
Research Article | DOI: https://doi.org/10.31579/2641-0419/416
¹Assistant professor of interventional cardiology, Department of cardiology, Tehran Heart Center, Tehran university of Medical Sciences, Tehran, Iran
²Shahroud University of medical sciences, Imam Hossein Hospital
³Student research committee, Faculty of medicine, Shahid Beheshti University of Medical Sciences, Tehran, Iran
⁴Department of Sports and Exercise Medicine,Imam Khomeini Hospital (Tums), Tehran, Iran
⁵Cardiovascular Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran
*Corresponding Author: Mehdi Sheibani, Department of Cardiology, Shahid Beheshti University of Medical Sciences, Loghman-hakim Hospital, kamali Avenue, South Kargar Street, Tehran, Iran.
Citation: Mohammad Sadeghian, Maryam Ahmadi, Hossein Toreyhi, Najmeh Ahmadpour, Mahshid Nazarieh, et al, (2024), No-Reflow Phenomenon after Primay Percutaneous Coronary Intervention in patients with ST segment elevation myocardial infarction treated with ticagrelor versus clopidogrel plus eptifibatide: A Randomized Clinical Trial, J Clinical Cardiology and Cardiovascular Interventions, 7(12); DOI: 10.31579/2641-0419/416
Copyright: © 2024, Mehdi Sheibani. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 16 September 2024 | Accepted: 30 September 2024 | Published: 21 October 2024
Keywords: no reflow phenomenon; primary percutaneous intervention; Tcagrelor; eptifibatide
Background and Aims
No reflow phenomenon (NRP) is one of the essential complications of primary percutaneous intervention (PPCI). Anti-platelets have essential role in prevention of NRP. The aim of this study is comparison the NRP between ticagrelor and clopidogrel+glycoprotein IIb/IIIa Inhibitor in ST elevation myocardial infarction (STEMI) patients candidate for PPCI.
Methods
From January 2022 to January 2023 in a randomized clinical trial we compare ticagrelor and clopidogrel plus eptifibatide (a glycoprotein IIb/IIIa inhibitor) in terms of NRP and secondary outcome include mortality, stent thrombosis, vascular complications, bleeding complications and major cardiovascular adverse events (MACE). NRP was defined as TIMI flow grade less than 3.
Results:
140 patients were randomly assigned to two study groups. Mean age of patients was 59 years and 82% were male. Baseline characteristics and culprit vessels was not significantly different between study groups.NRP at the end of procedure was occurred in 47.5% in ticagrelor group and 53.7% in clopidogrel + eptifibatide group without statistical significant difference (Pvalue: 0.48). Two major and two minor bleeding occurred in in the clopidogrel+eptifibatide group and no bleeding was reported in ticagrelor group. Bleeding complications was not significantly different between study groups. In hospital mortality, vascular complications and MACE were also not significantly different between study groups.
Conclusion:
Clopidogrel plus eptifibatide in PPCI has similar outcome with ticagrelor and could be administered if ticagrelor is unavailable or prohibited.
PPCI: Primary percutaneous intervention
STEMI: ST-segment elevation myocardial infarction
NRP: No-reflow phenomenon
GFR: glomerular filtration rate
CABG: coronary artery bypass graft surgery
ACT: activated clotting time
Primary percutaneous intervention (PPCI) is the treatment of choice recommended by the European Society of Cardiology's international guidelines to restore epicardial coronary supply in ST-segment elevation myocardial infarction (STEMI). (1) Despite significant reductions in STEMI mortality achieved through PPCI, STEMI still results in 7
Study population
This is a prospective, randomized clinical trial of patients with STEMI at Imam Khomeini Hospital in Tehran from January 2022 to January 2023. This study was approved by Medical Ethics Committee of Tehran University of Medical Sciences and registered in Iranian Registery of Clinical Trial (code: IRCT2020318046810N1). Patients with the diagnosis of STEMI whom candidate for primary PCI entered the study. Informed consent was obtained from all patients. Moreover, patients with the following conditions were excluded: patients on ticagrelor or clopidogrel, patients with cardiogenic shock, patients with CHF decompensation (NYHA class III & IV ), patients with severe valvular heart disease, patients whom referred after 12 hours of MI event based on history, patients older than 85 years old, low serum platelet count (<100>
A case report sheet includes demographic data, past medical history, cardiovascular risk factors and laboratory tests was filled for each patient. Basic ECG and ECG of 90 minutes after PCI were evaluated by a cardiologist to determine ST resolution. ST resolution was defined as at least 50
SPSS ver. 26 software was used to perform the statistical analysis of the data. The qualitative variables in the statistical study were described as percentages and ratios using descriptive indicators. A proportional statistical test with Chi-Square was also used to investigate the relationship between qualitative and qualitative variables, or if Chi-Square conditions were not met and the two-state qualitative variable was compared, the Fisher-Exact test was used. A significant level was defined as a P-value less than 0.05. Linear regression analysis was performed to examine the independent relationship of various variables with the endpoints under consideration Furthermore, as sensitivity analysis, we compare groups after excluding participants undergone thrombo-aspiration.
After considering the inclusion and exclusion criteria and receiving informed consent, 140 people were enrolled in the study, with 14 of them being excluded after randomization. Five patients excluded due to cardiogenic shock during PCI and 9 patients candidates for urgent CABG and stent implantation was not done for them (Figure 1) .Therefore, a total of 67 patients were treated with clopidogrel plus eptifibatide, and 59 patients were treated with ticagrelor.
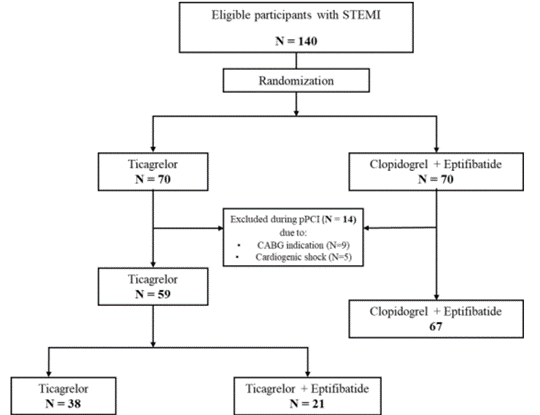
Figure 1: Algorithm of patient selection and randomization. STEMI: ST segment Elevation Myocardial Intervention, CABG: Coronary Arteries Bypass Graft Surgery, PPCI: primary percutaneous intervention
Table 1 shows the participants' baseline characteristics. One hundred and four (82.5 %) of the participants were men. The mean [standard deviation (SD)] age of the participants was 59.13 (12.20), with no significant differences between study groups. Furthermore, the study groups had no differences in terms of basic characteristics and risk factors except mean plasma creatinine level and prevalence of type 2 diabetes mellitus (T2DM).
| Demographic information | Total (n=126) | Clopidogrel + Eptifibatide(n=67) | Ticagrelor(n=59) | P value |
| Male | 104 (82.5) | 55 (82.1%) | 49 (83.1) | 0.88** |
| Female | 22 (17.5) | 12 (17.95) | 10 (16.9) | |
| Age (years) | 59.13 (12.20) | 58.91 (11.78) | 59.38 (12.76) | 0.77 |
| - Weight (kilogram) | 77.70 (11.67) | 76.19 (12.45) | 77.81 (10.77) | 0.50 |
| - Height (centimeter) | 174.35 (55.43) | 168.87 (22.44) | 180.57 (77.30) | 0.67 |
| - BMI, (kg/m2) | 26.22 (3.52) | 25.83 (3.75) | 26.66 (3.22) | 0.45 |
| Plasma creatinine, mg/dl | 1.1 (0.26) | 1.16 (0.24) | 1.04 (0.26) | 0.017 |
| Comorbidities | ||||
| - Smoker, n (%) | 58 (46) | 29 (43.3) | 29 (49.2) | 0.51 |
| - Hypertension, n (%) | 45 (35.7) | 25 (37.3) | 20 (33.9) | 0.69 |
| - T2DM, n (%) | 30 (23.8) | 10 (14.9) | 20 (33.9) | 0.013 |
| - Opium addiction, n (%) | 29 (23) | 19 (28.4) | 10 (16.9) | 0.12 |
| - Hyperlipidemia, n (%) | 23 (18.3) | 15 (22.4) | 8 (13.6) | 0.20 |
| - IHD, n (%) | 11 (8.7) | 5 (7.5) | 6 (10.2) | 0.59 |
| - Family history of premature CVD, n (%) | 11 (8.7) | 7 (10.4) | 4 (6.8) | 0.46 |
| - History of CVA, n (%) | 2 (1.6) | 1 (1.5) | 1 (1.7) | 1 |
BMI; body mass index, T2DM; type2 diabetes mellitus, IHD; ischemic heart disease, CVD; cardiovascular disease, CVA; cerebrovascular accident *Values are shown as Mean (SD) and number (%), for continuous and categorical variables, respectively. ** Unlike other p-values, the suggested one is related to the difference between men and women. | ||||
Table 1. Baseline characteristic of the participants *.
Twenty (34%) patients in the ticagrelor group and 25(37%) patients in the clopidogrel + eptifibatide group receive morphine sulfate in the emergency room and there was no significant difference between study groups (p value: 0.69).
Table 2 illustrates the MI characteristics of the participants, including STE type based on electrocardiogram (ECG), stenotic vessels, and culprit vessels. With a prevalence of 52 (41.3%) and 32 (25.4%), respectively, the most common types of STEMI among study participants were inferior and anterior MI. Notably, no significant differences in STEMI type were found between the study groups. The LAD was the most commonly culprit vessel, accounting for 67 (53.2 percent) of total participants. In this study, a total of 226 arteries had significant obstruction with had no significant difference between two study groups. Twenty-six (20.7%) patients were single vessel disease, 72 (57.1%) were two vessel disease and 28 (22.2%) were three vessel disease. It should be noted that due to high thrombotic bulk, 13 (10.3%) patients underwent thrombo-aspiration (9 patients in clopidogrel + eptifibatide group and 4 patients in ticagrelor group) and 77 (61.1%) patients underwent pre-dilatation (46 patients in clopidogrel + eptifibatide group and 31 patients in ticagrelor group (at the discretion of the operator. Forty one patients (32.5%) was post-dilated with non-compliant balloons at the session of primary PCI due to stent under-expansion (25 patients in the Plavix + eptifibatide and 16 in the ticagrelor group). There was no difference in the number of patients who underwent this procedures between study groups (p values: 0.22, 0.06 and 0.43 for thrombo-aspiration, pre-dilation and post-dilation respectively).
| Type of STEMI | Total | Clopidogrel + Eptifibatide | Ticagrelor | P value | ||||
Anterior (V2-V4) | ||||||||
| 32 (25.4%) | 20 (29.9%) | 12(20.3%) | ||||||
Extensive anterior (V1-V6) | 21 (16.7%) | 8 (11.9%) | 13 (22.0%) | |||||
Anterolateral (V2-V4, I, aVL) | 6 (4.8%) | 5 (7.5%) | 1 (1.7%) | |||||
Extensive anterolateral (V1-V6, I, aVL) | 6 (4.8%) | 4 (6%) | 2 (3.4%) | |||||
Inferior (II, III, aVF) | 52 (41.3%) | 28 (41.8%) | 24 (40.7%) | 0.22 | ||||
Inferolateral (I, II, III, aVF, aVL) | 2 (1.6%) | 0 (0%) | 2 (3.4%) | |||||
Inferior+ RV (II, III, aVF, V4R-V6R) | 4 (3.2%) | 1 (1.5%) | 3 (5.1%) | |||||
Lateral (I, aVL, V5, V6) | 2 (1.6%) | 1 (1.5%) | 1 (1.7%) | |||||
Inferoposterior (II, III, aVF, V7-V9) | 1 (0.8%) | 0 (0%) | 1 (7%) |
| ||||
| Culprit vessels | ||||||||
| LAD | 67 (53.2%) | 38 (56.7%) | 29 (49.2%) | |||||
| RCA | 48 (38.1%) | 26 (38.8%) | 22 (37.3%) | 0.19 | ||||
| LCX | 11 (8.7%) | 3 (4.5%) | 8 (13.6%) | |||||
| Stenotic vessels * | ||||||||
| LAD | 33 (26.2%) | 17 (25.4%) | 16 (27.1%) | |||||
| LCX | 5 (4.0%) | 1 (1.5%) | 4 (6.8%) | |||||
| RCA | 16 (12.7%) | 8 (11.9%) | 8 (13.6%) | 0.30 | ||||
| LAD-LCX | 20 (15.9%) | 13 (19.4%) | 7 (11.9%) | |||||
| LAD-RCA | 18 (14.3%) | 13 (19.4%) | 5 (8.5%) | |||||
| LCX-RCA | 6 (4.8%) | 3 (4.5%) | 3 (5.1%) | |||||
| LAD-LCX-RCA | 28 (22.2%) | 12 (17.9%) | 16 (27.1%) | |||||
STEMI: ST-elevation myocardial infarction, LAD: left anterior descending artery, RCA: right coronary artery, LCX: left circumflex artery Values are shown as number (%) variables. *stenotic vessel was defined as vessels with more than 50% luminal stenosis | ||||||||
Table 2. Details of STEMI among study participant. | ||||||||
| Total | Clopidogrel + Eptifibatide | Ticagrelor | P value | |||||
| Type of STEMI | ||||||||
- Anterior (V2-V4) | 32 (25.4%) | 20 (29.9%) | 12(20.3%) | |||||
- Extensive anterior (V1-V6) | 21 (16.7%) | 8 (11.9%) | 13 (22.0%) | |||||
- Anterolateral (V2-V4, I, aVL) | 6 (4.8%) | 5 (7.5%) | 1 (1.7%) | |||||
- Extensive anterolateral (V1-V6, I, aVL) | 6 (4.8%) | 4 (6%) | 2 (3.4%) | |||||
- Inferior (II, III, aVF) | 52 (41.3%) | 28 (41.8%) | 24 (40.7%) | 0.22 | ||||
- Inferolateral (I, II, III, aVF, aVL) | 2 (1.6%) | 0 (0%) | 2 (3.4%) | |||||
- Inferior+ RV (II, III, aVF, V4R-V6R) | 4 (3.2%) | 1 (1.5%) | 3 (5.1%) | |||||
- Lateral (I, aVL, V5, V6) | 2 (1.6%) | 1 (1.5%) | 1 (1.7%) | |||||
- Inferoposterior (II, III, aVF, V7-V9) | 1 (0.8%) | 0 (0%) | 1 (7%) | |||||
| Culprit vessels | ||||||||
| - LAD | 67 (53.2%) | 38 (56.7%) | 29 (49.2%) | |||||
| - RCA | 48 (38.1%) | 26 (38.8%) | 22 (37.3%) | 0.19 | ||||
| - LCX | 11 (8.7%) | 3 (4.5%) | 8 (13.6%) | |||||
| Stenotic vessels * | ||||||||
| - LAD | 33 (26.2%) | 17 (25.4%) | 16 (27.1%) | |||||
| - LCX | 5 (4.0%) | 1 (1.5%) | 4 (6.8%) | |||||
| - RCA | 16 (12.7%) | 8 (11.9%) | 8 (13.6%) | 0.30 | ||||
| - LAD-LCX | 20 (15.9%) | 13 (19.4%) | 7 (11.9%) | |||||
| - LAD-RCA | 18 (14.3%) | 13 (19.4%) | 5 (8.5%) | |||||
| - LCX-RCA | 6 (4.8%) | 3 (4.5%) | 3 (5.1%) | |||||
| - LAD-LCX-RCA | 28 (22.2%) | 12 (17.9%) | 16 (27.1%) | |||||
STEMI: ST-elevation myocardial infarction, LAD: left anterior descending artery, RCA: right coronary artery, LCX: left circumflex artery Values are shown as number (%) variables. *stenotic vessel was defined as vessels with more than 50% luminal stenosis. | ||||||||
Table 2. Details of STEMI among study participant.
Table 3 shows continuous and categorical analysis of TIMI flow results. The mean (SD) mid-procedure TIMI flow score (after crossing the wire) for the clopidogrel + eptifibatide and ticagrelor groups was 1.88 (0.47) and 1.96 (0.41), respectively. The mean TIMI flow score in these groups at the end of the procedure (after stent implantation and post dilation if required) was 2.41 (0.60) and 2.94 (0.56), respectively. There was no significant difference between the two groups in terms of mid-TIMI flow (p-value: 0.276) or end-TIMI flow (p-value: 0.515). After crossing the wire and at the end of the procedure, 63 (94%) and 36 (53.7%) of the clopidogrel + eptifibatide group had TIMI flow scores of less than 3. Similarly, in the ticagrelor group, 55 (93.2 percent) and 28 (47.5 percent) of patients experienced mid-procedure and end-procedure no reflow phenomenon (TIMI flow < 3>(Supplementary Table3).
| Table 3. Continues and categorical analysis of TIMI flow | ||||
| Total | Clopidogrel + Eptifibatide | Ticagrelor | P value | |
| Continues | ||||
| Mid-procedure | 1.92±0.44 | 1.88±0.47 | 1.96±0.41 | 0.27 |
| End-procedure | 2.45±0.58 | 2.41±0.60 | 2.94±0.56 | 0.51 |
| Categorical | ||||
| Mid-procedure | ||||
| - 3 | 8(6.3%) | 4(6.0%) | 4(6.8%) | 1 |
| - < 3> | 118(93.7%) | 63(94.0%) | 55(93.2%) | |
| End-procedure | ||||
| - 3 | 62(49.2%) | 31(46.3%) | 31(52.5%) | 0.48 |
| - < 3> | 64(50.8%) | 36(53.7%) | 28(47.5%) | |
Values are shown as Mean (SD) and number (%), for continuous and categorical variables, respectively. Mid-procedure: after crossing the wire, end-procedure: after stent implantation | ||||
| Supplementary Table3. Continues and categorical analysis of TIMI flow after excluding patients who had undergone thrombo-aspiration | ||||
| Total | Clopidogrel + Eptifibatide | Ticagrelor | P value | |
| Mid-procedure | ||||
| - 3 | 7(6.2%) | 3(5.2%) | 4(7.3%) | 0.71 |
| - < 3> | 106(93.8%) | 55(94.8%) | 51(92.7%) | |
| End-procedure | ||||
| - 3 | 57(50.4%) | 27(46.6%) | 30(54.5%) | 0.39 |
| - < 3> | 56(49.6%) | 31(53.4%) | 25(45.5%) | |
Values are shown as Mean (SD) and number (%), for continuous and categorical variables, respectively. Mid-procedure: after crossing the wire, end-procedure: after stent implantation | ||||
Supplementary Table 3: Mid-procedure: after crossing the wire, end-procedure: after stent implantation
Given that 21 patients of the ticagrelor group whom had NRP, were treated with eptifibatide on the recommendation of the operator, secondary outcomes were compared in the three clopidogrel + eptifibatide, ticagrelor, and ticagrelor + eptifibatide groups. TIMI flow was evaluated before Eptifibatide in all patients in the ticagrelor group. The mean EF of the patients in each group after the procedure was 35.59% (10.71) in the clopidogrel + eptifibatide group, 36.57% (9.01) in the ticagrelor group, and 33.80% (12.93) in the ticagrelor + eptifibatide group. The EF differences between groups were not statistically significant (p-value: 0.79). Furthermore, the mean duration of hospitalization in the three groups was 5.83 (2.67), 5.73 (2.23), and 5.33 (2.0), with no difference between the three groups (p-value: 0.77).
Patients' post-procedure complications are illustrated in Table 4. Vascular complications occurred in two patients, one in the clopidogrel + eptifibatide group and the other in the ticagrelor group, with no statistically significant difference (p-value = 0.95). Only two people in the clopidogrel + eptifibatide group experienced major bleeding. Similarly, only two patients in the same group experienced minor bleeding. Furthermore, only one patient in the ticagrelor group experienced minimal bleeding. Bleeding requiring medical attention occurred in 2, 1, and 1 patient in the clopidogrel + eptifibatide, ticagrelor, and ticagrelor + eptifibatide groups, respectively. However, there was no significant difference in the incidence of bleeding (of any kind) between the three groups (p-value = 0.70). In the clopidogrel + eptifibatide, ticagrelor, and ticagrelor + eptifibatide groups, the incidence of MACE was 3%, 2.6%, and 9.5 %, respectively. The difference in MACE between the three groups was not statistically significant (p-value: 0.35). Stent thrombosis occurred in one patient of the ticagrelor group and no stent thrombosis occurred in other two groups.
| Total | Clopidogrel + Eptifibatide | Ticagrelor | Ticagrelor + Eptifibatide | p-value | |
| Vascular | 2 (1.6%) | 1(1.5%) | 1(2.6%) | - | 0.73 |
| Bleeding | 0.63 | ||||
| Major | 2 (1.6%) | 2 (3%) | - | - | |
| Minor | 2 (1.6%) | 2 (3%) | - | - | |
| Minimal | 1 (0.8%) | - | 1 (2.6%) | - | |
| Require medical attention | 4 (3.2%) | 2 (3%) | 1 (2.6%) | 1 (4.8%) | |
| Total | 9 (7.1%) | 6 (9.0%) | 2 (5.3%) | 1 (4.8%) | 0.70 |
| Contrast nephropathy | 10 (7.9%) | 5 (7.5%) | 3 (7.9%) | 2 (9.5%) | 0.95 |
| MACE | 5 (4%) | 2 (3%) | 1 (2.6%) | 2 (9.5%) | 0.35 |
| MACE: major adverse cardiac and cerebrovascular events | |||||
Table 4: The complications of participants after procedures during hospitalization.
The current study included 126 STEMI patients who were candidates for primary PCI and we compared them in the two groups of clopidogrel + eptifibatide and ticagrelor in terms of safety and efficacy of anti-platelet therapy. The initial characteristics of the two groups were nearly identical. The TIMI Flow findings indicate that No-reflow phenomenon does not differ significantly between these groups. Moreover, we didn’t find any difference in adverse events between study groups.
High platelet activity was seen to has association with NRP in STEMI patients.(7) Ticagrelor, as a reversible direct-acting oral antagonist of P2Y12- receptor antagonist with no catabolite activation, could have a significant impact on platelet inhibition faster and more consistently than clopidogrel. (8) The efficacy and safety of ticagrelor and clopidogrel were compared in previous studies with acceptable heterogenicity (I2 = 64%) in a meta-analysis conducted by Wang et al. (9) They found no differences in efficacy or risk of bleeding, MI, or stroke between the two groups. Another meta-analysis by Dai etal reported that loading dose of ticagrelor compare with clopidogrel effectively reduces NRP during PPCI. (10) In PLEIO study the superiority of ticagrelor to clopidogrel in recovery of endothelial function is shown .(11)In contrast to this findings a recent clinical trial showed that the incidence of NRP is not affected by the type of P2Y12Inhibitor.(12) Eptifibatide is a short-acting, small-molecule competitive inhibitor of the GP IIb/IIIa receptor. (13) The role of GP II/III inhibitors, particularly tirofiban, has always been taken into account. According to a meta-analysis of prior trials on the effect of tirofiban on TIMI flow result, it reduces the risk of thrombosis by approximately 75% and the risk of MACE by 90%. (14) A recent meta-analysis reported the effectiveness of tirofinal and eptifibatide in preventing NRP in primary PCI. (15) Given that this drug's bleeding trend did not reach a significant level, it would be a promising choice for combination therapy for ACS patients. Another meta-analysis on two common glycoprotein inhibitors, tirofiban and eptifibatide, found that treatment with tirofiban or eptifibatide had no effect on favorable outcome, functional outcome, or last available National Institutes of Health Stroke Scale (NIHSS), but may increase mortality. (16) However, considering tirofiban increased the risk of fatal ICH while decreasing the risk of ICH, maybe eptifibatide could be a better option to adjunctive therapy.
However, the efficacy of the addition of eptifibatide to clopidogrel has been examined by Moazez et al in a randomized clinical trial. (17) They suggested that platelet reactivity could be further reduced by using glycoprotein IIb/IIIa inhibitors in addition to P2Y12 inhibitors. It is worth noting that the endpoint of this study was based on laboratory measurements of platelet aggregation (PA) and activated clotting time (ACT). Because of the therapeutic dose of heparin used in this study, laboratory measurements could be easily influenced by confounding factors. The major adverse effects of combination therapy were not compared in this study, and the safety of eptifibatide should be investigated in future studies (18) To the best of our knowledge, this is the first study to compare the efficacy and safety of the eptifibatide plus clopidogrel versus ticagrelor in the total ACS population with any troponin level status.
Shimada et al evaluated whether the use of a glycoprotein IIb/IIIa inhibitor improves the relative efficacy and safety of ticagrelor when compared to clopidogrel in the Platelet Inhibition and Patient Outcomes (PLATO) Trial. (19) However, no interaction was found between treatment and tirofiban use for the primary efficacy and safety end points of P2Y12 inhibitors. Moreover, stent thrombosis was found with a prevalence of about 1% in the ticagrelor group with GP IIb/IIIa inhibitor.
In our study, stent thrombosis was observed in only one case of the ticagrelor group, while the other two groups did not report any cases of MI or stent thrombosis. Due to the small number of patients, we did not have enough power to evaluate and compare stent thrombosis in different groups.
Some limitations could be considered for this study. This study was conducted in one center with 140 patients. We recommend to design a multicenter study with more cases to confirm our findings.
Clopidogrel plus eptifibatide in PPCI procedure for STEMI has similar outcomes with ticagrelor and could be administered if ticagrelor is unavailable or prohibited.
“This research received no specific grant from any funding agency in the public or commercial.
The authors declare that they have no competing interest.
All authors have read and approved the final version of the manuscript and had full access to all of the data in this study and takes complete responsibility for the integrity of the data and the accuracy of the data analysis.
Mehdi Sheibani affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
