
Review Article | DOI: https://doi.org/10.31579/2640-1053/200
*Corresponding Author: Ahmad Reza Rahnemoon. Retired at hematology department, I.U.M.S, Tehran, Iran.
Citation: Ahmad R. Rahnemoon, (2024), Niche remodeling during aging process. J. Cancer Research and Cellular Therapeutics. 8(4); DOI:10.31579/2640-1053/200
Copyright: © 2024, Ahmad Reza Rahnemoon. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 01 July 2024 | Accepted: 10 July 2024 | Published: 18 July 2024
Keywords: Niche; aging; remodeling; hematopoietic malignancy
Aging of hematopoietic system might result from hematopoietic stem cell (HSC) and micro-environmental alterations with changes at the location, regulation and function of HSC and their progeny. Hereby, we can state the relative contribution of the aged micro-environment and the graduate alterations which changed hematopoiesis and increased incidence of age-related diseases originating in the bone marrow environment. Here, we focus on a better understanding of the biology of aging in HSCs and their niche. In summary, studies on the micro-environment that maintains and regulates HSC and its niche suggested that micro-environmental aging contributes to declined HSC function over time. After this period, aged HSCs and their derivatives remodel the niche in changing to favor myeloid expansion.
Niche specific cell populations, varied growth factors, extra cellular matrix and cell adhesion molecules produced by niche cells are integrated with each other for controlling stem cell behavior common goal. It is mentionable that HSCs locate in unique niches which offers a pivotal microenvironment for HSC quiescence, activation, differentiation and expansion. In this pathway, mature blood and immune cells are generated by hematopoiesis which has been modeled as a stepwise differentiation process in the core of which reside HSCs. Thus, early hematopoiesis is now viewed as a continuous landscape composed of undifferentiated HSCs with a variable degree of priming toward specific lineages including lymphoid, myeloid or erythroid base on a tree-like hierarchy arises from HSCs in which lineage commitment occurs at binary branching points to homogenous progenitor populations. In the better words, the BM niche is comprised of many different cell types including mesenchymal stromal cells, osteo-progenitor derivatives, endothelial cells, adipocytes, sympathetic nervous system and blood of specific immature and mature cells such as megakaryocytes as well as monocyte, neutrophil and erythroid precursors. [12,13,21,22]

Figure 1: Schematic model in autophagy inhibition, MSCs dysfunction and bone loss. (27)
Arch and chip:
Clonal populations existence in the BM, identified the expansion of more than one genetically distinct cell populations, is increasingly being viewed as a phenomenon in age related inflammation or the age associated surge in systemic inflammation. Recent characterization of clonal hematopoiesis in a large segment of aging population has raised tremendous interest and concern alike. Mutations have been documented in genes associated with hematological cancers. So in challenging between clonality and malignancy, age related clonal hematopoiesis (ARCH) refer to clonal hematopoiesis caused by any type of acquired clonal event or ARCH describe as an inevitable consequence of aging which in this condition, many of the intrinsic aspects of HSC are affected by the aging process resulting in a deterioration in their potential, independently of their microenvironment. But clonal hematopoiesis of indeterminate potential (CHIP) refers to the mutation of a gene like DNMT3A, TET2, etc. with a variant allele frequency greater than 2% that happen in 10%-40 % cases and can progress to an increased risk of blood cancers as well. Hence, these potent clones with: a) increasing age, b) genomic instability, c) age related inflammation and at last external environmental cues that can accumulate in the BM, reaching a stage known as CHIP. Notably, when the hematopoiesis become abnormal or marked by additional mutations acquisition as well as other additional external factors, the malignancy can appear. [1-4,7-10] In reality, on the one hand, some mutations can establish as a detectable clone of hematopoietic cells in healthy individuals which lacking any hematological cancer evidence. Hence, the clonal hematopoiesis becomes commoner with age and can detect in the people aged particularly in 90 years or even older, which can appear acquire additional mutations such as FLT3 or NPM1 that go to generate into the expansion of acute leukemia. Also, the number and frequency of HSC in the BM of mice and humans increase with aging, while their regenerative capacity measured in transplantation assays in clearly reduced, notably that is caused primarily by cell intrinsic mechanism even though an aged microenvironment can further aggravate it. So that’s why, hematopoietic function severely decline with age, also sometimes anemia, impaired adaptive immunity, autoimmune disease and cancer may be happened in the elderly. Aging can lead to major changes in bone and BM cavity which provide specialized niches for introduce the distinguished role of HSC in the niche. Now, this is clear that intrinsic changes in the BM microenvironment contribute to old HSC dysfunction but the concept and mechanisms driving niche aging much less is known and additionally the role of influence of old niche on hematopoietic aging. In the other words, during aging, the hematopoietic system can be with various changes including increase in the relative number of HSCs that presumably aims to compensate for a repopulation ability loss (figure 1). So, increasing in HSCs and decreasing in total BM cellularity may be happened, also lymphocyte production loss, increase in the number of platelet primed HSCs and a skewing toward myeloid differentiation have been demonstrated. Generally, loss of immune function that affects innate and adaptive immunity together has been reported. So, as mentioned above, ARCH is defined as the expansion of HSC clones, harboring specific, recurrent genetic variants and disruptive without any hematologic malignancy because, ARCH in human blood system occur in B and T cells, also in cells of the innate system and HSCs as well. [5,6,11-17]
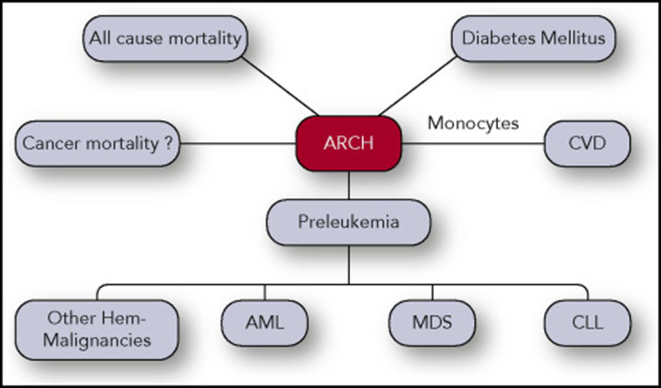
Figure 2: ARCH is defined as the gradual, clonal expansion of HSC 0r other progenitor cells carrying specific, disruptive to changes in the micro-environmental niche and recurrent genetic variants which can increase the risk for pre-leukemia or/and leukemia as well. [1]
It is mentionable that some ARCH cases are clearly pre-leukemic (will certainly evolve to leukemia) as was demonstrated by several researchers. Actually, pre-leukemia referred to a heterogeneous group of hematopoietic disorders associated with a block in myeloid differentiation as well as chronic cytopenias. In pre-leukemia position appear to have an identical clonality of both myeloid and lymphoid compartments. It suggest that the
clone can initiate in a very early hematopoietic stem cell. In this case, the mutant genes involve in ineffective dysplastic hematopoiesis pathway. In other words, some driver mutations produce an essential block in differentiation providing a proliferative advantage to the clone cells. In fact, chronic inflammation or exposure to specific environmental stimulus might allow such clones to become dominant.

Figure 3: ARCH is the clonal expansion of at least single HSCs capable of multi-lineage differentiation. Please look at genetic alterations after clonal expansion of cancer cell and additionally the important role of disruptive influences of cancer cells in the hematopoietic micro-environment. (Google website)
For example, among elderly who received chemotherapy and developed therapy induced MDS/AML, 62% had ARCH before chemotherapy, however 15% of match controls (who did not develop MDS/AML) had ARCH. Taken together these studies indicate that there is a clear relationship between ARCH and CHIP, but more CHIP specifically to the malignant hematopoietic development (figure 2). Although, some researchers stated that when clonal hematopoiesis documented in individuals with unexplained cytopenia and no CHIP criteria, the positive predictive value of progression to a myeloid cancer is very high. It is important to consider that ARCH related mutations may have distinct functional consequences during ARCH evolution and later during leukemia progression to leukemia clones evolution (figures 2, 3 & 4). That’s why, clonal hematopoiesis offers a new opportunity to understand the important role of niche and also the biology and adaption mechanisms of aging and malignant transformation mechanism as well. Therefore, cancer is not a single disease but instead is morphological and biological features. As a result, cancer stem cells (CSCs)reside at the apex of the hierarchy and are thought to possess the cancer initiating cells, their microenvironment and metastatic ability as well. [1-9]
Hematopoietic aging:
Hematopoietic aging is marked by a loss of regenerative capacity and skewed differentiation from HSCs leading to impaired blood production which is tailored in part by differential production of distinct HSC derived multi-potent progenitor subsets with specific myeloid or lymphoid lineage biases that in turn give rise to an array of lineage restricted progenitors, precursors and mature cells. So, the BM niche is comprised of many different cell types which described important age-related changes in individual niche components, specially in the vasculature (like fragilization of the vasculature), innervation, specific stromal populations as well as reported heightened inflammation in the aged marrow cavity particularly inflammatory remodeling of central marrow populations. In addition, HSC can bypass the intermediate steps to generate mature progenies under the conditions like aging and chronic inflammation. These changes create a self-reinforcing cycle of damage that drives lineage biases and regenerative response defects from the aged blood system which localized inflammation drives the constitutive activation of emergency myelopoiesis pathways particularly from old HSCs and MPPs, reinforcing myeloid cell production in the erythroid and lymphoid commitment expense. But the question, may niche alterations predispose to hematologic neoplasm in the situation? In response, during aging, remodeling of the BM endothelial vasculature is notable. So, on age related BM niche remodeling, the key micro-environmental players and their associated mechanisms with the HSC localization are very important. Supposedly, in MDS, abnormal cytokines production from the microenvironment, MSC and osteolineage cells dysfunction as well as vascular remodeling have been associated with the initiation and progression of disease. (figures 3 & 4) [1-3,14-20].

Figure 4: A model of the interplay between HSCs and the micro-environment during aging. The alterations in specialized niches might affect lymphoid/myeloid output directly and to accumulation of aged HSCs in the central BM and in the imbalanced mature HSCs production at particular niches might in turn remodel the micro-environment for these cells which can increase aged-related hematopoietic disorders incidence. [3]
In the end, aging is a heterogeneous process leading to impairment, malfunction as well as failure of cells and tissues. One of the hallmarks of aging relates to stem cell exhaustion which means aged HSCs have a diminished functional capacity while the increase number of HSCs seems to be a compensatory mechanism in order to maintain blood production. Another characteristic of aged HSCs is their distorted and skewed differentiation potential as well. Told all, in aging, after HSCs increased in number and impaired in functions which characterized by reduced regenerative and homing capacity, loss of cell polarity and myeloid biased differentiation at the expense of lymphopoiesis may be happened. These changes were thought initially to cause only cell-intrinsic deregulation like epigenetic deregulation, deficient DNA repair and replication stress. Also, old HSC suffer metabolic changes, impaired autophagy and altered protein hemostasis that contribute to their regenerative potential decline. [1-4,20-25,27]
Hematologic malignancies:
Many hematologic disorders including anemia and hematologic malignancies are more common with aging. So, compared with younger adults, older adults are more likely to have age related vulnerabilities such as functional and cognitive impairment. Therefore, the hematopoietic system is affected by this process in different ways such as clonal hematopoiesis (CH) with unexplained cytopenias which the progression to a myeloid cancer should be increased. But why? Because firstly, these patients with clonal cytopenia have a higher risk of developing a myeloid neoplasm significantly than those with no evidence of clonality. Secondly, morphologic evidence of dysplasia and MDS-specific cytogenetic abnormalities together which can be important in the malignant hematopoietic process. In summary, unexplained cytopenia is a rare hematologic disorder, while caution should be taken in unexplained cytopenia cases because the possible transformation of the disease to MDS or AML. Regarding this point, some researchers revealed a decreased survival in cases with CH as compared to cases without CH in unexplained cytopenia. In other report, specific ARCH mutations were identified among 64% of individuals with unexplained cytopenia and no history of any blood neoplasms but eventually many of these individuals suffered from myeloid malignancies as well.

Figure 5: Hypothetical model of evolution from age related clonal hematopoiesis to MBL (monoclonal B-cell lymphocytosis and CLL (chronic lymphocytic leukemia), although we know ARCH can find in some hematological malignancies like AML, CLL, MDS or others. But CLL is happened after third hit, not earlier than It. Why? [26]
It is noticeable that in some malignant hematopoietic diseases with normal genetic state, the concept of BM abnormality can be acceptable as the central and essential role, particularly on seizing in controlling of hematopoietic microenvironment pathway and their cellular functions and in the deregulation of hematopoietic pathway. [1-3, 15-17, 28-29].
Clonal hematopoiesis is a common trait of elderly persons in which blood cell populations are clonally derived from a single HSC or progenitor with acquired mutation. In fact, ARCH is a heterogeneous entity with a common feature including the expansion of specific HSCs and their progenitors. Several ARCH-related mutations can increase hematopoietic malignancy. Therefore, the clonal evolution suggests that the successive mutations accumulating in a given cell generate clonal outgrowths that thrive in response to micro-environmental selection pressures, dictating the phenotype of the malignancy which means the malignancy like myeloid malignancy defining the notion of CHIP. Anyhow, aging of the hematopoietic system might result from both HSC-intrinsic and micro-environmental alterations with changes in regulation, function and location of HSCs and their progeny, so this is a reason why the interconnections between these biological processes will be a key aspect in deciphering the extent of the impact of aging on HSC. Interestingly, the niche alterations are shared between aging and myeloid disorders associated with age which an important selection pressure to expand aberrant HSC clones which can go to hematopoietic malignancy. Thus, as a result, these actions can expand our understanding on the architecture of abnormal BM niche and its construction in aging particularly in changing to leukemic diseases (figures 4&5).
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
