borders suggestive of the lesion being well localized and well circumscribed. (Figure 3)

Upon corelating the clinical and radiographical findings the diagnosis of complex odontoma was made.
Excisional biopsy was planned under GA. Root canal treatment was done for 47 and 45 prior to the surgery. All the pre-liminary investigations including Total blood count, serology, BT, CT, blood group, LFT, KFT, serum electrolytes, Chest X-ray and ECG were performed.
Following all the aseptic measures before the surgery, trapezoidal incision was given extending from 43 to 48 region. Releasing incision was placed in the canine and 3rd molar region and mucoperiosteal flap was raised to visualize the area completely. 46 was extracted then bone was removed buccally till we reached the lesion (Figure 4).

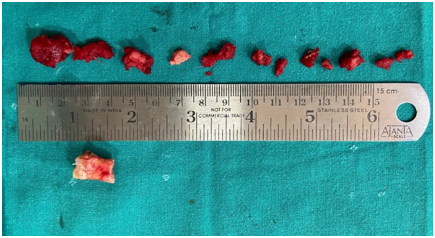
The bony mass was sectioned and delivered in parts and sent for histopathological evaluation (Figure 5).
Curettage was done and the bony cavity was packed with PRF to accelerate healing. The flap was then approximated with resorbable 3-0 vicryl sutures. (Figure 6)

Post-operative medications to control pain, post-operative edema and infection were prescribed. Mouthwash was advised to maintain oral hygiene. Patient was recalled after 7 days for suture removal and post op OPG was done. (Figure 7).

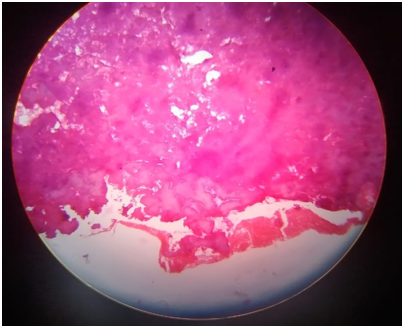
On histopathological examination of the excised lesion the diagnosis of odontoma was confirmed. (Figure 8)
Odontoma are benign odontogenic tumor composed of enamel, dentine, cementum and pulpal tissue.
Etiology of odontoma [9]
1. Trauma to the primary dentition
2. Infection from deciduous predecessor
3. Genetically inherited
4. Associated with anomalies like Hermann’s and Gardner’s syndrome
5. Hyperactivity of the ameloblast, cell rest of serres, dental lamina remnants
6. Genetic mutation causing aberrations in signaling pathways controlling tooth development.
Classification
Several Classification has been given to odontome
A) In 1914, Gabell, James, and Payne grouped odontome according to their developmental origin: [10]
B) In 1946, Thoma and Goldman proposed a classification which is as follows: [11]
C) According to the World Health Organization (WHO) classification, odontomes can be divided into three groups: [12]
1. Complex odontome: In this type the calcified dental tissues are arranged in a haphazard manner which morphologically does not resemble to rudimentary teeth.
2. Compound odontome: composed of odontogenic tissues which are arranged in an orderly pattern, which result in many teeth-like structures, but without morphological resemblance to normal teeth.
3. Ameloblastic fibro-odontome: In this subtype varying amounts of calcified dental tissue and dental papilla-like tissue, resembling an ameloblastic fibroma is seen. This type has been considered as an immature precursor of complex odontoma.
D) On the basis of radiographical representation and microscopic features two types of odontoma are seen, namely: [13]
E) According to their position within the jaws: [13]
Extraosseous or peripheral odontomas: These are odontomas occurring in the soft tissue covering the tooth bearing portions of the jaws, having a tendency to exfoliate.
Usually the odontoma are asymptomatic, discovered routinely during radiographs. Occasionally signs and symptoms do exist which may be observed in the form of unerupted or impacted teeth, retained deciduous teeth, swelling, infection, displacement or devitalization of tooth. Compound odontomas rarely cause bony expansion but complex odontomes may lead to marked bony expansion [8].
Since odontoma are usually intraosseous type so they diagnosed only by radiograph. Extraosseous form can be manually palpated. But the distinguishable type can only be diagnosed on radiograph. The radiographic appearance of complex and compound odontoma is mentioned in (table 1).
Treatment
Surgical excision or enucleation of the odontoma is the treatment of choice. Since odontoma are benign encapsulated odontogenic tumors which have little propensity to grow and reoccur but as mentioned earlier it can cause bony expansion, cystic changes, interruption of tooth movement, etc. so surgical removal is necessary.
Early diagnosis and treatment of odontomas led to better prognosis, cost effective and prevent relapse and devitalization and displacement of tooth.
Odontomas rarely erupt into the oral cavity and tend to be associated with impacted, erupted as well as retained teeth. They are diagnosed on a thorough visual and radiographic examination. Compound odontoma on radiograph shows tooth like structures whereas compound odontoma presented as irregular calcific mass. The enucleation of the odontoma and extraction of the associated tooth along with root canal treatment for both the adjacent teeth is done for best outcomes.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
