
Research Article | DOI: https://doi.org/10.31579/2694-0248/013
*Corresponding Author: Francisco López Bustos,
Citation: Francisco López Bustos. (2021) Non-Conventional Tendon Advance for injuries in zones I and II New Surgical Technique. J. Clinical Orthopedics and Trauma Care, 3(1); Doi:10.31579/2694-0248/013
Copyright: © 2021 Francisco López Bustos, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 12 October 2021 | Accepted: 22 November 2021 | Published: 10 December 2021
Keywords: Non-Conventional Tendon
Once a primary suture of flexor tendon in zone II of Verdan is unable to be performed, or in those cases in which a re-rupture of a primary tenorraphy occurs, the tendon graft is the goldstandard option.
Once a primary suture of flexor tendon in zone II of Verdan is unable to be performed, or in those cases in which a re-rupture of a primary tenorraphy occurs, the tendon graft is the goldstandard option.
The adherence rates in primary suture, as well as the inherent co-morbilty related to use of tendon grafts whether from the forearm or the foot, are widely known [1, 2, 3].
The results of these last methods are, in most of their cases, less satisfactory than those in which primary suture is carried out.
Considering these instances, a procedure which dispenses flexor graft is presented.
This technique consist in performing a zetaplasty in zone V of the proximal stump of the flexor committed, making its progress in that area, and thereby achieving the distal stump to carry out an end to end suture in zone I or II. In case the shortening of the proximal stump is considerable, and thus the end to end suture is unable, we propose to suture then lengthened proximal stump to the nearest uninjured flexor profundus tendon.
In earlier reports from 1950[1] and 1981[1], encouraging results of lengthening of flexor pollicis longus in zone V for rupture of this tendon are described. Le Viet [1] performed a zetaplasty of profundus flexors in order to achieve a primary suture in cases of retraction of the proximal stump.
In a more recent study [1], these procedures are described just for treatment of jersey finger injuries.
In view that these techniques have been used only for specific cases, we consider important to describe our results in other cases.
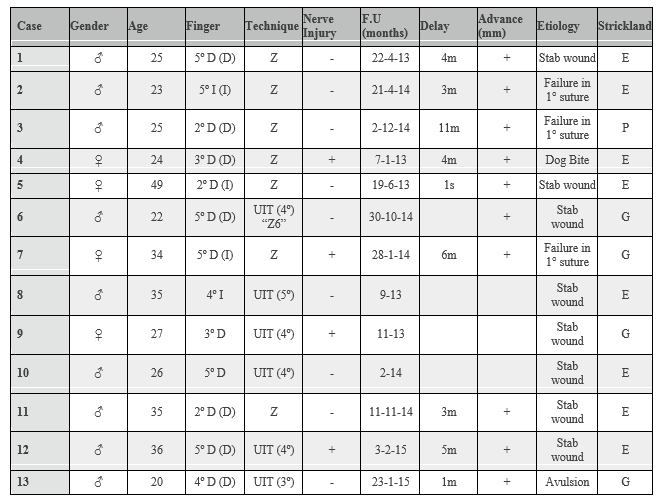
13 flexor tendon injuries in 13 patients were operated on.
9 (69,23 %) were male, and 4 were female. Average age was 29 years (range 20-49 years). Dominant hand was affected in 84,61 % of the cases (11 of 13 cases).
The most affected finger was the little (6 cases), followed by the index (3 cases). Middle (2 cases), and ring (2 cases) completed the series.
7 cases constisted of rupture of primary suture of profundus flexor tendon, and the remaining 6 were untreated profundus flexor tendon injuries which had such degree of shrinkage, that make impossible any attempt to carry out an end to end suture.
In 4 cases (30,77 %) suture of injured collateral nerves was excute. This procedure delayed the rehabilitation period.
In 7 cases tendon advance was performed by zetaplasty in zone V of the same affected tendon, thus achieving the distal stump to carry out the end
to end suture.
In 6 cases in which the shortening of the proximal stump was considerable, a suture of the lengthened proximal stump to the nearest and unscathed profundus flexor tendon was execute.
After surgery, an above elbow cast was used for protection of the suture for 4 weeks.
Rehabilitation exercises began following the removing of the cast, and progressive load was applied to the hand 8 weeks after the surgery.
Strickland punctuation system [2] was used to assess the results.
“Statistical analysis was carried out with an IBM SPSS Statistics 19.0”. This analysis was developed with a non-parametric median test.
Average follow up was 17,23 months (rate 32-6 months).
Tendon progress achieved for the total sample was 20,53 mm (12-32 mm).
Zetaplasties in zone V yielded an average advance of 18 mm, whereas the inter-tendon sutures 23,5 mm. These contrasts were statistically significant. (p=0,029).
Regarding the Strickland punctuation, good and excellent results were present in almost all cases.

Reconstruction of profundus flexor tendon is indicated in cases of failure of primary repairs, late diagnosis with retraction of proximal stump, and in complex injuries with tissue defect.
Prognosis in reconstructions is determined by the delay in treatment, the rate of tendon retraction, it´s blood supply, the soft tissue environment, the indemnity of the superficial flexor tendon, and surgeon´s experience.
Surgical options include tendon advance, grafts in one or two procedures, tendon transfers, and silastic prosthesis. Other rescue surgeries include arthrodesis, capsulodesis, and tenodesis, etc.
According to bibliography, grafts in all its variants, are the most popular and the very first chosen. Although, there is not still agreement on which tendon would be the best graft, diameter, length, and resilience must be taken into consideration. The most often used are Flexor Palmaris Brevis, Plantaris, Extensor Digiti Quinti, Extensor Indicis, and Toes Extensors [1, 2 ,3] .Allografts have also been proposed [12].
More recently, in a series of 71 cases [13], vascularized tendon grafts have been proposed.
Synthetic implants can be used, provided they are well tolerated [13, 14, 15].
Sita and Durand, [16] proposed the reconstruction in zones I and II by transferring a half tendon of the adjacent flexor superficialis tendon.
Regarding tendon lengthening in forearm [6], there have been recent reports. Chanel et al, [7] in 2014 assessed the advance of flexor profundus tendon by performing a zetaplasty as a treatment for the jersey finger. This tendon advance was limited due to presence of the lumbrical muscle and the synovial adherence. No restrictions in the index were reported. Although this technique was proposed for this last pathology, we consider that the zetaplasty might weaken the tendon, and therefore increase the adherence rate.
Any of these procedures needs a very careful technique and an extensive experience in flexor tendon repair.
With regard to this technique, we consider among its advantages, the minor complexity, the lower co-morbidity, and the decrease in surgical time. These benefits might be greater in case more fingers are needed of repair.
The proposed technique can be applied in 1 or two steps.
Since the tendon original blood supply is preserved, and the anatomic diameters of the stumps are similar, the glide through the pulleys shall not be restricted.
A weakness in the tendon after the zetaplasty, which can be reinforced by inter tendon suture, might be a disadvantage of the technique.
We consider that the number of cases is still low, but the short term results encourage continuing to perform this technique regarding its simplicity, low morbidity, and early recovery.
Proper indications for this new technique of non-conventional tendon advance of the fingers in injuries in zones I and II are: acute and chronic trauma where the retraction of the proximal stumps makes the primary suture unable.
Its versatility lies on the possibility of carrying out an end to end suture of a retracted tendon disregarding a tendon graft. A Z lengthening is performed in the proximal stump in zone V so as to suture it to the distal stump, or to attach this last one to the distal phalanx.
We emphasize that the requirement of tendon grafts is left aside, decreasing thereby the morbidity of the procedure.
The need of a second approach in the wrist must be considered, though, in order to carry out the zetaplasty, tendon advance, or inter tendon suture.
The performance in 1 or 2 steps can be determined by the surgeon, provided the presence of adherences, or the requirement of reconstruction of the pulleys.
This new technique is presented as an alternative to the classic option of the tendon grafts in cases of a single or multiple injuries of flexor tendons.
More comparative studies will be needed so as to achieve more definitive conclusions.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
