
Research Article | DOI: https://doi.org/10.31579/2578-8965/123
1 Consultant OBS and Gynae, Khemchand Jain Hospital, Sagar, MP, India.
2 Statistician cum lecturer, department of community medicine, Bundelkhand Medical College Sagar, MP, India.
3 Consultant Surgeon, Dept. of Surgery, Om Surgical Center & Maternity Home, Varanasi, UP, India.
*Corresponding Author: Ruby Reja. Consultant Khemchand Jain Hospital Sagar, MP, India.
Citation: Ruby Reja, Sandhya Singh, Pankaj Srivastava. (2022). Non-Descent Vaginal
Hysterectomy (Ndvh): A Promising Surgical Technique in Benign Uterine Disorders, J. Obstetrics Gynecology and Reproductive Sciences, 6(4) DOI: 10.31579/2578-8965/123
Copyright: © 2022 Ruby Reja. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 May 2022 | Accepted: 24 May 2022 | Published: 30 June 2022
Keywords: abdominal hysterectomy; intra operative complications; Salpingooophorectomy; Non descent vaginal hysterectomy
Background: Hysterectomy, one of the most common gynaecological surgeries performed around the world, has many techniques including abdominal, vaginal, laparoscopic and robotic. The Vaginal technique which was introduced and performed eras back has been less successful due to lack of experience and eagerness among gynaecologists because of a misconception that the abdominal route is safer and is easier.
Aims and Objectives: Evaluation of most efficient and suitable route of hysterectomy.comparison between intraoperative and postoperative complications in non descent vaginal hysterectomy and abdominal hysterectomy.
Materials and Methods: This retrospective study was conducted during the period from October 2020 to December 2021, it studied 60 women who underwent hysterectomy for benign uterine disorder at Khemchand Jain Hospital, Sagar, out of which 30 women underwent non descent vaginal hysterectomy and 30 women underwent total abdominal hysterectomy.
Result: Baseline characteristics were similar between the two groups with no intraoperative complications in either. Regarding operation duration, intraoperative blood loss, post-operative pain, post-operative blood transfusion, mobilization in post-operative periods, post-operative wounds infection, febrile morbidity, duration of hospitality stay, P-value was significant in vaginal hysterectomy when compared to abdominal hysterectomy. Regarding post-operative systematic infection, P-value was not significant. None of the cases in the vaginal group were converted to abdominal route and none of the cases in the whole study group underwent relaparotomy.
Conclusion:
The study concludes that patients requiring hysterectomy for benign non prolapse cases may be given the option of vaginal hysterectomy because it has quicker recovery, shorter hospitalization, lesser operative and post-operative morbidity compared to abdominal route.
After caesarean section, hysterectomy is the most common surgical procedure in obstetrics and gynaecology [1,2]. The comfort and convenience in large abdominal incision have led to the predominance of abdominal hysterectomy over the vaginal route [3]. Emphasis on minimaly invasive surgery today has led to revival of interest and importance of vaginal hysterectomy (VH) for non-prolapsed indications, i.e., non-descent vaginal hysterectomy (NDVH). The popular beliefs that bulky uterus, pelvic inflammatory diseases, narrow vagina, prior Caesarean delivery [4] and enlarged uterus, make vaginal hysterectomy difficult are is not considered to be contraindication for non-descent vaginal hysterectomy, but it can be successfully attempted in all these conditions. Even in nulliparous women, when anaesthetized, there is sufficient uterine descent to make vaginal hysterectomy possible. Because the surgeon removes uterus through normal orifice/opening (vagina) in the body, it does not leave any visible scars. It is because of this reason that NDVH is referred to as a scarless hysterectomy or scarless surgery sometimes. The vagina is the ideal and most natural route to reach the uterus along with the presence of good anaesthesia, light, better suture material, electro surgical technique [5]. It is because of these reasons that the exploration of uterus through vaginal route is becoming highly approachable. Like any other surgery, hysterectomy is also a major operation and thus, we advise hysterectomy in conditions where medical and non-surgical treatments have not helped and only to women who have completed their family and do not wish to have more children. Every gynaecologist should be proficient in doing vaginal surgery and should believe that every uterus can be removed vaginally unless contraindicated. NDVH is better tolerated by elderly patients with medical diseases [6]. It has the clear advantage in obese women also [7,8]. However proper selection of patients is an important factor in deciding the success of vaginal procedure.
Material And Methods: It was a retrospective study conducted in Khemchand Jain Charitable Trust Hospital Sagar [M.P.] from October 2020 to December 2021. Patients in need of hysterectomy for benign diseases were included in this study. Data was collected from the case records of patients. 60 patients were included in the study and were divided into two groups. 30 patients (Group A) received non descent vaginal hysterectomy and 30 patients (Group B) received abdominal hysterectomy. All Preoperative criterias were fulfilled in these cases. Every patient was clinically evaluated and checked. After proper fitness and pre-anaesthesia checkup, patients were posted for hysterectomy.
The main criteria used for comparison were-
a) Intra operative blood loss
b) Operating time - For NDVH, it was calculated from incision at cervico-vaginal junction to the completion of closure of vault. Operating time for TAH was calculated from incision on the abdomen to closure of skin incision.
c) Intraoperative injury – Any injury to bowel, bladder or ureter was taken a note of.
d) Pain scoring as per the visual analog scale (VAS) was done on Day 3.
e) Post-operative ambulation.
f) Post-operative blood transfusion.
g) Post-operative complications like fever, pain, bladder, bowel disturbances, bleeding and wound infection.
h) Duration of post-operative hospital stay.
i) Conversion of vaginal to abdominal route.
j) Relaparotomy.
Statistical analysis was done and data collected in this study was presented in tabular form.
Inclusion criteria’s:
Exclusion criteria’s:
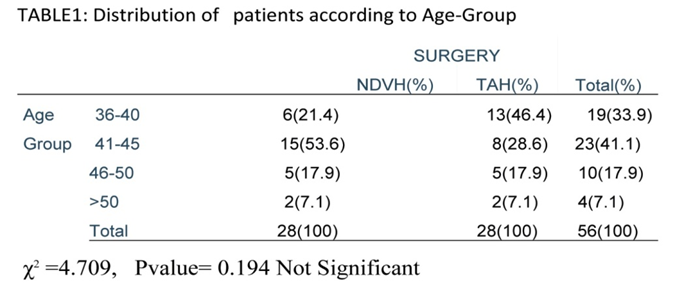
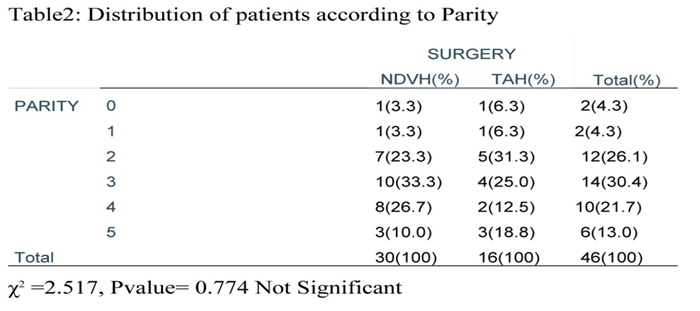
Total 60 patients were included in this study, 30 patient underwent non descent vaginal hysterectomy and 30 patients underwent abdominal hysterectomy. Baseline demographic characteristics were similar between both the groups [Table/Fig 1, 2].
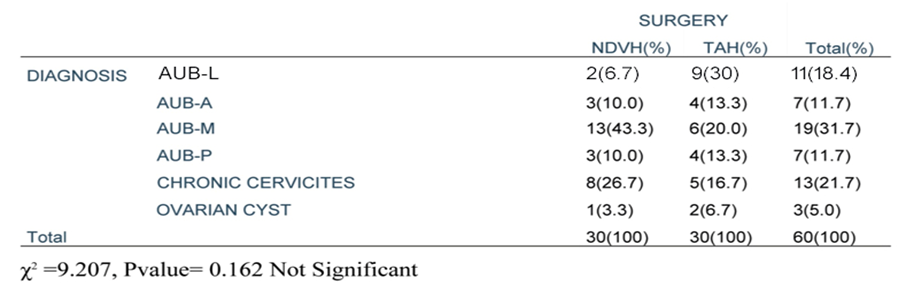
Gynecological problem diagnosed by history, examination and investigations as shown in [Table/Fig 3].
The problems in each group were comparable. In the vaginal group 14% patients had undergone Salpingoophorectomy along with hysterectomy as shown in [Table/Fig 4].

The mean operative time in NDVH group was 39.43 minutes while it was 77 minutes in abdominal group so p-value was highly significant p-value<.0001 as shown in [Table/Fig 5].

Intraoperative blood loss was significantly more in abdominal group as TAH requires entry via skin, abdominal fat, rectus and muscles as shown in [Table/Fig 6].

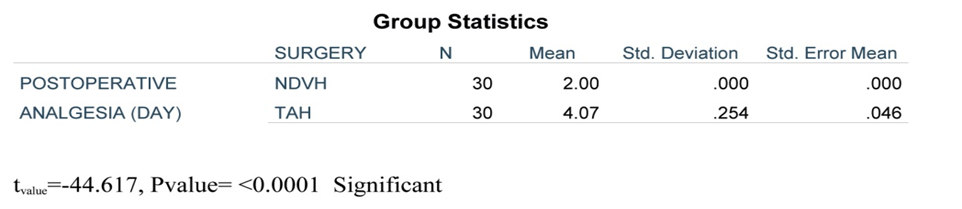
Post operatively more analgesia required in TAH group (4.07) compared with vaginal group (2), as measured by requirement of post operative analgesia as shown in [Table/Fig 7].
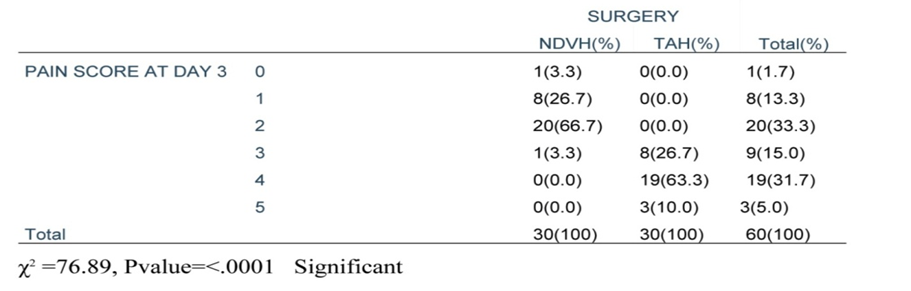
Pain Score on Day 3 of post operative periods was more in abdominal group as compared to vaginal group (p-value<.0001) as shown in [Table/Fig 8].
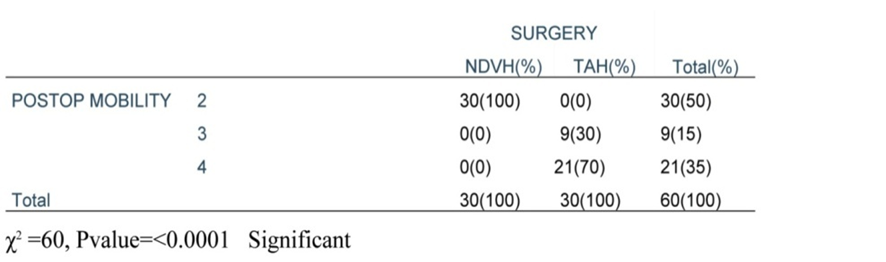
As post operative pain was less in NDVH group hence post operative mobilization and ambulation was earlier in NDVH group as compared to abdominal group (p-value<.0001) [Table/Fig 9].
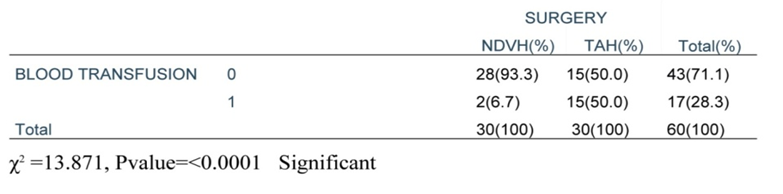
Post operatively only 2% NDVH cases required blood transfusion while need was clearly excess in TAH group (p-value<.0001) [Table/Fig 10].
No patient in NDVH group had wound infection while it was present in 40% (n=12) patient of abdominal group [Table/Fig 11].

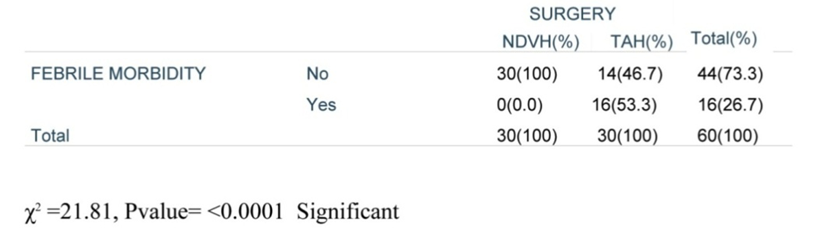
In NDVH group febrile mobidity was very less as compared to abdominal group 53.3% (n-=16) [Table/Fig 12].
P-value < .0001. The mean duration of hospital stay was 4 days in the abdominal group while in the vaginal group it was 2.30 days [Table/Fig13].

None of the cases in the vaginal group needed laparotomy and we did not encountered any intraoperative complication such as bladder, bowel or ureter injuries and none of the cases in both group required.
The uterus is the most important organ of female body so case selection for hysterectomy is of utmost importance. We should do hysterectomy only when conservative management fails and then deciding the route of hysterectomy is also important always. We should choose minimally invasive procedure. i.e. Non descent vaginal hysterectomy. The vaginal approach to hysterectomy has been the hallmark of the gynaecological surgeon. The motivation to acknowledge the advantages and explore the limits to the vaginal route came from patients who wished to avoid an abdominal incision [3]. Vagina is the best possible and most natural route to approach the uterus along with the availability of good anaesthesia, light, better suture material, electro surgical technique (ligasure vessel sealing system) [5], and it is because of these aforementioned reasons that the exploration of uterus through vaginal route is gaining popularity. Earlier, vaginal hysterectomy was usually done for uterine prolapse or inversion. As per tye medical historian Leonardo, vaginal hysterectomy was performed by Saronus in 2nd century on a gangrenous uterus[9]. In 1985, Garceau of France initiated vaginal hysterectomy for carcinoma of cervix, large fibroid, uteri prolapsed and infection. He became the first to introduce hemisection and morcellation of uterus to accompany vaginal removal. Most of the indications for vaginal hysterectomy in the past years was related to prolapse and abnormal uterine bleeding. Kovac felt that vaginal hysterectomy is the go-to treatment choice for management of patienta with non-malignant pelvic disease[10]. Usually, uterus > 12 weeks is considered as a contraindication, but a well-trained gynaecologist won’t accept it. While doing NDVH we had difficulty in delivery of uterus in patients of fibroid uterus it was accomplished with the help of enucleation of lecomyoma. According to sheth s [6] the preoperative sonographic estimation of uterine volume and the finding at examination under anaesthesia help in choosing the vaginal route. They needed debulking for uteri with a volume more than 300cm3[11], chandrashekhar etal used bisection in 12(16%) cases and morcellation in 2 cases (2.67%) [12]. In our study we used bisection in one cases (50%) and morcellation in other case (50%). Entire removal of uterus was done in all cases of TAH without using any debulking method. Magoc etal (9) removal large uteri weighing more than 1000gms vaginally [13], Aparna hedge etal[10], could successfully remove uteri size up to 16 weeks using these techniques[14]. D Kammerer deak and J Mao [12] concluded that use of uterine morcellation during vaginal hysterectomy is safe and it facilitates the removal of moderately enlarged and well supported uteri vaginally without increasing peri-operative morbidity [15]. Kumar et al., in a study performed on 80 women planned for NDVH, had a success rate of 95%. These patients were treated by vaginal hysterectomy and the operating time, laparotomy conversion rate and intraoperative blood loss were directly proportional to the size of the uterus [16]. The study concludeds that vaginal hysterectomy is a safe and effective process in uteri of less than 12 weeks size. Garg et al. performed a study to compare vaginal hysterectomy and abdominal hysterectomy with 23 patients in each group and found a reduced operating time, lesser intraoperative blood loss, reduced post-operative morbidity and shorter hospital stay in the vaginal hysterectomy group [17]. Mc Cracken et al found that intraoperative morbidity was less in vaginal hysterectomy when juxtaposed with abdominal hysterectomy and that vaginal hysterectomy should be the procedure of choice wherever possible [18]. Doucette and co-workers, in their study on 250 patients, challenged the common contraindications to vaginal hysterectomy including large uteri, nulliparas, previous CS or laparotomies and found that the aforementioned factors are rarely contraindications [19]. In a systematic Cochrane review of nine RCTs, it was concluded that NDVH should be performed whenever possible, taking into consideration the low rate of complications and cost-effectiveness.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
