
Case Report | DOI: https://doi.org/10.31579/2641-0419/479
Department of cardiology, MM Institute of Medical Sciences and Research, Mullana, Ambala (India).
*Corresponding Author: Rajeev Bhardwaj, Department of cardiology, MM Institute of Medical Sciences and Research, Mullana, Ambala (India).
Citation: Rajeev Bhardwaj, Rajesh Nandal, Tania Pruthi, Saurav Mittal, Subeg Singh, et al, (2025), Nutcraker Syndrome Managed by Endovascular Approach, J Clinical Cardiology and Cardiovascular Interventions, 8(8); DOI: 10.31579/2641-0419/479
Copyright: © 2025, Rajeev Bhardwaj. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 May 2025 | Accepted: 27 May 2025 | Published: 06 June 2025
Keywords: nutcracker; hematuria; stent
Nutcracker syndrome is a clinical syndrome, presenting with various symptoms caused by compression of left renal vein, between aorta and superior mesenteric artery, due to narrow angle between these vessels. Patient may present with abdominal pain, hematuria, or symptoms of urinary tract infection. We present a case of Nutcracker syndrome presenting with chronic abdominal pain, managed by percutaneous intervention.
44 years female, presented with pain in abdomen for the last one and half years. Pain was present in left lumber region and left iliac fossa and radiated to back. Pain initially was mild in intensity, but for the last 6 months, it was moderate in intensity and increased after meals and was aggravated during menstruation. Patient took treatment in various hospitals, without any relief. Patient also gave history of intermittent hematuria and also intermittent burning micturition. 3 months back, her ultrasound was done in some outside hospital, which reported mildly dilated venous channels seen in the region of left renal vein-possibility of compression of left renal vein was kept.
CECT of abdomen was done in same hospital which reported- Grossly dilated venous channels are seen in the pelvic cavity-likely pelvic congestion, with maximum diameter of venous channels approximately 12 mm. Left ovarion vein is dilated with opacification of left ovarian vein in corticomedullary phase from left renal vein and measures up to 11 mm in diameter. There is abrupt narrowing of left renal vein as it courses posterior to SMA due to compression between aorta and SMA with approx. 90% luminal narrowing. SMA and aorta angle is approximately 5 degrees. With space between Aorta and SMA at the level of left renal vein is approx. 3.3 mm.- likely anatomical variant/ nutcracker syndrome.
Blood investigations:
Hemoglobin-11.3 gm%
TLC-7.7x1000/cumm
Polys-65%
Platelet count-99x1000/cumm
ESR-15 mm in 1st hour.
Urea-21.8 mg/dl
Creatinine-0.49mg/dl
Keeping in view the possibility of Nutcracker syndrome (NKS). patient was taken up for percutaneous treatment. Right femoral vein puncture was done. Femoral vein angiography was done to see inferior vena cava (IVC), (Fig.1) to have idea of origin of left renal vein. Femoral artery access was also taken and left renal arteriography was done to trace renal vein in venous phase, but it could not be visualised. Since renal vein was not visualised, blind entry was done with terumo wire passed through right Judkins (JR)catheter. Catheter was then negotiated into LRV and venography was done (Fig. 2). It showed markedly dilated left gonadal vein (LGV), and left ovarion vein (Fig 3). Hardly any contrast was entering into IVC, due to compression by superior mesenteric artery (SMA). It was decided to put a stent in LRV across the compressed segment. To properly define the site of obstruction and stent placement, a JR catheter was placed in SMA (Fig 4), from left brachial artery approach. Self-expanding venous stent was then deployed, size 14x 60 mm. (Fig 5). LRV angio was then done which showed free flow of contrast into IVC and minimal reflux into LGV (Fig. 6). If, large reflux persisted, then coiling of LGV would have been required.
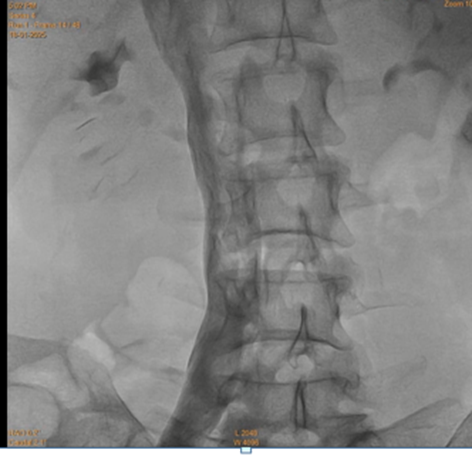
Figure 1: Inferior veno-cavography

Figure 2: Left renal venography shows hugely dialted gonadal vein, with very little flow into inferior vena cava (Due to renal vein compression and reflux of blood into gonadal vein)

Figure 3: Marked dilatation of left ovarian vein, due to reflux from gonadal vein.
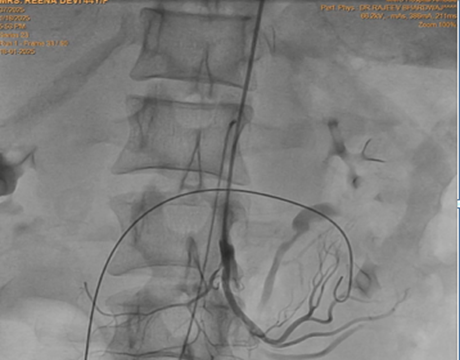
Figure 4: Catheter in superior mesenteric vein, from left brachial artery approach, as marker to guide the position of stent.
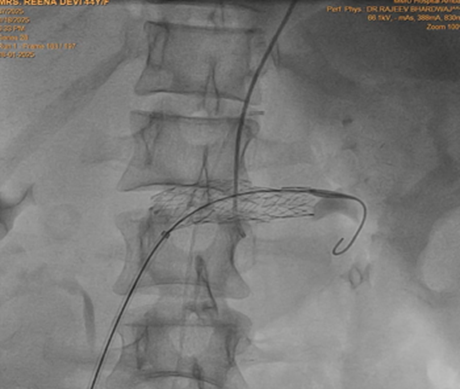
Figure 5: Self expanding stent placed in left renal vein across the superior mesenteric artery crossing.

Figure 6: Left renal venography shows free flow into inferior vena vava, with hardly any reflux into gonadal vein.
NKS is a rare condition caused by compression of LRV between aorta and SMA [1]. Patient has non-specific symptoms and so condition remains undiagnosed for long time. Symptoms include flank pain, intermittent hematuria, orthostatic proteinuria and autonomic dysfunction [2]. Women may present with pelvic congestion syndrome, dysmenorrhoea or dyspareunia. Men may present with left sided varicocele. NKS may cause infertility in both sexes. NKS refers when anatomy concides with symptoms, while asymptmatic persons with anatomy are labelled as nutcracker phenomenon.
There are 2 varieties of NKS:
NKS occurs when angle between aorta and SMA is reduced to less than 40degree. Normal 4-5 mm space between the vessels is maintained by retroperitoneal adipose tissue and 3rd part of duodenum. So, thinner individuals are more affected. In some cases, relief of symptoms have been reported with weight gain [3].
Management: Initial management, especially in children should be conservative, as there are chances of spontaneous relief with weight gain. Around 75% of all children with NKS will have complete resolution of symptoms within two years [4].
Surgical treatment is recommended in patients with severe hematuria, severe proteinuria, varicocele, renal failure and severe pain. Endovascular stenting was first described as therapy for NKS in 1996 and results are good [8,9]. 6-8 Cm long stent with diameter of 12-14mm is placed near the first division of left renal vein to prevent stent migration. If significant reflux persists into the LGV after stent placement, then embolization of LGV may be required. Stent migration, erosion into adjacent structures, and kinking are the most common complications of endovascular procedures.
Our patient remained undiagnosed for one and half years, she was lucky to have been subjected to CT from outside, after suspicion on ultrasound. We implanted a long stent. Patient became symptom free within 3 days and is doing well. She will be subjected to ultrasound after 3 months and then annually for 3 years.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
