
Case Report | DOI: https://doi.org/10.31579/2690-4861/132
1 Department of Medical Oncology, Nizam’s Institute of Medical Sciences, Hyderabad, Telangana.
*Corresponding Author: Krishnamani Kalpathi, Department of Medical Oncology, Nizam’s Institute of Medical Sciences, Hyderabad, Telangana.
Citation: K Krishnamani. (2021) Non Hodgkin Lymphoma Presenting As a Pancreatic Mass- Treated Sucessfully with R-Chop. International Journal of Clinical Case Reports and Reviews. 7(3); DOI: 10.31579/2690-4861/132
Copyright: © 2021 Krishnamani Kalpathi, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 24 April 2021 | Accepted: 01 July 2021 | Published: 05 July 2021
Keywords: non hodgkins lymphoma; pancreas; dlbl
Primary pancreatic lymphomas are extremely rare, when present mimics symptoms of adenocarcinoma of the pancreatic head. They account for less than 1% of pancreatic neoplasms. The most common histological subtype is diffuse large B cell lymphoma (DLBCL). Herein, we present a case of a 47-year-old female who presented with symptoms of pain abdomen and weight loss. CT (Computerized Tomography) was suggestive of a lesion in the pancreatic head which on histopathology was diagnosed as a primary non-Hodgkin’s lymphoma confirmed by immunohistochemistry.
The gastrointestinal region is the commonest site of extra nodal NHL followed by skin. Gastrointestinal non-Hodgkin lymphoma commonly involves the stomach and the small bowel. It rarely presents as a pancreatic mass accounting for less than 1% [1, 2]. It tends to have a male predominance (male-to-female ratio of 7:1) with age ranging from 35 to 75 years (mean age: 55 years) [4]. Primary Pancreatic Lymphomas (PPLs) are potentially treatable [5]. Majority of patients can be managed with chemotherapy and the prognosis is much better compared to patients with pancreatic adenocarcinoma which has a dismal outcome [5].
A 47 year old lady without any co morbidities presented with pain abdomen, dyspepsia and 8 kilogram weight loss of 3 months duration. She did not report any symptoms of fever, night sweats, pruritis, chest symptoms, and bowel and bladder disturbances. Clinical examination was unremarkable but for mild pallor. There was no lymphadenopathy and organomegaly. She was hemodynamically stable. Initial imaging done elsewhere with Computerised Tomography (CT) of abdomen was suggestive of a 34 x 57 x 66 mm pancreatic head lesion, with loss of fat planes with stomach. Also noted was lymphadenopathy involving peripancreatic, periportal and portocaval regions. CA 19.9 was normal (0.760 units/ml). Complete blood picture, renal, liver function tests and LDH was normal. Viral markers were negative. An endoscopic ultrasound (EUS) was suggestive of gastric antral ulcer and a pancreatic body and tail mass. EUS guided fine needle aspiration cytology (FNAC) was done which suggested a poorly differentiated neoplasm. Immunohistochemistry (IHC) was done to further characterize the lesion which showed positivity for LCA, CD 20, BCL2, BCL6, CD 45 and CD 10 with KI-67 of 50%. The lesion was negative for Pan CK, Chromogranin and CA 19.9 leading to a diagnosis of B cell NHL (non-Hodgkin’s lymphoma). Fluorescence in situ Hybridisation (FISH) done for BCL-2, BCL-6 and c-myc expression and rearrangement were negative ruling out a possibility of double hit lymphoma.
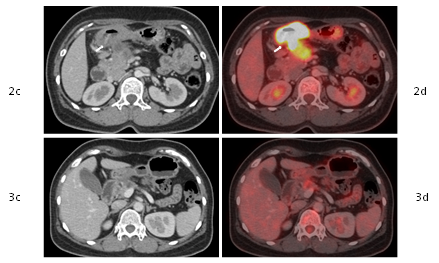
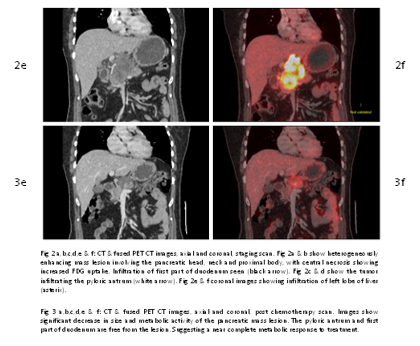
PET CT (Positron Emission Tomography Computerised Tomography) scan was done for baseline staging. PET CT was suggestive of a metabolically active locally advanced primary pancreatic head lesion infiltrating the pyloric antrum with adjacent peripancreatic nodes. Also seen were metabolically active Index score was 2 which is low intermediate. A diagnosis of Stage III BE Non-Hodgkin’s lymphoma was made. Considering the prognosis and available options for treatment, she was offered R- CHOP (Rituximab-Cyclophosphamide, Doxorubicin, Vincristine and prednisolone) based chemotherapy. After three cycles,an interim PET-CT done suggested a complete metabolic response. She received a total of six cycles and continues to be in remission.


Gastrointestinal lymphomas constitute 10-15% of all non-Hodgkin lymphomas and 30-40% of all extranodal lymphomas with Gastrointestinal non-Hodgkin lymphoma (NHL) usually involving the stomach and the small bowel. PPLs are rare. Most cases of pancreatic non-Hodgkin lymphoma usually present as a disseminated disease [1]. The most common histologic type of the pancreatic lymphoma is diffuse large B-cell lymphoma [1]. Accounting for 77% to 80% of all patients [3]. PPL are also known to present as follicular lymphoma, small lymphocytic lymphoma, Burkitt’s lymphoma, and rarely as a T cell lymphoma [3]. The clinical presentation of primary pancreatic lymphoma is nonspecific, varying from abdominal pain which is most common presenting symptom , followed by abdominal mass , weight loss, jaundice , acute pancreatitis, small bowel obstruction and diarrhea .The classic symptoms of nodal non-Hodgkin's lymphoma, such as fever, chills and night sweats are uncommon [4].
Diagnostic criteria for PPL, as described by Dawson et al. Behrns include (a) mass predominantly located in the pancreas with lymph nodes confined to the peri pancreatic region. (b) neither superficial lymphadenopathy nor enlargement of mediastinal lymph nodes on chest radiography (c) a normal leukocyte count in peripheral blood, and (d) no liver or splenic involvement [4]. These days however CT chest abdomen and/or PET-CT are standard baseline imaging tests, with higher sensitivity to pick up occult or small volume disease in the mediastinum and other sites, as illustrated in our case too.CA 19-9, Lactate dehydrogenase (LDH) and beta-2-microglobulin are essential serum markers for the diagnosis and differential diagnosis of PPL and for differentiating from pancreatic adenocarcinoma [4]. CA 19.9 tends to be raised in adenocarcinoma, while raised LDH would be more in favour of a lymphoma. Imaging studies tend to show a bulky localized tumor in the pancreatic head without significant dilatation of the main pancreatic duct, infrahilar retroperitoneal enlarged lymph nodes and invasive tumor growth not respecting anatomic boundaries with infiltration of surrounding structures. Also the presence of necrosis and calcification is unlikely in NHL [5]. However, the definitive diagnosis of PPL is based on the histopathological and cytopathological examinations [3, 5]. For a definitive diagnosis, CT, or ultrasound-guided fine needle aspiration biopsy is the optimal approach, as it is highly accurate [5]. Pathological evidence is useful not only for the diagnosis, but also for the classification of lymphomas which is mandatory for the choice of chemotherapeutic regimen [6].
Although morphologically different, these two lesions can still diagnosed using IHC which prove to be confirmatory in cases of ambiguity. In patients with aggressive lymphomas FDG-PET is done at baseline for staging, for interim evaluation and to assess response to therapy. It has shown to be a useful prognostic tool to predict relapse risk after the chemotherapy. Poorer clinical outcomes were seen in patients with positive FDG-PET scans as compared to patients with negative scans [6].
Total pancreatectomy (Whipple procedure), which is standard of care for resectable pancreatic adenocarcinomas is considered to have no impact on survival in PPL and, because of associated morbidity, is not generally recommended for diagnosis and treatment of PPL [4,7]. Thus PPL are treated on similar lines to NHL at other sites.
The poly-chemotherapy with R- CHOP represents the standard chemotherapy regimen for DLBL treatment with a complete response in 45-53% of cases and long-term survival of 30-37% [6]. The role of radiation therapy in PPL remains poorly defined [8].
Bouvet and colleagues have reported use of adjuvant radiation to decrease local failures [9]. Earlier Studies have shown some evidence that an initial surgical resection, when coupled with chemotherapy and radiotherapy, was associated with increased long-term survival of PPL [7], but R-CHOP remains standard for extranodal lymphomas. Prognosis of PPL is significantly better than pancreatic adenocarcinoma, with cure rates of up to 30% in earlier series compared to less than 5 % 5 year survivals for the latter [10, 11, 12].
To conclude, PPLs are a class of rare cancers afecting the pancreas, of which DLBL is usually the common variant. However, as efficacious treatments exist for this entity and differ markedly from that of pancreatic adenocarcinom, it is very important that PPLs should be included in the differential when evaluating a probable pancreatic neoplasm.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
